Chronic obstructive pulmonary disease (COPD), as was defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD), is a disease state which is characterized by an airflow limitation that is not fully reversible. COPD includes chronic bronchitis, peripheral bronchiolitis and emphysema [1]. The most important risk factor for the development of COPD is cigarette smoking. In India, a daily cigarette smoker smokes an average of 6.2 cigarette sticks and a bidi smoker smokes 11.6 bidi sticks per day. Smoking bidis (hand rolled Indian cigarettes) is also implicated in the pathogenesis of COPD.
Identifying the key components in the pathogenesis of COPD is paramount, as the therapy which targets these components might provide substantial clinical benefit. Three key processes have been identified in the pathogenesis of COPD: oxidative tissue damage, protease- mediated tissue destruction, and leukocyte-driven chronic inflammation [2]. These could be mediated by the T cells. The T cells are lymphocytes which mature in the thymus, which contribute to an acquired immunity. The T-cell receptor (TCR) which is present, in association with CD3, determines the specificity of the T cell. Following the T-cell maturation in the thymus, with regards to the TCR specificity and the CD4+/CD8+ subtype, they are released into the peripheral circulation and then, they are transported to various tissues in search for their specific antigen. The CD4+ T-cells are the helper cells, while the CD8+ T cells are cytotoxic cells. For example, the CD8+ T cells are could cause apoptosis and thus, the destruction of the lung parenchyma. Abnormalities of the T-lymphocyte subsets in the peripheral blood and in bronchoalveolar lavage (BAL), as well as increased neutrophils, macrophages and CD8+ T lymphocytes in the airways, have been reported in patients with COPD. The T-cell mediated abnormal intrapulmonary inflammation persists even after the cessation of smoking and it has been identified as a key component in the development and the progression of COPD [3,4]. The increase in the T-cell populations in the lung could possibly be caused by the movement of these cells from the blood to the lung tissues, or it could be the result of the de novo differentiation and proliferation within the lung. The T cells may respond to an antigenic stimulus which is induced by cigarette smoking, and it may thus result in the development and the progression of COPD. If that were the case, COPD could be considered as an autoimmune disease which was triggered by smoking [5].
Thus, the studies which are done on the T-cell populations in the peripheral blood may add valuable information about their recruitment to the lung and their roles in the COPD pathogenesis. It may also throw light on the development of newer modalities of therapy which target the recruitment and the protease production by the macrophages and the neutrophils in COPD. Also, whether bidi smoking elicits a similar inflammatory response in the lung, needs to be sought, as most of the studies are conducted among cigarette smokers.
MATERIALS AND METHODS
The study design
This was a case control study. Sixty male patients who were aged above 40 years, who attended the outpatients department or were admitted in the Father Muller Medical College Hospital were included in this study. Twenty one male patients who were diagnosed to have COPD and 19 AS and 20 HNS subjects were included in the study by using a purposive sampling technique. The never smokers without any respiratory symptoms/airflow limitations were included in the HNS group. The current smokers without any respiratory symptoms or airflow limitations were included as the AS, and those smokers with respiratory symptoms and/or airflow limitations were included as the patients with COPD. None of the subjects had a documented tuberculosis or HIV infection, nor were they receiving oral corticosteroids or immunosuppressive treatment. However, one apparently asymptomatic smoker was found to have an airflow limitation on spirometry and he was therefore included among the smokers with COPD. The COPD group had a history of cough with sputum production and/or dyspnoea on most of the days of the month, for at least 3 months a year, for a period of minimum 2 consecutive years before the study and/or an airflow limitation on spirometry (FEV1/FVC < 70% and FEV1 < 80% of predicted normal). The patients with respiratory failure and cor pulmonale or an SpO2 of < 88% on room air, those with a history of bronchial asthma, HIV infection and tuberculosis and those who received immunosuppressive treatment were excluded from the study.
Ethical approval: The study protocol was approved by the ethics committee, and informed consents were obtained from all the subjects.
The period of the study: Two years (2009 to 2011).
The method of collection of the data
Twenty one COPD patients who fulfilled the GOLD criteria, 19 AS with normal lung functions and 20 HNS were included in the study. Following a detailed history taking, clinical examinations, pulse oximetry and laboratory investigations which included a complete blood count, screening for HIV, chest X-ray and spirometry were done. The lung volumes and the flow rates were measured according to the recommendations of the American Thoracic Society (ATS). The forced expiratory volume in the first second (FEV1) in litres and the forced vital capacity (FVC) in litres were measured and the FEV1/FVC ratio was calculated.
Five ml of peripheral venous blood was collected in heparinized vacutainer tubes from all the participants of the study, at their initial presentations to the hospital. The blood was stored at a temperature of 20-25°C until a cell count analysis was performed within 24 hours, by using an automated differential cell counter and a flowcytometry system (BD FACS CaliburTM system, USA) at Manipal Life Sciences Center, Manipal University. The CD4+T-cell and the CD8+T-cell counts (cells/μl) were measured and the CD4+/CD8+ ratio was calculated.
The data was collected for the three groups: Group COPD (FEV1/FVC < 70%). The patients in this group were classified, based on the FEV1 values. (< 80% as mild COPD, 50-80% as moderate COPD, 30-50% as severe COPD and < 30% as very severe COPD), according to the GOLD standards.
Group AS (FEV1/FVC > 70%)
The subjects with smoking habits which matched those of the COPD group but without airflow limitations.
Group HNS
Non-smoking healthy subjects.
DATA - ANALYSIS
The data was analyzed for the significant differences in the CD4+ T-cell and CD8+ T-cell counts in the three groups by using the One-way Analysis Of Variance (ANOVA). The results were reported as mean + SD. The comparisons between the groups were made by using the Mann-Whitney U test or the Kruskal-Wallis test. Spearman’s rank correlation was used to determine as to how the T-lymphocyte subsets correlated with the pulmonary function tests in the 3 groups of subjects. All the statistical analyses were performed by using the software, SPSS, version 13; p values of < 0.05 were considered as significant.
RESULTS
The study population
The study population consisted of 20 HNS, 19 AS, and 21 smokers with respiratory symptoms and/or airflow limitations (smokers with COPD). All the subjects were men (mean + SD age, 53.3+10.6 years, 57.7+9.4 years, and 58+12.8 years for HNS, AS and COPD respectively) [Table/Fig-1].
Demographic data of the subjects participating in the study
| Variables | Healthy non-smokers (n=20) | Asymptomatic smokers (n=19) | COPD (n=21) | p value |
|---|
| Age, yrs | 53.3±10.6 | 57.7±9.4 | 58±12.8 | 0.326 NS |
| Smoking, pack yrs | 0 | 22.2±11.6 | 45.1±36.3 | 0.012 S |
| FVC, % predicted | 92.7±15.2 | 97.2±17.9 | 69.8±16.7 | 0.000 HS |
| FEV1, % predicted | 89±10.6 | 98.7±17.6 | 47.5±16.9 | 0.000 HS |
| FEV1/FVC,% | 80.7±6.2 | 81.5±4.9 | 53.1±13.3 | 0.000 HS |
| BMI (kg/m2) | 23.7±4.0 | 23±4.3 | 19.1±4.8 | 0.003 HS |
The mean smoking history was 22.2+11.6 pack-years for the asymptomatic smokers and it was 45.1+36.3 pack-years for the smokers with COPD (p = 0.012 S). Among the AS group, 52.6% were bidi smokers and 47.4% were cigarette smokers, while in the COPD group, 76.2% were bidi smokers and 23.8% were cigarette smokers. Based on the pack-years of smoking, the subjects were classified as light smokers (<14 pack years) and heavy smokers (>14 pack years).
The pulmonary function tests
The subjects were originally grouped as AS and HNS, depending on the respiratory symptoms and the spirometry values. The smokers with COPD had severe airflow limitations (FVC, 69.8+16.7%; FEV1, 47.47+16.9%; FEV1/FVC, 53.1+13.3%). The BMI was found to be significantly lower among the patients with COPD (19.1+4.8kg/m2) as compared to those among the AS (23+4.3kg/m2) and the HNS (23.7+4.0kg/m2). No differences in the absolute counts of the peripheral blood T-lymphocyte subsets and in the CD4+/CD8+ ratios among the HNS, AS, and the patients with COPD were observed [Table/Fig-2]. There was no significant correlation between the T-lymphocyte subsets and the smoking intensity [Table/Fig-3].
Lymphocyte subsets in various subject groups
| Variables | Healthy non-smokers (n=20) | Asymptomatic smokers (n=19) | COPD (n=21) | p value |
|---|
| CD3+ | 1424.9±352.2 | 1251.9±491.6 | 1154.3±582.2 | 0.207 NS |
| CD4+ | 832.5±220.7 | 745.7±313.8 | 652.7±340.5 | 0.161 NS |
| CD8+ | 500.4±191 | 426.9±193.2 | 424.7±264.3 | 0.470 NS |
| CD4+/CD8+ | 1.83±0.74 | 1.89±0.72 | 1.88±1.26 | 0.976 NS |
showing that there was no correlation between T-lymphocyte subsets and pack years (<14 pack years – light smokers; > 14 pack years – heavy smokers)
| Pack years | Mean + SD | Mann-Whitney test (Z) | p value |
|---|
| CD3+ | <14 | 1287.25±465.35 | 0.98 | 0.327 |
| >14 | 1179±557.49 |
| CD4+ | <14 | 792.38±299.73 | 1.05 | 0.295 |
| >14 | 673±333.95 |
| CD8+ | <14 | 423.75±173.07 | 0.24 | 0.813 |
| >14 | 426.28±244.91 |
| CD4+/CD8+ | <14 | 1.99±0.59 | 0.96 | 0.335 |
The mean CD3+ T-cell absolute count in the COPD patients (1154.3+582.2), was markedly lower than those among the AS (1251.9+491.6) and the HNS (1424.9+352.2). The mean CD4+T-cell count in the COPD patients (652.7+340.5) was also lower as compared to those among the AS (745.7+313.8) and the HNS (832.5+220.7). There was no statistically significant difference between the mean CD8+T-cell counts of the COPD patients (424.7+264.3), the AS (426.9+193.2) and the HNS (500.4+191). We did not find any correlation between the T-lymphocyte subsets and the type of smoking (bidis or cigarettes) [Table/Fig-4].
showing that there was no correlation between T-lymphocyte subsets and type of smoking
| T cell subset | Type of smoking | N | Mean + SD | Mann Whitney Z value | p value |
|---|
| CD3+ | bidis | 26 | 1189.6±570.1 | 0.68 | 0.510 NS |
| cigarettes | 14 | 1220.5±487.6 |
| CD4+ | bidis | 26 | 678.3±354.2 | 0.74 | 0.474 NS |
| cigarettes | 14 | 731.4±279.4 |
| CD8+ | bidis | 26 | 428.7±236.1 | 0.09 | 0.944 NS |
| cigarettes | 14 | 420.3±227.9 |
| CD4+/CD8+ | bidis | 26 | 1.81±1.2 | 0.98 | 0.334 NS |
| cigarettes | 14 | 2.03±0.8 |
DISCUSSION
The primary focus of our study was to determine whether the peripheral adaptive immune functions in the COPD patients correlated with the severity of the airflow obstruction. Several theories have been hypothesized with regards to the role of the T-cells in COPD. An important hypothesis is that the cytotoxic T-cells could drive apoptosis and thus, destruction of the lung tissue. Another theory states that the T-cells could release several proinflammatory cytokines, which could further activate more T-cells and other inflammatory cells. However, the type of T-cells which are activated and the cytokines which are released by them, would determine the final outcome in COPD (chronic bronchitis/emphysema). Sixty age-matched subjects, with 33% belonging to the HNS group, 32% belonging to the as group and 35% belonging to the COPD group were included. No statistically significant difference in the T lymphocyte subsets was found between the control and the study groups. This was similar to the results of Kim WD et al., [4] and De Jong et al., [6] who observed that the difference between the T lymphocyte subsets in the COPD patients and the asymptomatic smokers was not significant.
Miller et al., in 1982, analyzed 60 smokers and 35 non-smoking controls and grouped the smokers as light smokers (10-19 pack years), moderate smokers (20-49 pack years) and heavy smokers (50-120 pack years). They found that the WBCs were increased in all groups of smokers, but that the relative percentage of the lymphocytes was not different from that of normal subjects. The percentages of CD3+ and CD4+ were similar in all the groups of smokers and in the normal subjects. Among the smokers, the percentage of the CD4+ T-cells was considerably decreased in the heavy smokers (41+2%), as compared to those in the light (48+2%) and moderate smokers (48+1%). The percentage of the CD8+ T-cells was significantly higher in the heavy smokers (28+1%) than in the non-smokers (2+1%), light smokers (22+1%) and the moderate (24+1%) smokers. Hence, the heavy smokers had a relative decrease in the CD4+ T-cells and an increase in the CD8+T-cells, with a low CD4+/CD8+ ratio [7].
Koch A et al., found that there was a significant increase in the peripheral blood neutrophils in the smokers with COPD (65.2+1.7%) as compared to the nonsmokers (57.5+2.6%). They also found that the COPD patients had higher lymphocyte counts than the asymptomatic smokers and the controls. There was a significant increase in the percentage of the CD4+/CD3+ T-cells and a significant decrease in the percentage of the CD8+/CD3+ T-lymphocytes in the smokers with COPD (CD4+:73.4+2.1%, p<0.01; CD8+: 22.7+1.6; p<0.01) as compared to the nonsmokers (CD4+: 60.5+2.0%, CD8+: 34.2+2.0) and the smokers without COPD (CD4+: 65.9+2.5%, p<0.05; CD8+: 29.8+2.1;p<0.05) [8].
Pons J et al., conducted a study in Spain on 10 HNS, 20 AS and 20 COPD patients. The COPD patients were slightly older (66.4+1.6years) than the HNS (57.8+6.3years) and the as (58.0+1.9 years) groups. The smoking history of the patients with COPD and of the smokers with normal lung functions was similar. In the blood, the percentages of CD4+ (60.0+4.7%, 57.1+2.7% and 60.2+3.1%) and the CD8+ T-lymphocytes (35.6+4.6%, 35.2+2.6% and 34.6+3.0%) were similar in the COPD patients, the asymptomatic smokers and the never smokers, respectively [9].
Gadgil et al., showed that the peripheral T-cells (particularly CD8+T-cells) were more frequently activated in the patients with COPD and that their levels correlated with the disease severity [10]. On comparing the COPD patients with the healthy smokers, Hodge et al., found a higher percentage of CD8+ T-cells in the blood and a lower CD4/CD8 ratio. Since they did not observe a decrease in the apoptosis of CD4+ T-cells which was relative to that of the CD8+ T-cells, they could not explain the increase in the CD8+ T-cells in COPD [11]. This was in contrast to the findings of other studies, which failed to show any differences in the T-cell subpopulations in the COPD, AS and the HNS groups [4,12].
Glader Pernilla and colleagues correlated the lung functions with the expressions of five different T-cell activation markers on the peripheral blood CD4+ T-cells and the CD8+ T-cells in COPD patients and they matched the smokers and never-smokers. No differences were found between the three groups with regards to the proportions of the lymphocyte populations, but the number of CD4+ T-cells in the smokers was higher than those in both the never-smokers and the COPD patients [13].
Zhu et al., in 2009, found that the COPD severity was significantly and inversely associated with the proportion of the circulating CD4+T-cells and that it directly correlated with the CD4+ production of IL-2, as well as the frequency of the CD8+T-cell activation and the CD8+ IFN-γ production [14].
In our study, a tendency towards lower absolute counts of the CD3+, CD4+ and the CD8+ lymphocyte subsets among the patients with COPD was detected, though it was not statistically significant [Table/Fig-5]. This may indicate that the T-cells do play a critical role in the maintenance of the peripheral tolerance and the prevention of autoimmunity among the COPD patients. One possible explanation for this finding is that the T cells could be reduced in the periphery as a result of their recruitment to the lung. Since these changes occurred in the smokers both in those with and without COPD, they cannot in themselves be responsible for the disease, but they could facilitate the development of the disease in smokers, in synergy with other inflammatory changes. However, there was no correlation between the CD8+ T-cell counts and the FEV1 (%pred.). The BMI was found to be significantly lower among the patients with COPD (19.1+4.8kg/m2) as compared to those in the AS (23+4.3kg/m2) and the HNS (23.7+4.0kg/m2) groups, which perhaps supported the fact that COPD was a systemic disease [15].
Comparison of CD3+, CD4+ and CD8+ in HNS, AS and COPD
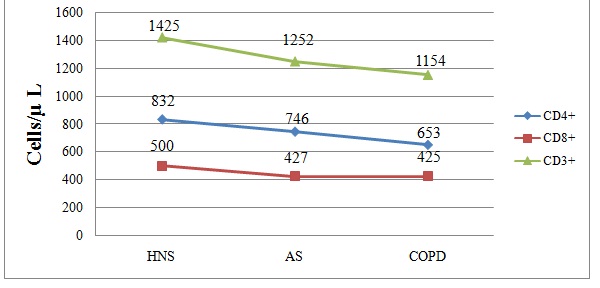
In this study, there was no significant difference in the total leukocyte counts among the 3 groups (ANOVA F value – 2.238 and p value – 0.116). However, in contrast to the findings of Miller et al., [7] a significant difference in the lymphocyte percentage between the various groups (Z value – 6.052 and p value – 0.05) was evident in this study. The absolute counts of the CD3+, CD4+, the CD8+ T-cell populations were similar in both the light and heavy smokers and hence, there was no correlation between the T-lymphocyte subsets and the intensity of smoking.
The presented results were in agreement with those of the studies which were conducted by Kim WD et al., De Jong et al., and Majori et al., which suggested that the origin of the abnormal T-lymphocyte infiltration which was seen in the lungs of the patients with COPD may be a local, rather than a systemic event [4,6,12].
A limitation of this study was the relatively small sample size in each subject group. Doing further studies on larger numbers of smokers with COPD as well as on patients with COPD who have discontinued smoking is necessary to substantiate the results. A larger study which can investigate the relationship of the T lymphocyte subset numbers in the peripheral blood with those in the lung tissue is needed.
This study included the Indian population as compared to most of the other studies which were done on western populations and hence, racial and genetic differences may have contributed to our results.
Cigarette smoking exerts different effects on the immune system at different doses, which further compounds the interpretation of the results. A majority of the subjects in our study were bidi smokers as compared to the majority of the cigarette smokers who were included in all the other studies. Hence, a larger subgroup analysis needs to be done, to evaluate the effects of bidi smoking on the CD4+ and the CD8+ T-cells.
The immunological assays which were done on the COPD patients may have been influenced by the distribution of the disease severities, as well as the smoking statuses and the pharmacologic therapies in the form of bronchodilators and inhaled corticosteroids (ICS).
CONCLUSIONS
Despite several studies being conducted in the field of the immunological changes in COPD, the exact pathogenesis and the role of the T-cells yet remains unclear. Though it was not statistically significant, our study has demonstrated a decrease in the blood CD8+ T-lymphocytes among the COPD patients. This may suggest a possible role of the cytotoxic T cells in the pathogenesis of COPD. Hence, it may be suggested that the increase in the CD8+ T-lymphocyte population in the central airways, which is seen in the patients with COPD may be the result of the local immunity rather than the systemic immunity. These results may be influenced by the small sample size, the Indian population, the genetic constitution, the age and the smoking history of bidis. These effects could potentially affect the present results and they should, therefore, be addressed in future studies.
Competing Interests: None to declare
Patient Consent: In this study, the pulmonary function tests and the blood tests were done (with informed consent) for the purpose of classifying the subjects into the study groups. The patient confidentiality was maintained.
Ethics Approval: The Institution Ethics Committee of Father Muller Medical College, Mangalore, India.
Funding: For the purpose of the study, the investigations were done at a subsidised rate by Father Muller Medical College and the Manipal Life Sciences Laboratory.