The pancreas is a mixed exocrine-endocrine gland, with the exocrine portion of the gland making up the greatest volume (84%). Ductal cells and blood vessels make up around 4% of the volume, while the endocrine part makes up 2% of the volume. The other part (10%) is occupied by an extracellular matrix. The acinar tissue in the pancreas is in the close vicinity of the islets. Because of this close morphological relationship, functional interactions are likely to occur between the exocrine and endocrine pancreas in any disease, which affect this organ [1].
Anatomically, the blood from the islets bathes the acinar cells by way of an islet-exocrine portal system [2]. There is also morphological evidence that indicates that the pancreatic exocrine function may be influenced by the pancreatic endocrine hormones. Insulin has a trophic effect on the exocrine pancreas, especially on the peri-insular acini. A progressive damage to the pancreatic acinar cells is seen in insulin deficiency. The pancreatic exocrine tissue in a diabetic patient becomes fibrosed and it shows a reduced response to the hormonal stimulation [2].
In type 2 Diabetes mellitus, the continuous interstitial matrix connection between the endocrine and the exocrine pancreas is lost in animal models and humans, which results in a dysfunctional insulino-acinar-ductal-incretin gut hormonal axis [3]. Besides these putative mechanisms, there are multiple defects in the insulin secretion and the signalling in type 2 diabetes, which may affect the enzyme synthesis and release in the exocrine pancreas [4]. Not only this, also, the secretion of the pancreatic juice is controlled by the autonomic nervous system and by the naturally occurring gut hormones, cholecystokinin and secretin. This complex interplay is often found to be disturbed in diabetes due to the well-known complications of autonomic neuropathy and the microvascular complications, which are so common in Diabetes mellitus [1].
With this background, the present study was conducted in order to elucidate a possible correlation between the functional entities of the pancreas.
Material and Methods
This study was conducted in the Department of Clinical Biochemistry, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi for a period of six months. 110 patients of type 2 Diabetes mellitus who were already diagnosed and were taking treatment were included in this study. These patients were visiting the hospital for follow up check-ups from time to time. An inclusion criterion for them was males and females with type 2 Diabetes mellitus with or without complications or any co-morbid conditions like hypertension, coronary artery disease, etc. 30 non-diabetic healthy individuals who visited the hospital for medical check-ups in the general out-patients department were considered as the controls. All the subjects, including the controls, were fully informed about the study and their voluntary informed consents were taken.
Fasting venous blood was collected from the cases (diabetic patients) as well as the controls (healthy subjects), it was centrifuged and the plasma/serum was separated for analysis on the same day for the blood glucose, the lipid profile which included the estimation of serum triglycerides, total cholesterol, high density lipoprotein (HDL), low density lipoprotein (LDL) and the serum amylase activity as per the routine procedure which was followed in the department.
The sample analysis was carried out on a fully automated analyser by using different reagent kits as per the procedure which was defined by the manufacturer. The estimation of fasting blood glucose was done by the glucose oxidase–peroxidase method. The serum triglycerides were measured by the enzymatic (GPO-PAP) method. For the determination of the total cholesterol, an enzymatic (CHOD-PAP) colourimetric method was used. The direct measurements for LDL and HDL were done by using enzymatic methods. The amylase activity was measured by a photometric enzymatic method.
The results were analysed statistically by using the Student’s “t”test and correlation coefficients on the suitable software. P values of <0.05 were considered as statistically significant.
Results
Diabetes is a global problem and with an increasing incidence worldwide, it would be the leading cause of morbidity and mortality in the future. Diabetes is invariably associated with a derangement in the functions of the pancreas.
The pancreas has dual functions in our body, as a digestive organ and as an endocrine organ. To evaluate this complex relationship between the two functional entities of this organ, the present study was conducted. 110 known cases of Type 2 diabetes (group I, n=110) and 30 controls, [group II, n=30 (healthy subjects)] were considered to assess the possible exocrine-endocrine relationship of the pancreas, by evaluating the serum amylase levels and the blood glucose in the two groups. The other biochemical parameters like the lipid profiles of the cases were compared with those of the healthy controls and they were also correlated with the amylase activities in the two groups. The following were the findings of this case-control study.
The clinical characteristics of the study subjects have been shown in [Table/Fig-1]. The mean ages among the two groups were comparable and the difference was not significant, being 53.41±10.48 years in the diabetic patients group and 50.15±5.58 years in the healthy control group. There were 67 males and 43 females in group I, against a comparable ratio in group II i.e. 18 males and 12 females.
Clinical characteristics of the study subjects.
| Characteristics of the subjects | Group I Cases n=110 | Group II Controls n=30 | p value |
|---|
| Age (years) | 53.41 ± 10.48 | 50.15 ± 5.58 | Not significant |
| Sex (males: females) | 67:43 | 18:12 | Not significant |
| Fasting blood glucose (mg/dl) | 154.41 ± 42.93 | 82.85 ± 9.92 | <0.001 |
| Serum Triglycerides (mg/dl) | 168.7 ± 67.25 | 88.1 ± 38.57 | <0.001 |
| Total cholesterol (mg/dl) | 172.6 ± 31.84 | 150.5 ± 25.25 | <0.05 |
| High density lipoproteins (HDL )(mg/dl) | 37.74 ± 6.29 | 43.45 ± 8.7 | <0.05 |
| Low density lipoproteins (LDL) (mg/dl) | 116.07 ± 27.13 | 90.35 ± 25.89 | <0.001 |
| Total cholesterol/HDL ratio | 4.67 ± 0.9 | 3.53 ± 0.81 | <0.001 |
| Serum amylase (U/L) | 48.13 ± 9.16 | 73.9 ± 23.1 | <0.001 |
The serum amylase activity was found to be significantly lower in the cases (group I, n=110) as compared to that in the controls (group II, n=30) with a p value of <0.001. On comparing the other biochemical parameters like the fasting total cholesterol, triglycerides and LDL among the two groups, it was found that these were significantly higher in the cases as compared to those in the controls, with p values of <0.05, <0.001 and <0.001 respectively. However, the cardio-metabolic protective factors like HDL and the Chol/HDL ratio were found to be lower in the diabetic subjects (cases) as compared to those in the healthy controls with p values of <0.001. This further consolidated the well-known risk of the cardio-metabolic abnormalities and the dyslipidaemia in the diabetic individuals.
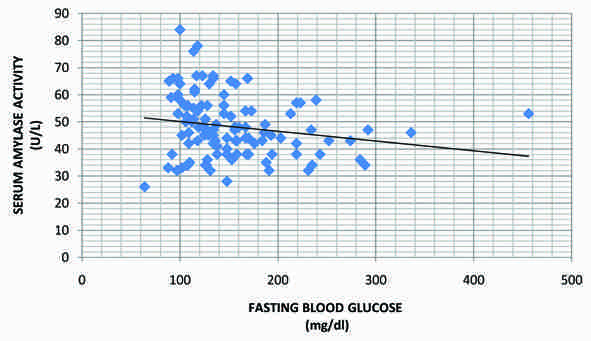
Interestingly, there was a significant (p value <0.05) negative correlation between the serum amylase activity and the fasting blood glucose levels in the diabetic patients (Pearson’s correlation coefficient, r= -0.185) [Table/Fig-2 and 3].
Correlation of the serum amylase levels with the blood glucose and the lipid profile (serum triglycerides, total cholesterol, HDL, LDL and total cholesterol/HDL ratio) of the diabetic patients (group I) (N.S.= not significant)
| Correlation of serum amylase with: | Pearson’s correlation co-efficient (r) | p-value |
|---|
| Fasting blood glucose | -0.185 | <0.05 |
| Serum triglycerides | -0.102 | N.S. |
| Total cholesterol | -0.190 | N.S. |
| HDL | 0.214 | <0.05 |
| LDL | -0.080 | N.S. |
| Chol/HDL ratio | -0.304 | N.S. |
Correlation of serum amylase with fasting blood glucose in diabetic patients showing a negative correlation (r=-0.185).
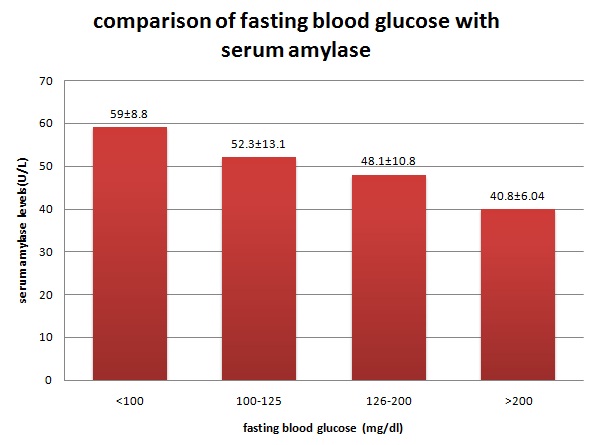
Therefore, the patients with poorly controlled diabetes had lower serum amylase activities as compared to the ones with a good control on their diabetes [Table/Fig-4].
Comparison of fasting blood glucose levels with serum amylase levels in the diabetic patients (group I)
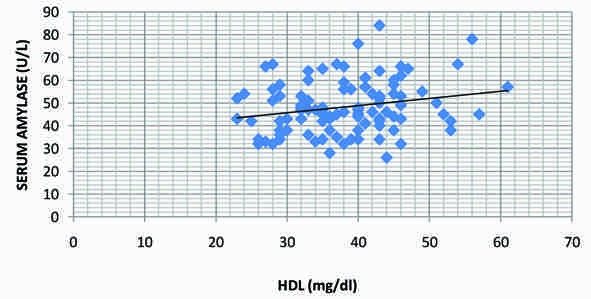
However, the correlation of the serum amylase activity with the serum triglycerides, total cholesterol and the LDL in the diabetic group was not found to be significant [Table/Fig-2]. On the contrary, the HDL levels were significantly (p value of <0.05) positively correlated with the serum amylase activity in the diabetic group (Pearson’s correlation coefficient r= 0.214). Thus, the patients with low HDL levels also had low serum amylase levels [Table/Fig-5].
Correlation of serum amylase with HDL levels in diabetic patients showing a positive correlation (r=0.214).
Discussion
The human exocrine pancreatic secretions are affected in the diseases which affect the pancreas . The low serum amylase levels in diabetes may reflect the impaired exocrine-endocrine interactions of the pancreas. However, only few clinical studies have addressed this complex relationship.
In our study, we found a significantly low amylase activity in the diabetic patients as compared to that in the healthy subjects. Several animal and cellular studies have tried to find out the pathogenic features and the underlying mechanisms which link the islet cells and the acinar cells [1]. But, the estimation of the serum levels of amylase along with the blood glucose to assess this relationship, consolidates its clinical relevance in humans.
There is evidence that the pancreatic hormones, insulin and glucagon, influence the enzyme synthesis and release in the exocrine pancreas. Insulin has a trophic effect on the acinar cells, whereas glucagon has been found to have an inhibitory influence on the exocrine secretions and moreover, there is a decrease in the sensitivity of the diabetic pancreatic acini to secretagogues [1]. So, the insulin deficiency and the glucagon excess in diabetes affect the normal milieu of the pancreas, thereby decreasing the total volume, the amylase secretions and the bicarbonate content of its exocrine secretions [1].
Our results suggest that the low serum amylase levels in diabetes are associated with an impaired insulin action due to insulin resistance and/or inadequate insulin secretion, as was indicated by the raised blood glucose levels in our study.
Moreover about 50% of the diabetics have been found to have pancreatic fibrosis and pathological findings such as atrophy, fatty infiltration and loss of the exocrine acinar cells [5–9].
Also, diabetic neuropathy may lead to impaired entero-pancreatic reflexes and exocrine dysfunction [10]. Elevated hormones and peptide concentrations (glucagon, pancreatic polypeptide P, somatostatin) may suppress the exocrine function [11–15]. Recently, it has been added that cytokines such as TGF-beta 1, TGF-alpha (transforming growth factors) and TNF-alpha (tumour necrosis factor), gastrin and low regulatory gene functions may interact and further impair the exocrine and endocrine functions [16–18].
However, some of the previous studies had conflicting results, especially in the patients of Type 1 diabetes, where an increase in the serum amylase levels was found. In Type 1 diabetes, the clinical and the pathological pictures are different, with the presence of insulitis and the diffuse lymphocytic infiltration of the exocrine pancreas. Moreover, it has been characterized as an organ-specific autoimmune disease. Also, this increment in the serum amylase levels as compared to those in the controls was more pronounced in the patients of Type 1 diabetes who presented with acute fulminant ketoacidosis [19–24].
Since diabetes is a multifactorial disorder, apart from the major pancreatic hormones, an interplay between a number of other factors play an important role in the carbohydrate, protein and lipid metabolisms. Hypercholesterolaemia and hypertriglyceridaemia are mostly observed and they are related largely to the degree of the diabetic control [25]. Hyperglycaemia may alter the lipoproteins to a form that promotes atherogenesis. Dyslipidaemia, which is characterized by raised triglycerides, low HDL and high small dense LDL particles, is very frequently seen in diabetes. This contributes to the risk of coronary artery disease in these patients and the determination of the serum lipid profile in the patients of diabetes is now considered as a standard of the diabetic care [26,27]. In our study also, we found a dyslipidaemic picture of the lipid profile in the diabetic patients as compared to that in the healthy controls. However, adding a new dimension to this, is our finding of the significant positive correlation of the HDL levels with the serum amylase levels in the diabetes patients. So, it may be considered that the serum amylase may act similar to the well-known cardiometabolic protective factor, HDL.
Apart from all this, an estimation of the serum insulin levels, along with the measurement of the other pancreatic enzymes e.g. lipase, would be able to put an insight into the possible endocrine-exocrine relationship of the pancreas in the patients of diabetes.
In conclusion, our study demonstrated that low serum amylase levels are associated with Type 2 diabetes, thus suggesting a possible exocrine-endocrine relationship in this disease. However, its role as a valuable marker in various other clinical conditions of the pancreas remains to be elucidated.