INTRODUCTION
Adenomatoid Odontogenic Cysts (AOCs), the most intriguing and extremely fascinating hamartomatous malformations, have been described under a variety of terminologies till the recent years. Various authors have made different attempts for designating this entity. The first case was reported as “epithelioma adamantinum” by Steensland in 1905 [1].
The most widely accepted terminology is that which was proposed by Philpsen and Birn in 1971 of an “Adenomatoid Odontogenic Tumour” (AOT) [2]. This term was later adopted by the World Health Organization (WHO) and it was defined as. “A tumour of odontogenic epithelium with duct –like structures and with varying degrees of inductive changes in the connective tissue. The tumour may be partly cystic, and in some cases, the solid lesion may be present only as masses in the wall of a large cyst. It is generally believed that the lesion is not a neoplasm” [2]. Although the WHO definition states that the lesion may have a cystic nature, only very few cases have been reported.
Philipsen and Riechart have defined this lesion as “A hamartomatous lesion of odontogenic epithelium producing solid nodules of cuboidal or columnar cells here and there, forming convoluted bands which are arranged in complicated patterns. Throughout the lesion, the cells form structures which have a tubular or a duct like appearance. The lesion may be partly cystic, with the solid tumourous tissue constituting part of a large cyst wall. The fibrous connective tissue stroma is rather sparse and it may contain a dysplastic dentinoid as well as calcified material that may be quite extensive”. The cystic presentation was reported by Harbitz as a “Cystic Adamantoma” in 1915 [3,4]. It was referred to as “2/3rd tumour” because 2/3rd of the cases occur in the maxilla, 2/3rd of the cases occur in young woman, 2/3rd of the cases occur in unerupted teeth and 2/3 rd of the cases have been found to arise from the canine area [5].
Robert Markz and Daniel Stern regarded the lesion as a cyst rather than a tumour, that presents as an hamartomatous intraluminal proliferation of the epithelial cells which are derived from Hertwig’s epithelial root sheath (HERS), which fills the cystic space, giving a solid appearance [5]. The aim of this report was to present a unique case of AOC which arose in the posterior area of the mandible, with special emphasis on its histoarchitectural spectrum.
CASE REPORT
A 19-years-old male patient presented to a private dental clinic with the complaint of pain and swelling for the past six months on the left side of the face. There was no history of trauma.
His extra oral examination showed mild facial asymmetry, with the swelling measuring around 6x3cms, which extended anteriorly from the symphysis region to the parotid area and which posteriorly involved the ramus. The lesion was tender on palpation.
The intra oral examination revealed the presence of all the teeth from 31-36, with the absence of 37 and 38 [Table/Fig-1].
Intraoral photograph showing absence of 37 & 38 in the arch
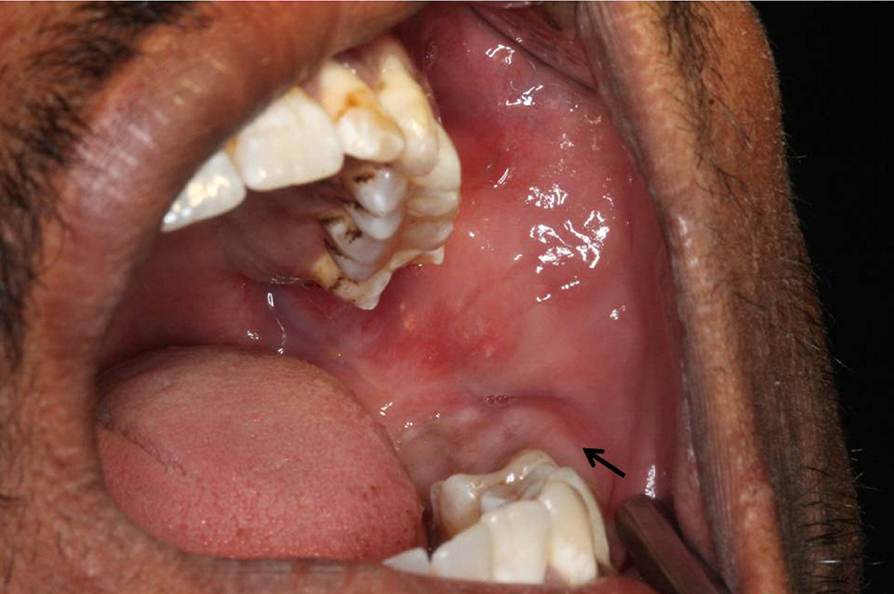
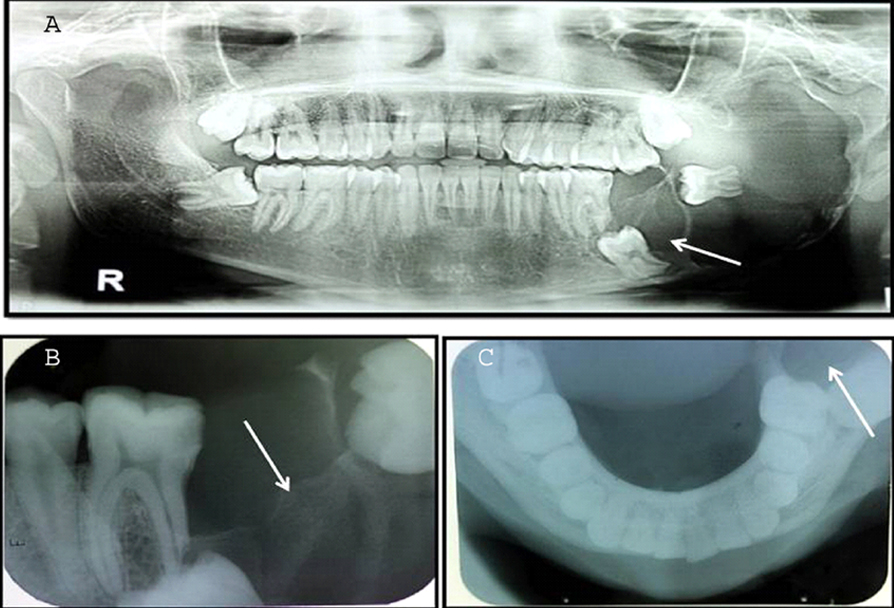
The radiographic examination showed a well defined large radiolucency which involved the angle of the mandible, till the left first molar area. Root resorption was observed in relation to 36 and 37 was placed in an apical position in relation to 36, along with an impacted 38 [Table/Fig-2]. A provisional diagnosis of a dentigerous cyst with an impacted 38 was given.
(a) OPG showing a well-defined radiolucent lesion with resorption of roots of 36. 37 is seen apically i.r.t to 36 with impacted 38. (b) IOPA showing defined radiolucency in relation 37 and 38 with resorbed roots of 36. (c) Occlusal radiograph showing a well defined radiolucency with impacted 38.
Macroscopically, the specimen consisted of multiple bits that were soft to firm in consistency and grayish white in colour. One bit of tissue was associated with 38 and some tissue bits were found to surround the CEJ of the molar [Table/Fig-3].
Gross specimen showing a large bit of tissue with brownish black in color, firm in consistency with tooth attached at the cervical area. Few minor fragment of tissue with irregular borders are also observed

This particular lesion particularly is of academic interest to the pathologist, rather than to the clinician, because it does not differ from the dentigerous cysts clinically.
HISTOPATHOLOGY
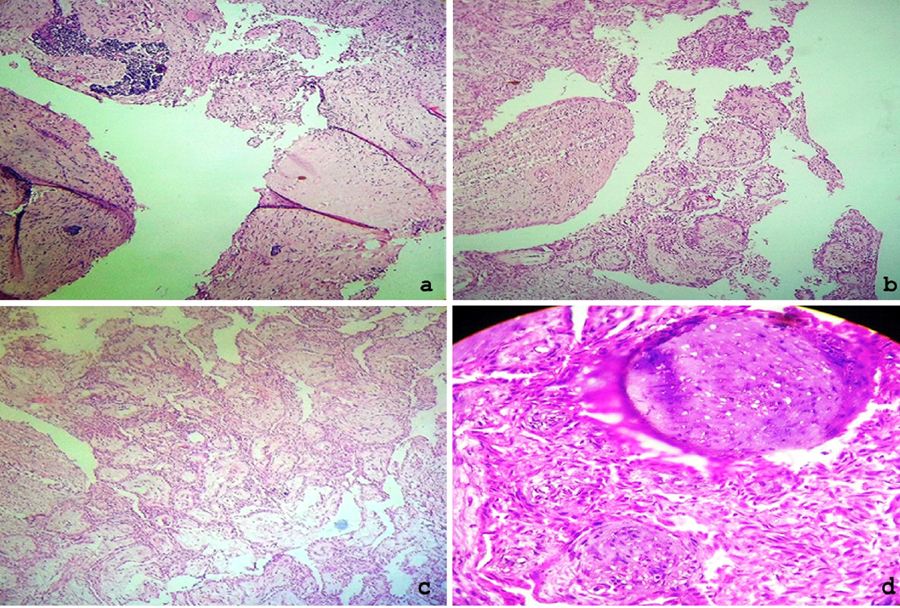
The histopathology of our lesion was very interesting and unique. On staining the tissue with Haematoxylin and Eosin (H and E), the sections showed an encapsulated lesional tissue, which consisted of different sized nodules with cuboidal to columnar epithelial cells which formed nests or rosette like structures, with minimal stromal connective tissue [Table/Fig-4].
(a) Cystic fibrous capsule with odontogenic islands in the periphery. (H&E, 40x). (b) Tumor showing multinodular proliferation of cells arranged in nodules and thin cords in the periphery (H&E, 10x). (c) Tumor islands showing polyhedral epithelial cells arranged in nodular pattern. (H&E, 10x). (d) Nodular arrangement of tumor cells interspersed with spindle shaped cells showing hyperchromatism & nuclear pleomprphism. (H&E, 40x)
Thin anastomosing strands of the basaloid cells of the tumour islands were also found to mimick a plexiform ameloblastoma pattern in few areas. The spindle shaped cells with a dark, eosinophilic cytoplasm and round hyperchromatic nuclei occupied the spaces between the epithelial nodules. In few areas, the tumour cell strands revealed a cribriform pattern along with a whorled arrangement [Table/Fig-5].
(a) tumor islands arranged in thin strands that are anastomosing, mimicking plexiform ameloblastoma.(H&E, 10x). (b) cells arranged in ductal & cribriform pattern and thin cords with interspersed connective tissue stroma. (H&E, 40x). (c) sheets of tumor cells with lumen containing eosinophilic material.(H&E, 10X). (d) presence of calcifications in spheroidal and globular pattern (H&E, 40x).
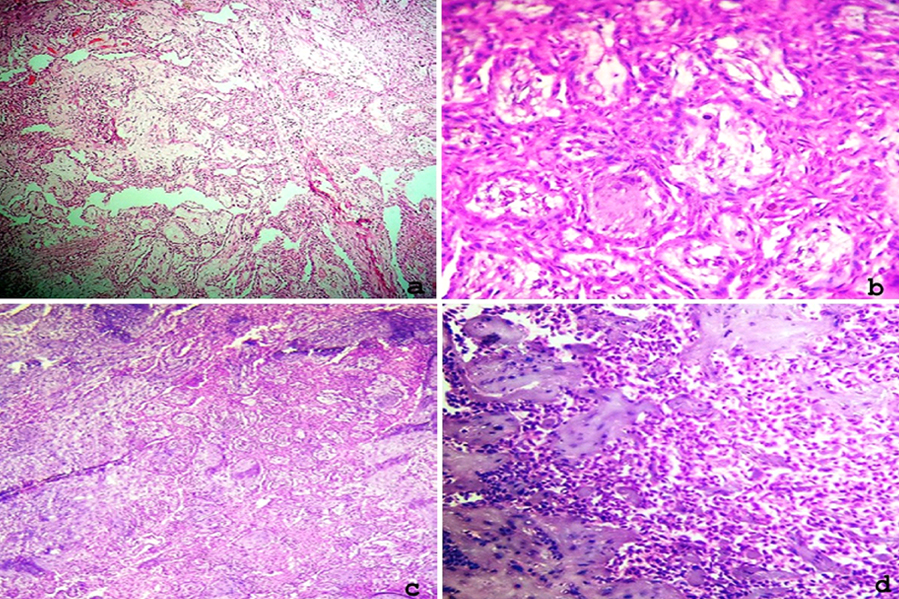
The tubular or duct like structures were lined by a single row of low columnar epithelial cells, the nuclei of which were polarized away from the luminal surface. The ducts varied in size and the cystic lumens were empty in some. In other cells, they contained a variable amount of eosinophilic material. Few calcified areas were also observed [Table/Fig-5].
DISCUSSION
Regarding the controversy of this lesion, it is regarded as a hamartoma or a benign neoplasm or a developmental anomaly or a cyst. It was considered to be an hamartoma clinically, due to its limited size and lack of recurrence [1,5,6]. It has also been described as a hamartoma histologically, because of its metaplastic mineralization. It has also been described as a neoplasm, because of its slow growing nature and its early detection, before it reached a clinically noticeable size.
Macroscopically, “it is a tumour like tissue that fills the follicular space and presents as a solid mass, with few tumour like nodules which can be observed”. It was also described, histologically as a benign tumour which showed inductive capacity.
The lesional tissue shows a greater departure from the arrangement of the normal odontogenic apparatus, than would be expected in a developmental anomaly, as was thought by few authors in its very initial stages of its inception.
It can also be considered as a cystic lesion, as it was in our case. A similar lesion was reported by Handschel et al., [7], that exhibited a cystic epithelium that lacked the lining.
The cystic lesion which we are describing here, is rightfully called as a perfect imitator of a dentigerous cyst with the similar classic clinical and radiographic features, which can render a diagnosis of AOC. It readily separates from its bony crypt, because it has a thick capsule and it presents as an expophytic epithelial lining which grows into the lumen [5].
Its origin is controversial; but most of the authors accept it to be odontogenic, as it occurs within the tooth bearing areas of the jaws and are often found in close association with embedded teeth, having cytological features which are similar to those of various components of the enamel organ, the dental lamina and the Reduced Enamel Epithelium (REE) and/or their remnants.
Philipsen et al suggested that its origin could be the dental lamina complex or its remnants, which are haphazardly distributed but are confined to the soft tissue of the gubernaculum dentis, a soft tissue band which unites the tooth sac with the overlying epithelium [1].
HYPOTHESIS
There are two different hypotheses that can be attributed to the occurrence of a cystic lesion, both macroscopically and histologically.
First Hypothesis: The first hypothesis was thought to arise from the follicular lining of unerupted teeth that indeed arose from the reduced enamel epithelium (or) that it was a cystic lesion which originated from the lining of a dentigerous cyst. Macroscopically, the crown of the tooth is surrounded by and attached to the neck of the unerupted tooth. This can happen only when a cystic lesion occurs after a complete cystic expansion.
Second Hypothesis: The second hypothesis could be presence of cystic changes in the follicles of the tumour islands or probably there was an attempt to form a glandular tissue, since the origin was from the basal cells of the oral epithelium, which had a multiple differentiation capacity. It is also assumed by few authors, that in certain cases, if at all the lesion is a long standing one, the cyst enlarges and fills the lumen completely. It cannot be denied that when there is an impacted tooth, a dentigerous cyst develops first, followed by a cystic lesion, or it may directly develop as a cystic lesion.
The cystic lesion does not arise from the follicle of the tooth crown, but instead from the HERS, which would explain the finding of the tooth being completely within the lumen rather than the tooth root being within a bony crypt. The proliferation that may fill the lumen gives an impression of a solid tumour, but on close inspection, it will reveal that its emergence was from an epithelial lining. The calcifications also represent the attempt of the HERS to induce a root dentine-dentinoid material [5].
The most interesting finding in our case was that, a majority of the above mentioned histomorphological patterns existed in our particular case, that was indeed encapsulated.
Nodule formations in the lining of the cysts are very well known in odontogenic cysts. In a cystic lesion, we do find the nodule formation, which can be better appreciated in the macroscopic view, when it is compared to other cysts.
The histological variations can be attributed to the origin of the lesional tissue which occurs before or after the cystic expansion. If it had occurred before the cystic expansion, the tumour would have filled the follicular space and it would present as a solid tumour form. If it had occurred after the cystic expansion, then it would have originated from a dentigerous cyst.
The histological variants which were appreciated in our case had been previously discussed and reported by Mutalik et al., [14] [Table/Fig-6].
| Author with year | Histological Diversity |
|---|
| Siar et al., [4],1986 | Cystic variants forming mural lining |
| Philipsen et al., [8], 1991 | AOT with CEOT-like areas |
| Convoluted cords or bodies mimicking invaginations |
| Interlacing strands of cells |
| Luminal proliferations into cystic lumen |
| Nests-like pattern |
| Rosette like arrangement |
| Sheets of tumor cells |
| Trabecular arrangement |
| Tubular arrangement |
| Philipsen et al., [8],1991, Takahashi et al., [9], 2001 | Cribriform pattern |
| Philipsen et al., [8], 1991, | Duct-like structures |
| Nomura et al., [10], 1992, Garg et al., [11], 2009 | Whorled spheroidal masses of tumor cells |
| Fredrich et al., [12], 2009 | Peripheral strand of smaller cells which form net like proliferations |
| Garg et al., [11], 2009 | Ribbon-like pattern |
| Ring-like pattern of tumor cells |
| Arrangements of cells in layers |
| Gadeawarand srikant [13], 2010 | Cystic variant Of AOT |
To come to the final diagnosis of this lesional tissue, the opinion was asked by a general pathologist, who diagnosed it as a plexiform ameloblastoma. This could have been because of the areas which appeared or mimicked a plexiform ameloblastoma. These types of cases can be better evaluated or diagnosed by an oral pathologist who is aware of the clinical and the histopathological criteria.
CONCLUSION
It can be stated that “it is a tumour like tissue that fills the follicular space and presents as a solid mass, with few tumour like nodules which can be observed macroscopically” which suggests that it could be a neoplasm”.
Glickman et al., concluded that “such a controversy is irresolvable, because sound arguments can be advanced in favour of and against both the hypotheses. The arguments are based mostly on a personal bias rather than on scientific evidence” [8].
We conclude that the present case with varied histomorphological patterns helped us in making the diagnosis with ease. All the previous attempts which were made to determine an AOT directly or that which arose from dentigerous cysts are to be given a thought, as they can be regarded as cysts and not tumours anymore, as per our above discussion and reasoning.
[1]. Philipsen HP, Reichart PA, Adenomatoid odontogenic tumour: facts and figuresOral Oncol 1998 35:125-31. [Google Scholar]
[2]. Reichart PA, Philipsen HP, Adenomatoid odontogenic tumourOdontogenic Tumors and Allied Lesions 2004 LondonQuintessence Publishing Co Ltd:105-16. [Google Scholar]
[3]. Harbitz F, On cystic tumours of the maxilla, and especially on adamantine cystadenomas (adamantomas)Dental Cosmos 1915 57:1081-93. [Google Scholar]
[4]. Philipsen HP, An updated clinical and epidemiological profile of the AOT: a collaborative retrospective studyJ Oral Pathol Med 2007 36:383-93. [Google Scholar]
[5]. Marx RE, Stern D, Oral and Maxillofacial Pathology: A rationale for diagnosis and treatment 2003 Hanover ParkQuientessence Publishing:609-12. [Google Scholar]
[6]. Rick GM, Adenamatoid odontogenic tumorOral Maxillofac Surg Clin North Am 2004 16:333-54. [Google Scholar]
[7]. Philipsen HP, Reichart PA, Zhang KH, Nikai H, Yu QX, Adenomatoid odontogenic tumor: Biologic profile based on 499 casesJ Oral Pathol Med 1991 20:149-58. [Google Scholar]
[8]. Handschel JG, Depprich RA, Zimmermann AC, Braunstein S, Kubler NR, Adenomatoid odontogenic tumor of the mandible: Review of the literature and report of a rare caseHead Face Med 2005 24:1-3. [Google Scholar]
[9]. Takahashi H, Fujita S, Shibata Y, Yamaguchi A, Adenomatoid odontogenic tumour: Immunohistochemical demonstration of transferrin, ferritin and alpha-one-antitrypsinJ Oral Pathol Med 2001 30:237-44. [Google Scholar]
[10]. Nomura M, Tanimoto K, Takata T, Shimosato T, Mandibular adenomatoid odontogenic tumor with unusual clinicopathologic featuresJ Oral Maxillofac Surg 1992 50:282-85. [Google Scholar]
[11]. Garg D, Palaskar S, Shetty VP, Bhushan A, Adenomatoid odontogenic tumor - hamartoma or true neoplasm: a case reportJ Oral Sci 2009 51:155-59. [Google Scholar]
[12]. Friedrich RE, Scheuer HA, Zustin J, Adenomatoid odontogenic tumor (AOT) of maxillary sinus: Case report with respect to immunohistochemical findingsIn Vivo 2009 23:111-16. [Google Scholar]
[13]. Gadewar DR, Srikant N, Adenomatoid odontogenic tumour: tumour or a cyst, a histopathological support for the controversyInt J Pediatr Otorhinolaryngol 2010 74:333-37. [Google Scholar]
[14]. Mutalik VS, Shreshtha A, Mutalik SS, Radhakrishnan R, Adenomatoid odontogenic tumor: A unique report with histological diversityJ Oral Maxillofac Pathol 2012 16:118-21. [Google Scholar]