A Rare Case of Cervical Tuberculosis which Simulated Carcinoma of the Cervix
Saichandran Sabita1, Vijayan Sharmila2, Thirunavukkarasu Arun Babu3, Sankappa P Sinhasan4, Singh Darendra5
1 Associate Professor, Department of Obstetrics & Gynecology,
2 Assistant Professor, Department of Obstetrics & Gynecology,
3 Assistant Professor, Department of Pediatrics
4 Associate Professor, Department of Pathology,
5 Professor, Department of Obstetrics & Gynecology, Indira Gandhi Medical College and Research Institute (IGMC&RI), Pondicherry-605 010, India.
NAME, ADRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vijayan Sharmila, Assistant Professor, Department of Obstetrics & Gynecology, Indira Gandhi Medical College and Research Institute (IGMC&RI), Pondicherry-605 010, India.
Phone: 919843188678
E-mail: sharu_jipmer@yahoo.co.in
Cervical tuberculosis is a rare form of genital tuberculosis. The manifestations of genitourinary tuberculosis are protean in nature. A high index of suspicion is required for making prompt diagnosis.
The definitive diagnosis is based on the demonstration of the characteristic lesion on histopathology or on bacterial isolation. We are reporting a rare case of isolated cervical tuberculosis which mimicked carcinoma of the cervix. A 24 years old para 1, live 1, woman presented with secondary amenorrhoea and post coital bleeding which were there for one year. The speculum examination revealed a friable cervix which bled on touch. Though the clinical history and the examination findings were suggestive of a cervical malignancy, the histopathological examination revealed a granulomatous inflammation which was suggestive of tuberculosis. The patient responded well to the antituberculous therapy.
Cervix, Cervical tuberculosis, Genital Tuberculosis
INTRODUCTION
Genitourinary Tuberculosis (TB) is more prevalent in the developing countries like India, affecting 14 million people, mostly those in the reproductive age group [Table/Fig-1]. The incidence is also rising of late, partly due to its association with the human immunodeficiency virus infection [Table/Fig-2]. The clinical presentation of genitourinary tuberculosis is protean in nature and it can also be completely asymptomatic. Genital tuberculosis frequently affects the fallopian tubes (95-100%), the endometrium (50-60%), and the ovaries (20-30%), whereas the involvements of the vagina, vulva, myometrium and the cervix are less common [Table/Fig-3]. Cervical TB is extremely rare and it accounts for 0.1–0.65% of all the cases of tuberculosis and 5-24% of all the genital tuberculosis cases [Table/Fig-4]. Tuberculosis of the cervix without other genital involvements is extremely rare. We are reporting a rare case of isolated cervical tuberculosis which presented with the features of carcinoma of the cervix.
CLINICAL RECORD
A 24 years old para 1, live 1, woman presented to our Gynaecology Outpatients Department with secondary amenorrhoea of 1 year duration. She had a spontaneous vaginal delivery four years back and the postnatal period had been uneventful. She had lactational amenorrhoea for 2 years, following which she had resumed menstruation, which was once in 2 to 3 months, with a scanty menstrual flow for the next one year. This was followed by amenorrhoea for one year, for which she sought medical attention. She had a history of postcoital bleeding for the past one year. There was no family history of tuberculosis, genital malignancy or any significant medical or surgical illness in the past. On examination, the patient was found to be thinly built and poorly nourished. Her weight was 42 kg and her height was 152 cm. Her general and systemic examinations were unremarkable. The speculum examination revealed an unhealthy cervix which was friable and which bled on touch [Table/Fig-1]. The uterus was retroverted, normal in size and mobile and the fornices were free.
Cervical appearance on perspeculum examination before treatment

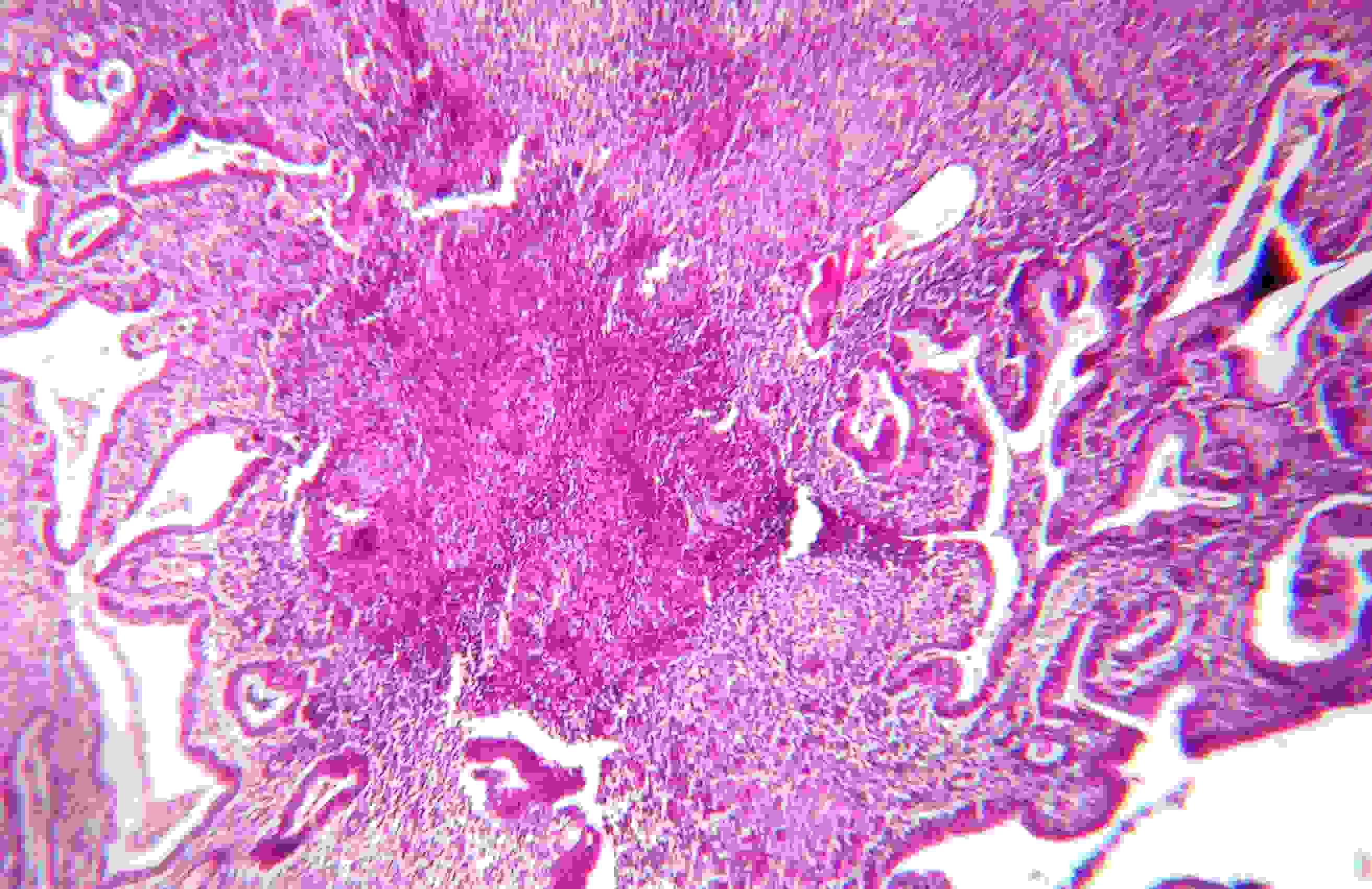
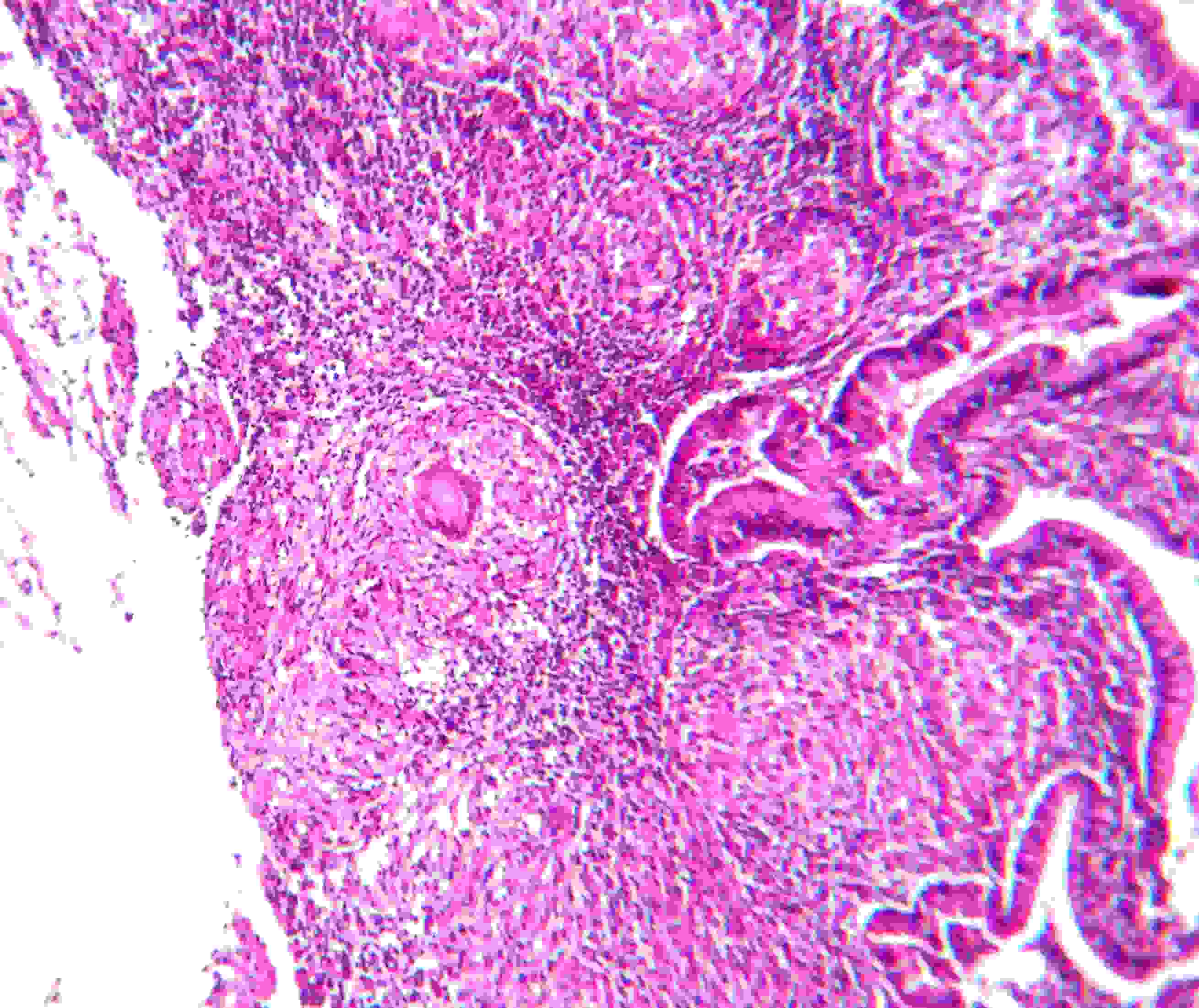
Her urine pregnancy test was negative. A treatment with progesterone and a combination of oestrogen and progesterone failed to induce the withdrawal bleeding. An ultrasound examination showed a normal sized uterus with a normal adnexa and a thin endometrium. The cervical cytology revealed inflammatory cells. A cervical biopsy and an endometrial sampling were done. The histopathological examination of the cervical biopsy revealed a necrotizing granulomatous inflammation [Table/Fig-2]. (H and E stain 5X). There were foci of caseating granulomas, along with Langhans’ giant cells [Table/Fig-3]. (H and E stain 10X). The staining for the acid-fast bacillus (AFB) was negative. The endometrial sampling was unremarkable. She was diagnosed as a case of cervical tuberculosis, based on the histopathology. The evaluation for primary pulmonary tuberculosis turned out to be negative. Her monogamous partner was evaluated for pulmonary and genitourinary tuberculosis by doing urine and semen analysis for AFB and ultrasound examination of the testes and the epididymis, but all turned out to be negative. The patient was provisionally diagnosed as cervical tuberculosis and she was started on antituberculosis treatment. The possible mode of transmission, whether it was an ascending or a descending infection, could not be established. The patient received 6 months of antituberculous therapy and a speculum examination which was done after the completion of the therapy, revealed a normal looking cervix [Table/Fig-4].
HPE of Cervical biopsy revealing necrotising granulomatous inflammation (H&E stain 5x)
HPE of cervical biospy showing caseating granulomas and langhan’s giant cells (H&E stain 10x)
Cervical appearance on perspeculum examination after treatment

DISCUSSION
In genital tuberculosis, the organs are infected by a haematogenous spread from a primary focus in the lungs. A cervical involvement represents a rare component of genitourinary tuberculosis. Cervical TB often occurs secondary to tuberculous salpingitis and endometritis. Cervical tuberculosis which occurs as a primary infection, which is caused by sexual contact with an infected partner, is rare. But an infection of tuberculous epididymitis in males and using sputum as a sexual lubricant have also been documented to transmit the disease [3, 5]. The common presentation of genitourinary tuberculosis in females include amenorrhoea, menstrual irregularities, infertility, vaginal discharges and postmenopausal bleeding.
The gross appearance of the cervix is highly variable. It may present in the papillary, ulcerative, interstitial, miliary, endocervical or the polypoid forms and even as an ulceration simulating invasive cervical cancer. The histological diagnosis requires demonstration of the caseating granulomas or tubercles in the cervical biopsy specimens. A lympho-plasmacytic infiltration can be present at the rim of the tubercles. The demonstration of AFB with the Ziehl-Neelsen staining may be difficult. Granulomatous lesions can also be seen in lymphogranuloma venereum, amoebiasis, brucellosis, tularaemia, sarcoidosis, schistosomiasis and foreign body giant cell granulomata to suture, crystal or cotton [6]. The presence of epitheliod cells and multinucleated Langhan’s giant cells on the cervical cytology can suggest a tubercular aetiology [7]. The bacterial isolation by culture is the gold standard for the diagnosis. The cervix usually responds to six months of the standard antituberculous therapy [4].
The incidence of the infertility in genital TB varies from 10 to 85% [6]. Genital TB accounts for 5-16% of the cases of infertility in India, though the actual incidence may be even more, due to the difficulty in establishing a diagnosis [6]. This case highlights the importance of considering the diagnosis of tuberculosis in a suspected case of carcinoma of the cervix. A high index of suspicion is required for a successful diagnosis of genitourinary tuberculosis, especially in the developing countries.
[1]. Agrawal S, Madan M, Leekha N, Raghunandan C, A rare case of cervical tuberculosis simulating carcinoma cervix: a case reportCases J 2009 2:161 [Google Scholar]
[2]. Seth A, Kudesia M, Gupta K, Pant L, Mathur A, Cytodiagnosis and pitfalls of genital tuberculosis: A report of two casesJ Cytol 2011 28:141-3. [Google Scholar]
[3]. Chowdhury NNR, Overview of tuberculosis of the female genital tractJ Indian Med Assoc 1996 94:345-61. [Google Scholar]
[4]. Lamba H, Byrne M, Goldin R, Jenkins C, Tuberculosis of the cervix: case presentation and a review of the literatureSex Transm Infect 2002 78:62-3. [Google Scholar]
[5]. Richards MJ, Angus D, Possible sexual transmission of genitourinary tuberculosisInt J Tuberc Lung Dis 1998 2:439 [Google Scholar]
[6]. Singh S, Gupta V, Modi S, Rana P, Duhan A, Sen R, Tuberculosis of uterine cervix: a report of two cases with variable clinical presentationTrop Doct 2010 40:125-6. [Google Scholar]
[7]. Kalyani R, Sheela S, Rajini M, Cytological diagnosis of tuberculous cervicitis: A case report with review of literatureJ Cytol 2012 29:86-88. [Google Scholar]