Multiparameter flow cytometric immunophenotyping has become a powerful tool for ascertaining the ontogeny in B-cell lymphoproliferative disorders by virtue of its high throughput, low turnaround time and feasible logistics [1]. The advances in antibody engineering, in conjunction with the evolution of chemical conjugation techniques, has provided additional momentum for the widespread application of these probes in the simultaneous querying of the cell – surface expression patterns of a variety of cancer-related antigens. This makes multicolour flow cytometry pivotal for the neoplastic entities which require the use of a cocktail of markers for reaching a definitive diagnosis, as also to rule out the associated pathologies, a case in point being the differential diagnosis of chronic lymphocytic leukaemia (CLL).
A comprehensive diagnosis of CLL is essential to distinguish it from other lymphoproliferative disorders like hairy cell leukaemia or mantle cell lymphoma, as well as the risk stratification of the neoplasm, which is crucial in determining the therapeutic approaches which have to be followed. Furthermore, the presence of the aggressive disease forms in CLL lends special importance to the prognostic tests which are performed to assess the expression of the markers like CD38 and ZAP70 on the tumour cells, as these have been shown to have an impact on the disease response [2]. Moreover, the evaluation of novel treatment modalities like antibody therapy and stem cell transplantation needs a reiterative analysis of the marker expression on the cancer cells.
The diagnosis of CLL is based on an absolute increase in the lymphocytes (>5000/μL), the presence of small mature lymphocytes (narrow rim of the cytoplasm, a dense nucleus with no appreciable nucleoli and partially aggregated chromatin) [3] and a characteristic immunophenotype (CD5+,CD19+,CD23+, dim CD20, dim CD79b, dim sIg and FMC7) [4]. As has been mentioned earlier, the differential diagnosis of CLL from other lymphoproliferative disorders, is accomplished mainly on the basis of the patterns of the antigen co-expression or its lack thereof, to arrive at a conclusive diagnosis. For example, CLL differs from Mantle Cell Lymphoma (MCL) on the basis of the expression of CD23 and the lack of expression of CD22.
Given the cost optimisation scenario which has been observed in recent years in the medical care industry, the decision to invest in an appropriate antibody panel that would enable an accurate diagnosis at reasonable costs is a crucial one. Numerous studies have investigated the utility of the different markers and their combinations in differentially diagnosing lymphoproliferative disorders [5–7]. These studies were mostly aimed at establishing the independence of the staining intensity of the markers in diagnosing CLL, thereby reducing the redundancies in the panel components [8,9]. The Indian economic setting sometimes makes the cost management even more pressing; creating the need to develop basic minimal panels which have to be used, to reach a workable diagnosis. The present study consisted of the evaluation of an antibody panel for the diagnosis of CLL and the stratification of CLPD in the patients who were getting treatment at a super – specialty cancer hospital.
Material and Methods
Patients
This study was based on the newly diagnosed cases of CLPD in a multispecialty oncology hospital, as well as on the preliminary diagnosed CLPD cases which were referred to the same between November 2008 and December 2011. The final diagnoses in all the cases were based on a multifactorial assessment of the available clinical data, the morphologic findings, the immunophenotyping results and cytogenetics. These studies were conducted on the specimens of EDTA – peripheral blood and bone marrow. The heparinised samples were used for cytogenetics. All the samples were collected with aseptic precautions in minor operating theatre conditions under local anaesthesia, after giving a test dose of xylocaine. Since all the samples were received as a part of the diagnostic workup for the clinician, informed consents were obtained by the clinician in all the cases.
Morphology
The peripheral blood smears and the bone marrow aspirate smears were air – dried and stained with the Leishman stain and the May – Grunwald Giemsa stain respectively. Previously established guidelines [10] were used to categorize the cases as typical CLL or Prolymphocytic Leukaemia (PLL), based on the haematopathological picture. In all the cases, the peripheral blood showed a lymphocytosis of greater than 5x109/L for least 3 months. Typically, CLL is characterised by small cells with scant cytoplasm, round nuclei, condensed chromatin and inconspicuous nucleoli. Smudge cells or basket cells are typically seen in the peripheral blood smears. The cases which had the numbers of the prolymphocytes ranging between >10% and <55% among the lymphocytes, were designated as CLL. The prolymphocytes were identified as the larger cells with prominent nucleoli. A distinction was not made between the cases which were designated as PLL with a stable number of prolymphocytes and the cases with temporally increasing numbers of prolymphocytes.
Immunophenotyping with the use of flow cytometry
All the antibodies were purchased from Beckman Coulter, India (Mumbai, India). The primary panel of the monoclonal antibodies included CD45 (leucocyte common antigen), CD10 (Common Acute Lymphoblastic Leukaemia Antigen-CALLA), CD5, CD19, CD20, CD23, FMC7 and CD79b. The additional markers which were used were CD3 (to exclude T-cell tumours), CD22 (to rule out B-proliferative disorders), CD25 and CD103 (to rule out Hairy Cell Leukaemia), CD 38 and ZAP70 (for prognostication), kappa and lambda (for clonality assignation). Briefly, the blood or bone marrow samples were incubated with the relevant antibodies for 30 min at room temperature before being washed twice with phosphate buffered saline (pH 7.4). All the samples were then analysed on a Dako CyAn ADP instrument and a minimum of 10,000 total events was acquired for each analysis. The data were analyzed by using the SUMMIT® software (version 5.4). The sample positivity was based on a finding of ≥ 20 % cells which expressed a particular antigen. Further, the expression levels of the individual antigens were described as strong, moderate, and dim, depending on the order of the magnitude by which the fluorescence intensity with their cognate antibodies was higher than the corresponding isotype controls. A 1.5 log increment was considered to be a strong antigen expression, an increment between 1 and 1.5 logs was considered as a moderate antigen expression and an increment below 1 log was representative of a weak or a negative antigen expression [11,12].
Cytogenetic analysis
All the reagents for the cytogenetic studies were obtained from Invitrogen, Bangalore, India. The studies were performed by initiating short-term (Direct, 24 h and 48 h) unstimulated cultures from the fresh bone marrow aspirates (BMA) in RPMI 1640 which was supplemented with L – Glutamine, 20% fetal bovine serum and penicillin-streptomycin. The cultures were exposed to colcemid (0.01 mg/ml) for 25 minutes before being harvested by hypotonic treatment in 75 mM KCl and by repeated fixations in a 3:1 mixture of methanol and acetic acid. The slides were incubated at 60° C for 1 day and they were then G – banded with trypsin and the Giemsa (NICE) stain. Twenty metaphases were analysed and each karyotype was named according to the International Human Chromosomes Nomenclature. The Fluorescent In Situ Hybridization (FISH) assay was carried out according to the manufacturer’s instructions by using a panel of seven probes which included 13q14/p53 (17p13), 11q22/GLI 12q13, 6q21/8q24 C-myc and the LSI IGH gene break apart (MP Biomedical LLC, Mumbai), India. In brief, the sample was washed in phosphate buffered saline (PBS) and it was fixed by using Carnoy’s fixative. The fixed cell suspension was then applied on microscopic slides and the area for adding the probe was marked. Following the addition of the probe, the slide was heated to 75° C for denaturation on a Thermobrite (Abbott Laboratories, Mumbai), India for 2 minutes and it was then maintained at 37° C overnight for hybridisation. After the post – hybridisation washes, the slide was counterstained with 4’, 6 – diamidino – 2– phenylindole (DAPI). At least 200 cells were counted under a fluorescence microscope for each combination of the probe set.
Statistical Methods
The statistical analysis was performed by using the SPSS 11.5 software and it consisted of applying ANOVA for the parametric data and the Chi-square or the Kruskal-Wallis tests for the non-parametric data. The analysis was aimed at evaluating the significant differences in the absolute lymphocyte counts and the expression of the cell markers among various categories. A p value of <0.05 was considered as significant.
Results
Demographics
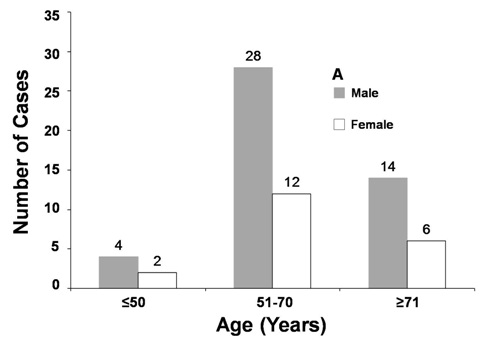
A total of 66 cases of CLPD were analysed, out of which six (9%) were ≥50 years, 40 (60.6%) were between 51-70 years and 20 (30.3%) were >70 years. The overall median age was 64.5 years and the age range was from 43-84 years. Out of the 66 cases, 46 (69.6%) cases were males and 20 (30.3%) were females, with a male to female ratio of 2.3:1. Out of the six cases which were ≥50 years, 4 (66.6%) were males and two (33.3%) were females, with a sex ratio of 2:1. Among the 51-70 year age group, there were 28 (70%) males and 12 (30%) female patients with a sex ratio of 2.3:1. Out of the 22 cases which were >70 years, 14 (70%) were males and 6 (30%) were females, with a male to female ratio of 2.3:1. [Table/Fig-1A] shows the relevant demographic distribution. As the graph depicts, a majority of the cases were seen to occur between 51-70 years of age. A total of 40 cases of CLL were recorded, while a typical CLL cases were observed [9]. The remaining 17 cases were classified as CLPD and they included 13 cases of Non-Hodgkin’s Lymphoma (NHL), two cases of HCL, one case of FL and one case of PLL.
Classification of CLPD cases by sex and age
Morphologic Evaluation
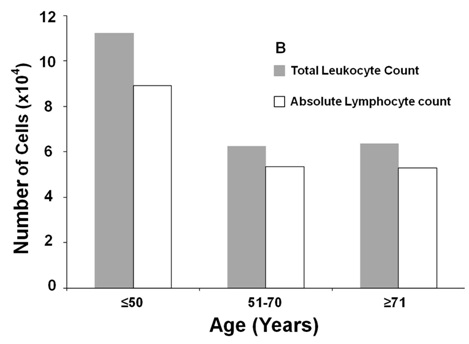
The review of the morphology which was concurrent with the immunophenotypic analysis by flow cytometry, was done in all the cases by two pathologists. The morphologic categorisation as CLL, CLL/PLL or CLPD was done in 66 cases, based on the microscopic appearance of the peripheral blood smears or the bone marrow aspirates, along with the absolute lymphocyte counts (>5000 cells/ μL). [Table/Fig-1B] shows the average total lymphocyte counts across the different age brackets. There was no significant association of the mean absolute lymphocyte counts with any categorical group. Apart from two cases being suspected of being Hairy Cell Leukaemia (HCL) and one case being suspected of being PLL, all the other cases were categorized as CLL, based on the preponderance of the small mature lymphocytes in the smears. The characteristic smudge cells were also observed in these cases [Table/Fig-2A & 2B].
Median leukocyte counts of CLPD cases distributed based on age groups
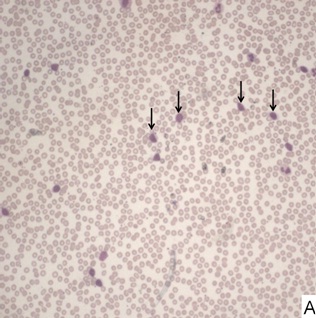
Low power field of a blood smear stained with Leishman stain showing a preponderance of mature lymphocytes with small round nuclei and distinct clumped chromatin which is characteristic of CLL (arrow). Few smudge cells are commonly seen
High power view of a small mature lymphocyte (arrow) in a peripheral blood smear showing characteristic scant cytoplasm, round nuclei, condensed chromatin and inconspicuous nucleoli

Cytogenetics
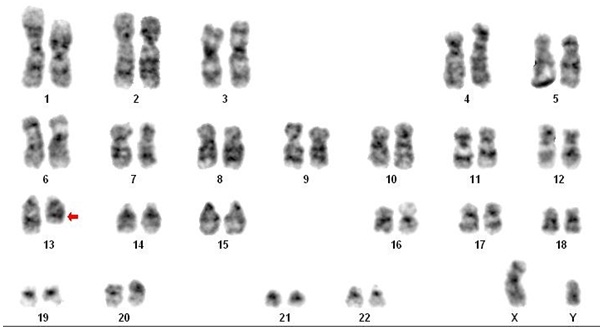
Karyotyping and FISH were done in 15 of the 66 CLPD cases, of which 3 (20%) showed abnormalities. One case demonstrated the abnormality, t (14; 18) (q32; q21), which is the characteristic of 80-90% follicular lymphomas [13]. The diagnosis was further supported by the morphological picture and the immunophenotypic status of CD5- and CD10+ [14]. Another case demonstrated a del (13) abnormality [Table/Fig-3] which is a characteristic of CLL [15]. The third case had trisomy 12q, which is the most common abnormality in CLL [16].
Karyotyping results from a CLL case showing the characteristic cytogenetic lesion del(13) indicated by the arrow
Immunophenotyping
The diagnostic criteria that we used for classifying the cases, based on their immunophenotypes, has been outlined in [Table/Fig-4].The immunophenotypic profiles of the various CLPD cases have been listed in [Table/Fig-5]. All the 66 cases demonstrated a population of B lymphocytes (CD19+). Of the 40 CLL cases, all but two cases showed positivity for the co-expression of CD5 and CD23. Representative histograms from a typical CLL case are shown in [Table/Fig-6]. The two samples were negative for CD5, which has been observed by others also [17]. CD3 was positive in 4 cases (10%) and CD10 was positive in two cases (5%). However, the morphological criteria overruled the immunophenotypic relegation of these cases as atypical forms or other CLPDs. CD38 and ZAP70 were positive in 16 and 9 cases (40% and 22.5%) respectively. All the atypical CLLs showed positivity for CD22, with two cases being negative for CD5. Of the 17 cases which were classified as CLPD, one was a follicular lymphoma with a characteristic immunophenotype of CD5- and CD10+. The sole PLL case had an immunophenotype of CD5-, CD23+, and CD22+. Two hairy cell leukaemias (HCL) were CD5-, CD23-, CD22+,CD25+ and CD103+. Of the remaining CLPD cases, six were positive for CD5, two were positive for CD23 and one each was CD3+ and CD10+. The limitations of our antibody panel precluded a more definitive diagnosis and such cases were advised confirmation through an immunohistochemical analysis of the lymph node biopsies with an appropriate panel.
Immunophenotypic diagnostic criteria for CLPD
| CD 19 | CD 5 | CD 23 | CD 20 | CD 22 | FMC 7 | CD 79b | CD 10 | CD 3 | CD 25 | CD 103 |
|---|
| CLL | + | + | + | + | - | -/(+) | -/(+) | - | - | - | - |
| MCL | + | + | - | + | + | + | + | - | - | - | - |
| HCL | + | - | - | + | + | + | + | - | - | + | + |
| FL | + | - | - | + | + | - | + | + | - | - | - |
| PLL | + | ± | ± | + | + | + | + | - | - | - | - |
Abbreviations: CLL = chronic lymphocytic leukemia; MCL = mantle cell lymphoma; HCL = hairy cell leukemia; FL = follicular lymphoma; PLL = prolymphocytic leukemia. Symbols: –/(+) - negative/weakly positive; ± - negative in majority of cases
Immunophenotypic diagnostic criteria for CLPD
| Antigen | CLL (Positive/Total) | Atypical CLL (Positive/Total) | CLPD (Positive/Total) |
|---|
| CD3 | 4/40 | 0/9 | 1/17 |
| CD5 | 38/40 | 2/9 | 6/17 |
| CD10 | 2/40 | 0/9 | 2/17 |
| CD19 | 40/40 | 9/9 | 17/17 |
| CD20 | 34/40 | 9/9 | 17/17 |
| CD22 | 0/40 | 9/9 | 16/17 |
| CD23 | 40/40 | 9/9 | 4/17 |
| CD25 | 0/40 | 0/9 | 2/17 |
| CD103 | 0/40 | 0/9 | 2/17 |
| CD38 | 16/40 | 1/9 | 11/17 |
| ZAP70 | 9/40 | 0/9 | 4/17 |
| CD79b | 23/40 | 3/9 | 11/17 |
| FMC7 | 5/40 | 2/9 | 9/17 |
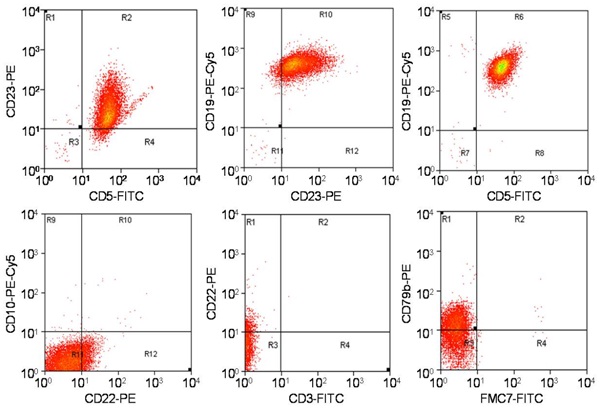
Immunophenotypic profile on flow cytometry of a CLL case. Note positivity of CD5, CD19, CD23, negativity of CD22 and FMC7 markers. Partial positivity is observed in CD22 and CD79b panels. FITC-Fluorescein isothiocyanate, PE-Phycoerythrin, Cy5- Cyanine 5
CD20 was expressed on 34 (85%) CLL cases, whereas CD79b and FMC7 were expressed on 23 (57.5%) and 5 (12.5%) cases respectively. Overall, the CD20 expression was constitutive in the atypical CLL and the CLPD cases, whereas the expressions of CD79b and FMC7 were consistently higher in the atypical CLL and the CLPD cases (p = 0.005). The correlations between the expressions of the individual markers and their diagnoses were studied. The lack of expression of CD22 had the highest correlation with a definitive diagnosis of CLL (r2= –0.97, P=0.000). The correlations of the expressions of CD5 (r2= 0.68, P=0.000) and CD23 (r2= 0.61, P=0.000) were also significant. We also correlated the expression of CD23 with those of CD20, FMC7 and CD79b. There was no significant correlation of CD23 with either CD20 or CD79b, but there was a significant negative correlation between the expressions of CD23 and FMC7 (r2= –0.52,P=0.000). A similar analysis with CD5 as a variable did not yield any significant correlations.
Discussion
The identification and the classification of Chronic Lymphoproliferative Disorders (CLPDs) is critical for the patient stratification, risk assessment and the treatment planning. An accurate diagnosis of CLPD poses numerous challenges and it has to be achieved by a combinatorial diagnostic approach which includes the morphologic examination, the surface marker expression profiling and cytogenetics. Cytogenetics may often be difficult in these cases due to the failure of the tumour cells to grow in culture, whereas the morphology alone is not considered as diagnostic. Given this scenario, a flow cytometry based immunophenotyping plays a crucial role in the sub – typing of CLPD. Furthermore, the surface marker expression is important for the prognostic evaluation, as also, for the following disease transformation/development after the therapy. The choice of the immunophenotypic panels that would provide the highest information at the least cost has come to occupy the vanguard of the research questions that are faced by diagnostic laboratories. The panel concordance between hospitals is variable, depending on the care that is given, the patient sections which are treated and the individual choice of the pathologist. However, it is imperative to have a basic minimal panel that would enable an accurate diagnosis in a majority of the cases and a provisional diagnosis in the remaining numbers. We have, in this study, evaluated a panel for its ability to diagnose CLL and to categorise CLPD in a tertiary cancer care centre and we simultaneously studied the epidemiological patterns of the occurrence of CLL.
Chronic lymphocytic leukaemia (CLL) accounts for nearly 30% of all leukaemias, thus making it a frequent lymphoid malignancy [18]. The disease is mostly observed in elderly people, with the incidence increasing rapidly with the age. The highest incidence is seen in the age group of 75 – 84 years, with the median age at diagnosis being 72 years [19]. In our study, the maximum incidence was in the age group of 51 – 70 years, with the median being 64.5 years. This variation could have been due to the small number of cases that were studied or due to the ethnic differences. Although, Gogia et al., reported a median age of 59 years from a large series study in India [20], which enhanced the basis of the ethnic variations in epidemiology. Indeed, the earlier epidemiological studies have emphasized the importance of the racial and genetic influences in the development of the disease [21, 22]. Furthermore, a recent study demonstrated a poorer prognosis for CLL in the Indian populations, due to higher numbers of the T regulatory cells [23], which further reinforces the concept of the ethnic variations in the CLL incidence and progression. According to the Surveillance, Epidemiology and End Results (SEER) database, CLL occurs approximately twice as commonly in males as in females [24]. This ratio or a proximate one, was maintained in our study population across all the age groups, as was seen in Gogia’s study [20].
The morphological evaluation which remains a key determinant in the diagnosis, did not present any differences from the afore-described haematopathological picture. With regards to immunophenotyping, our basic panel could diagnose CLL in almost all the cases, with the best correlation being seen with the lack of expression of CD22. The positivities of CD5 and CD23 was also significantly correlated with the diagnosis. We could narrow down the diagnosis in three CLPD cases as follicular lymphoma (1 case) and hairy cell leukaemia (2 cases) with our panel; however, this was not possible with the other cases. The follicular lymphoma diagnosis was supported by the cytogenetic finding of a characteristic translocation. The expressions of CD20, FMC7 and CD79b showed that their expressions were consistently higher in the non-CLL cases, although this difference was significant only with the FMC7 marker. These results led us to believe that the use of CD20 may be redundant in a basic panel. Earlier studies have demonstrated the importance of the CD23 and the FMC7 co-expression [5, 7]. Our analysis showed that the expression of CD23 was not found in the cases with a positive FMC7 expression and vice versa. The clinical significance of this association could not be evaluated due to the lack of a clinical follow – up.
The ability of our panel to accurately detect CLL in the patient samples, led us to believe that a basic minimal panel (which consisted of CD45, CD20, CD22, CD79b, CD19, CD5, CD23, CD10, FMC7, CD3, CD5, CD25, CD103, kappa and lambda) was sufficient for the routine diagnosis of CLL. However, the stratification of CLPD requires the use of more extensive panels. Based on these results, we recommend the initiation of immunophenotyping with a basic panel and then expanding the repertoire as the circumstance calls for.