Invasive (solid) Papillary Carcinoma of the Breast: A Report of Two Cases
Leena J.B.1, Reshma G. Kini2, Safeena Amber3
1 Assistant Professor, Department of Pathology, Fr. Muller Medical College, Mangalore, India.
2 Assistant Professor, Department of Pathology, Fr. Muller Medical College, Mangalore, India.
3 Assistant Professor, Department of Pathology, Fr. Muller Medical College, Mangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Leena J.B, Assistant Professor, Department of Pathology, Fr. Muller Medical College, Mangalore, India.
E-mail: drleenapriye@yahoo.co.in
Papillary carcinoma is a rare malignant tumour of the breast with an incidence of 1-2% in the general population. The clinical behaviour of solid papillary carcinomas is generally indolent unless it is associated with invasion. Here, we are reporting two cases of solid invasive papillary carcinomas of the breast, who were 2 female patients aged 44 years and 55 years., with breast masses which were diagnosed by FNAC and confirmed by histopathology. The exact incidence and the clinical behaviours of such cases need to be ascertained by further research.
Invasive, Solid papillary carcinoma, Breast
INTRODUCTION
Papillary Carcinomas constitute 1-2% of the breast carcinomas in women. They generally occur in older women as compared to the other forms of breast carcinoma. Papillary carcinomas in general, have a slow growth rate and a better prognosis than the other forms of breast carcinomas [1], with a 100% 10 year survival rate [2]. Lymph node involvement and distant metastases are uncommon and if they are present, they are limited to the cases with invasive components [3]. When the epithelium has features which are diagnostic of intraductal carcinomas, the lesion is classified as a papillary carcinoma in situ. If a cystic component is present, the tumour is defined as a intracystic papillary carcinoma. Otherwise, the lesion is defined as a solid papillary carcinoma [2].
CASE REPORT
Case 1
A 44 years old female presented with a mass in the right breast, which had a duration of 2 years. On examination, the nipple showed crusting and retraction. The mass had a bosselated surface and was firm in consistency. It was situated in the inner quadrant of the breast. FNAC was done, which showed malignant tumour cells in singles, clusters and occasional papillary patterns, which were suggestive of a papillary carcinoma. Based on these findings, a right modified radical mastectomy was done and the specimen was sent for histopathology.
Case 2
A 55 years old female presented with a mass in the left breast, which had a duration of 1 year and it had increased in size since 3 months. On examination, a bosselated mass was felt in the left upper quadrant of the breast. FNAC was done, which showed highly cellular smears with cells in clusters and papillary patterns, which were suggestive of a papillary carcinoma. A left radical mastectomy was done and the specimen was sent for histopathology.
The gross specimens of both the cases showed partially encapsulated tumours with predominantly solid and partly cystic components. The tumours were grey brown and granular [Table/Fig-1].
Gross specimen breast showed a partially encapsulated solid grey white and granular tumor

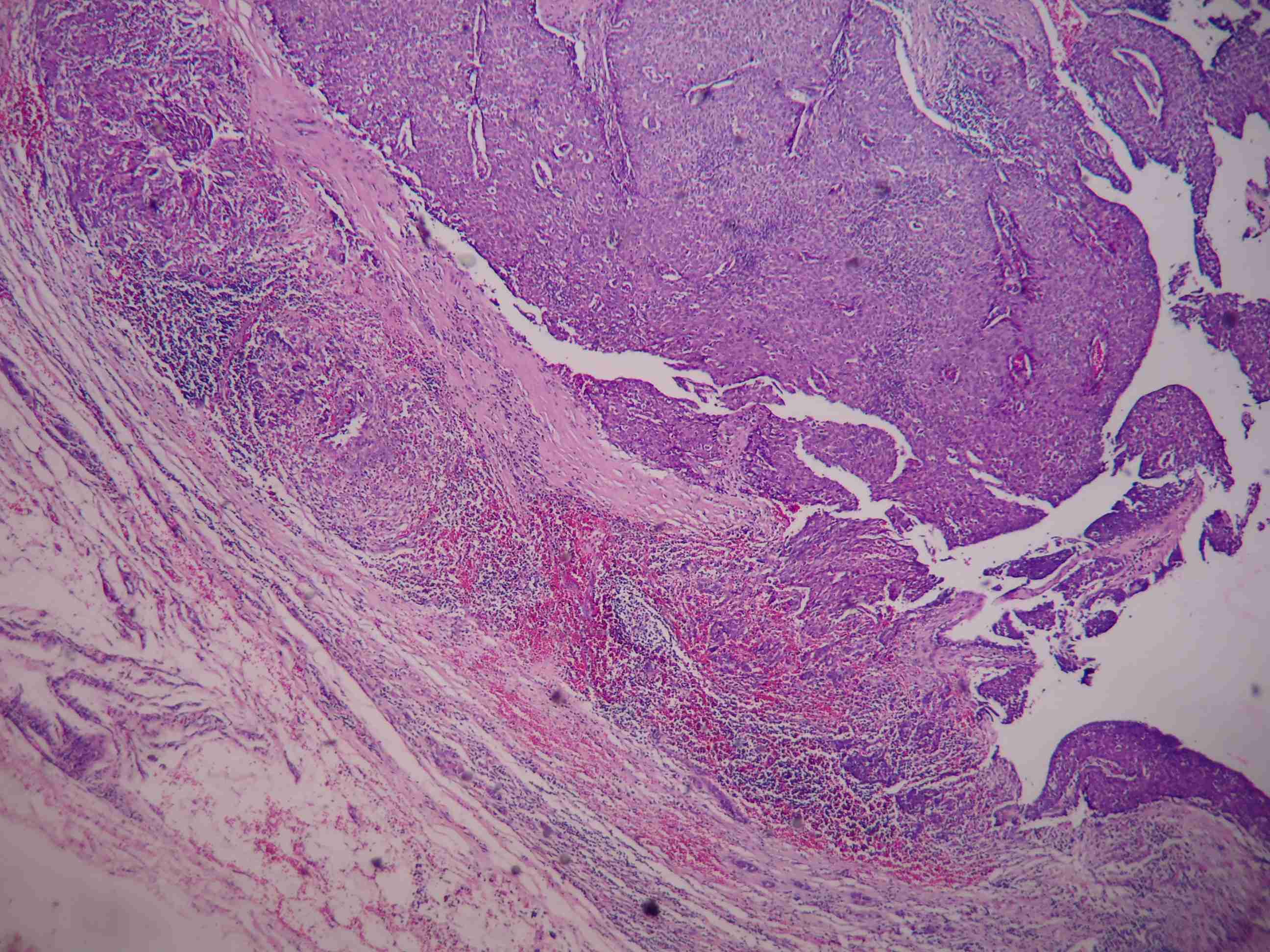
Microscopy of both the cases showed solid and partially encapsulated and cystic tumours.The tumour cells were arranged in lobules, with compactly arranged papillary fronds and branching networks of the fibrovascular cores [Table/Fig-2]. The tumour cells had large vesicular nuclei, stippled chromatin and moderate amounts of cytoplasm. The foci of the tumours showed infiltration into the surrounding breast tissue. The adjacent breast parenchyma showed the features of a ductal in-situ carcinoma. Due to the frank nature of the invasion which was seen, the immunohistochemical markers for the identification of the myoepithelial cells were not considered as necessary and a diagnosis of an invasive solid papillary carcinoma of the breast was given. Axillary dissections yielded an adequate number of lymph nodes which were negative for metastatic deposits in both the cases.
Cyst wall with invasion and the underlying papillary structure is represented by a network of fibrovascular cores among the solid cellular proliferation H & E 10X
DISCUSSION
Papillary carcinoma occurs mostly after the postmenoposal period, and the mean age at diagnosis is 63–67 years [4]. But in our case, one of the patients was a 44 year old woman and the other one was a 55 years old lady. Both of them presented with lumps in the breast rather than bloody nipple discharges, which have been quoted as the common presenting symptom in the literature [1]. Solid papillary carcinoma is also considered to be a variant of DCIS [5]. The histologic discrimination of the papillary tumours (benign or malignant) is based on the presence or the absence of the myoepithelial component. Foote and Stewart observed that in some areas, the cellular proliferation becomes so dense that the basic papillary properties become overgrown. Such tumours are classified as Solid Papillary Carcinomas (SPCs), as in both our cases. The SPC cases are divided into three groups: 1) SPC only (32.7%), 2) SPC with extravasated mucin (8.6%), and 3) SPC with invasive components (58.7%), which may be neuroendocrine-like (29.5%), colloid (23.5%), ductal not otherwise specified (14.5%), lobular (3%), tubular (3%), or mixed (26.5%) [3]. Both our cases were SPCs with invasive components. Fine-needle aspirations and core-needle biopsies may not be effective in distinguishing the in situ and the invasive papillary lesions, because the invasion is mostly seen at the periphery of the tumour. Therefore, an excision is recommended when papillary lesions are suspected or diagnosed through fine-needle aspirations or core-needle biopsies [6].
Macroscopically, the papillary carcinomas are well-defined and they usually contain haemorrhagic and cystic components. They may be solitary or multiple. In our cases, the lesions were unilateral and they included haemorrhagic components. The tumours of nearly half of the patients with papillary carcinomas are located in the centres (retroareolar areas) of the breast. On mammography, an intracystic papillary carcinoma generally appears as a round or oval circumscribed mass, mostly in the retroareolar region. Satellite nodules or microcalcifications are rarely seen. Ultrasound shows a cystic mass (with or without septations), with solid papillary masses projecting into the cyst lumen. Although the papillary carcinomas are usually cystic, some may be mixed in composition (predominantly a solid component) or pure solid lesions. The solid lesions tend to be more invasive. Invasive papillary carcinomas have a tendency to manifest as large masses which are related to the common presence of the bulky cystic components. Hence, the size of the invasive element is often small, and axillary metastases are infrequent, as in our cases. The solid papillary carcinomas are heterogenous tumours which have indolent clinical behaviours unless they are associated with invasion. However, our cases showed no evidence of metastasis or recurrence at six months of follow up.
In conclusion, invasive solid papillary carcinomas are rare malignant tumours of the breast, the clinical behaviours of which have to be ascertained by further research, though they are said to have aggressive clinical behaviours than those of other carcinomas in the presence of invasive components [7,8].
[1]. Soo MS, Williford EM, Walsh R, Bentely CR, Kornguth JP, Papillary Carcinoma of the Breast: Imaging FindingsAJR 1995 164:321-26. [Google Scholar]
[2]. Elverici E, Barc NA, Tqrksoy ZO, Araz L, Yqksel E, Bilateral invasive papillary carcinoma BreastClinical Imaging 2007 31:419-21. [Google Scholar]
[3]. Nassar H, Qureshi H, Volkanadsay N, Visscher D, Clinicopathologic analysis of solid papillary carcinoma of the breast and associated invasive carcinomasAm. J. Surg. Pathol 2006 30:501-07. [Google Scholar]
[4]. Liberman L, Feng TL, Susnik B, Intracystic papillary carcinoma with invasionRadiology 2001 219:781-84. [Google Scholar]
[5]. Collins LC, Schnitt SJ, Papillary lesions of the breast: selected diagnostic and management issuesHistopathology 2008 52:20-29. [Google Scholar]
[6]. Dogan BE, Whitman GJ, Middleton LP, Phelps M, Intracystic papillary carcinoma of the breastAJR Am J Roentgenol 2003 181:186 [Google Scholar]
[7]. Wagner AE, Middleton LP, Whitman GJ, Intracystic papillarycarcinoma of the breast with invasionAJR Am J Roentgenol 2004 183:1516 [Google Scholar]
[8]. Maluf HM, Koerner FC, Solid papillary carcinoma of the breast. A form of intraductal carcinoma with endocrine differentiation frequently associated with mucinous carcinomaAm. J. Surg. Pathol 1995 19:1237-44. [Google Scholar]