The Isometric Handgrip Exercise As a Test for Unmasking Hypertension in the Offsprings of Hypertensive Parents
Rinku Garg1, Varun Malhotra2, Usha Dhar3, Yogesh Tripathi4
1 Assistant Professor, Department of Physiology, Santosh Medical College, Ghaziabad, UP, India.
2 Professor, Department of Physiology, Santosh Medical College, Ghaziabad, UP, India.
3 Professor, Department of Physiology, Santosh Medical College, Ghaziabad, UP, India.
4 Professor, Department of Physiology, Santosh Medical College, Ghaziabad, UP, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rinku Garg Assistant Professor, Department of Physiology, Santosh Medical College, Ghaziabad, UP, India.
E-mail: rgrinkigarg6@gmail.com
Background: A familial history of hypertension increases the risk of hypertension in the offsprings.
Aims and objectives: The present study was undertaken to assess the underlying hypertension by using the Isometric Handgrip (IHG) exercise test in the offsprings of hypertensive parents and to compare it with age-matched controls of normotensive parents.
Material and Methods: The isometric handgrip test was performed in the study and control groups. The resting blood pressure was recorded before exercise and afterwards the subjects were asked to perform the isometric handgrip exercise with the dominant hand for 2 minutes. Then the blood pressure was recorded in the sitting position during and 5 minutes after the completion of the exercise.
Statistical Analysis: The analysis of the results was done by ANOVA with SPSS, version 17.0, by using the unpaired ‘t’ test.
Results: The results showed that the Resting Systolic (SBP), Diastolic (DBP) and the Mean (MBP) Blood Pressures were higher (p <0.001) in the offsprings of the hypertensive parents as compared to those in the control subjects of normotensive parents. During the isometric handgrip exercise test, the rise in the systolic, diastolic and the mean blood pressures was significantly higher (p<0.001) in the offsprings of the hypertensive parents. After 5 minutes of exercise, the SBP, DBP and the MBP were found to be significantly higher (p<0.001) in the study group as compared to those in the control group.
Conclusions: An early and a regular screening of the children of hypertensive parents is necessary to prevent any future cardiovascular complications.
Hypertension, Isometric handgrip, Resting blood pressure
INTRODUCTION
Hypertension is an increase in the blood pressure of =140/90 mm Hg measured on three separate occasions. Rapid urbanization, a sedentary life style, junk food and stress are the powerful environmental risk factors which are responsible for the increasing prevalence of hypertension, especially in the younger age group, that is associated with adverse cardiovascular complications [1]. Hypertension is a controllable disease. An early diagnosis and control can prevent 300,000 of the 1.5 million deaths which result from cardiovascular diseases in india [2].
The blood pressure is regulated by the autonomic nervous system [3]. An increased sympathetic tone and a decreased parasympathetic tone have been demonstrated in young normotensive offsprings of hypertensive parents [4,5]. This impairement of the autonomic activity can be detected in the young offsprings of hypertensive parents, with the application of various physical stress tests [6].
Exercise, in which contraction principally causes a change in the tension of the muscle with little change in the length, is termed as isometric or static e.g.lifting or pushing heavy weights and contracting muscles against fixed objects, in contrast to isotonic or dynamic exercises in which contraction of the skeletal muscle causes a change in the length of muscle, like running, swimming, etc. The static contraction of even a small mass of muscle causes a marked increase in the arterial pressure, with a relatively small increase in the heart rate and the cardiac output, thus primarily producing a pressure load on the heart [7–8]. A parental h/o hypertension increases the risk of developing hypertension [8].
A physiological test which is done to increase the arterial pressure is the isometric handgrip exercise test [9]. It provides pressor stimuli to the cardiovascular system through efferent sympathetic pathways, with a resultant increase in the heart rate and the blood pressure [10]. The isometric handgrip exercise can be used to unmask the underlying prehypertension in the children of hypertensive parents [11].
The relative consistency of the haemodynamic changes which occur during the isometric handgrip exercise test, indicates that it is a simple and a reliable method for studying the cardiovascular response to stress [12]. Lifestyle modifications like an increased physical activity, salt restriction and weight reduction, are effective for the prevention and the treatment of hypertension [3,13]. A routine screening must be performed to detect asymptomatic hypertension amongst adolescents with a family history of hypertension [14].
The aim of the present study was to unmask the underlying hypertension which follows physical stress, in the form of the isometric handgrip exercise test, in the descendants of hypertensive parents and to compare it with age-matched controls of normotensive parents.
MATERIAL AND METHODS
The present study was a cross-sectional study which was conducted in Santosh Medical College, Ghaziabad, UP, India. An ethical approval was obtained from the research committee of the Institution. Fifty medical students who were in the age group of 17-24 years, with a family history of primary hypertension (either single parent or both parents), were recruited for the study and the results were compared with those of fifty age-matched medical students with no familial history of hypertension. Informed consent was taken from all the medical students. The medical students with a h/o any chronic illness, those who were on any medication and smokers were excluded from the study.
The subjects were divided into 2 groups:
— Group I-control group with no family h/o hypertension
— Group II-study group with a family h/o hypertension
The procedure of the isometric handgrip exercise test was explained to all the students who participated in the study. Before the test, the subjects were allowed to rest for 10 minutes in a quiet room to reduce the anxiety.
The resting blood pressures of all the subjects were measured by the auscultatory method with the help of a mercury sphygmomanometer (Diamond). The first Kortkoff’s sound indicated the Systolic Blood Pressure (SBP) and the fifth Kortkoff’s sound indicated the Diastolic Blood Pressure (DBP). The mean blood pressure (MBP) was calculated as the diastolic blood pressure + 1/3rd of he pulse pressure.
The isometric handgrip exercise test was done in both the study and the control groups. After their basal blood pressures were recorded, the subjects were asked to perform the isometric handgrip exercise. The subjects were asked to hold the handgrip spring dynamometer in the right (or dominant) hand to get a full grip of it. The handles of the dynamometer were compressed by the subject by putting in maximum effort for few seconds. This whole procedure was repeated thrice with rests in between, to prevent fatigue. The mean of the three readings was referred to as the maximal isometric tension (Tmax).Then, the subjects were asked to perform the isometric handgrip exercise at 30% of Tmax for 2 minutes. During the test, the blood pressure was recorded from the non-exercising arm [15]. The blood pressure was again recorded 5 minutes after the completion of the exercise.
The results were analyzed by ANOVA with SPSS, version 17.0 by using the unpaired ‘t’ test.
RESULTS
The data which has been presented in [Table/Fig-1] shows that there was a significant increase in the basal SBP,DBP and the MBP in the individuals as compared to those in group I and that the values were statistically significant(p<0.001). In group II, the SBP, DBP and the MBP increases were much more pronounced in comparison to those in group I during the isometric handgrip exercise test (p<0.001). Five minutes after the isometric handgrip exercise (IHG), the systolic, diastolic and the mean blood pressures were found to be higher in group II (p<0.001) as compared to those in group I.
Difference in percentage between Group I & Group II
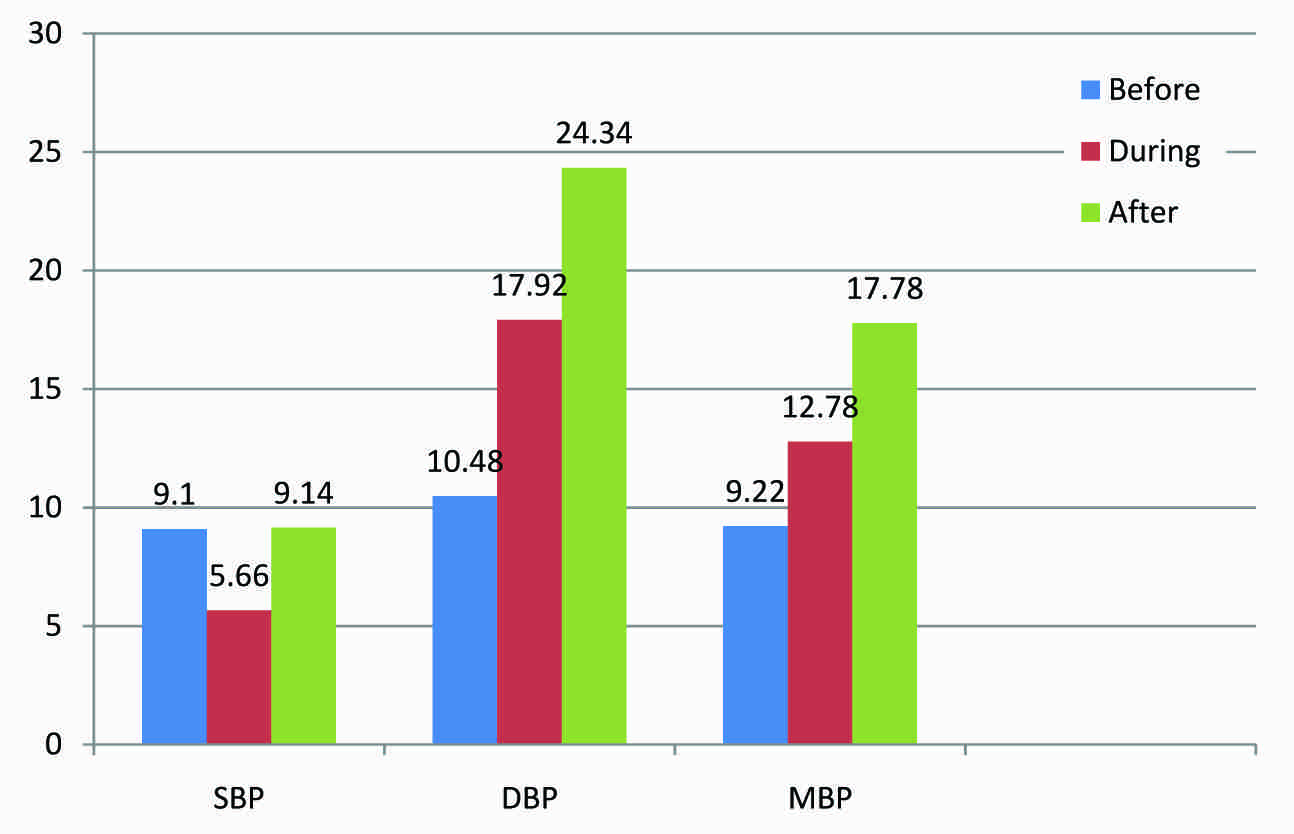
The percentage changes in the SBP, DBP and the MBP (mmHg) between the groups I and II have been presented in [Table/Fig-2].
It is evident from [Table/Fig-2], that before the exercise, there was a significant increase in the resting systolic (9.1%), diastolic (10.48%) and the mean blood pressures (9.22%) in the group II individuals as compared to those in group I. With the application of physical stress in the form of the isometric handgrip exercise, the percent increases in the diastolic (17.92%) and mean blood pressures (12.78%) were much more higher as compared to that of the systolic blood pressure (10.48%) in the group II individuals. Five minutes after the exercise, the percent increases in the diastolic (24.34%) and the mean blood pressures (17.78%) were found to be significantly higher as compared to the percent increase in the systolic blood pressure (9.14%) in the group II individuals.
Statistical analysis of SBP, DBP & MBP of basal blood pressure (before exercise), during IHG exercise and 5 minutes after IHG in group I and group II
| Subjects | Conditions | SBP(mmHg) Mean±SD | DBP(mmHg) Mean±SD | MBP(mmHg) Mean±SD |
|---|
| Group I (control group with no family h/o hypertension)(n=50) | Before(Resting BP) | 109.4±3.94 | 72.88±1.83 | 85.23±1.48 |
| During IHG | 120.72±3.04 | 83.00±1.83 | 95.66±1.49 |
| 5 min after IHG | 109.8±3.88 | 73.12±1.91 | 85.42±1.62 |
| Group II (study group with family h/o hypertension) n=50) | Before(Resting BP) | 119.36±3.32* | 80.52±3.98* | 93.09±2.13* |
| During IHG | 127.56±4.03* | 97.88±3.49* | 107.88±4.11* |
| 5 min after IHG | 119.84±3.35* | 90.92±3.24* | 100.6±2.79* |
* p<0.001 versus group I
*Percent value was calculated by taking group I as 100%
DISCUSSION
Our study results showed that the resting SBP, DBP and the MBP were significantly higher in the offsprings of hypertensive parents as compared to those in the offsprings of normotensive parents. There were significant increases in the systolic, diastolic and the mean blood pressures during the isometric exercise in the study group. Normally, during exercise, there is an increase in the concentrations of metabolites like lactic acid and adenosine, that are detected by the metabolite-sensitive nerve endings within the skeletal muscle interstitium. These substances increase the discharge of the group IV (metaboreceptor) afferent fibres, thus initiating a potent reflex that increases the sympathetic nerve activity. This leads to a vasoconstriction, which contributes to a rise in the BP [16]. However, it returns to normal within 5 minutes of stoppage of the exercise in normal individuals. But in our study, after 5 minutes of exercise, the SBP,DBP and the MBP were found to be significantly higher in the study group as compared to the resting blood pressure.
LOPES HF [5] showed that the resting blood pressures were higher in young normotensive subjects of hypertensive parents, which was due to an increased sympathetic activity before the exercise in these subjects and the results were consistent with those of our study. Their study showed that there were increases in both the systolic and the diastolic blood pressures during the isometric exercise, but that the increase did not differ significantly between the groups. However, the increase in the blood pressure in our study differed significantly between the groups, thus suggesting a greater reactivity of the blood vessels to physical stress. Ferrier et al., [17] also found higher plasma norepinephrine levels before exercise and an elevated rate of the spillover of norepinephrine to plasma in the offspring of hypertensive parents. However, no study, so far, has evaluated the blood pressure response, 5 minutes after the cessation of the exercise.
Krzeminski K [18] showed significant increases in both the systolic and the diastolic blood pressures with the isometric handgrip exercise and the findings were similar to our study results. The rise in the blood pressure was explained on the basis of the activation of the sympathetic adrenergic system, which was indicated by an increase in the plasma catecholamine level.
Bakke EF et al., [19] also showed a increase in the mean arterial pressure, which was consistent with our study results. An increased total peripheral resistance was the main factor which caused an increase in the blood pressure.
It has been shown that a common familial disturbance which could possibly predispose to the development of essential hypertension, was an imbalance between the cardiovascular noradrenaline responsiveness and the circulating noradrenaline [20]. The increased response to norepinephrine in the normotensive siblings of hypertensive parents was due to a reduced threshold to norepinephrine [21]. The increased blood pressure may also have been caused by the increased post-junctional (alpha-1) receptors during the isometric handgrip exercise [22].
Yamada Y et al., [23] reported that the baroreflex inhibition of the muscle sympathetic nerve activity was reduced in normotensive adolescents with a family history of hypertension. A reduced reflex sympatho-inhibition could lead to the development of hypertension due to an increase in the sympathetic vasomotor tone.
The isometric hand grip exercise activates the mechanoreceptors immediately, due to the increased muscle tension. The recruitment of new motor units to maintain the muscle tension, increases the excitatory state of the central nervous system and results in a possible increase in the sympathetic outflow and a decrease in parasympathetic outflow, which explain the increase in the blood pressure response [9].
It has been postulated that the pressure response to the isometric exercise is reflex in origin, which serves to increase the perfusion pressure to the active muscles, in which the blood flow is impeded by the sustained muscular contraction [24]. This may be the reason for the increase in the peripheral resistance and consequently, that in the diastolic pressure in our study. This can be explained on the basis, that the static (isometric) handgrip exercise causes an increase in the endothelin-1 in young normotensive offsprings of hypertensive parents [25] and thus, an increase in the blood pressure.
It was observed that youngsters with a parental history of hypertension showed enhanced reactivities of the total peripheral resistance during the static exercise, without higher blood pressure responses, as the physiological increase in stroke volume was blunted in the offsprings of hypertensive parents [26]. This explains why the blood pressures of this group of students did not increase during the exercise, significantly, as compared to those of the control group.
Static exercises increase the systolic and diastolic blood pressures mainly by central commands, causing changes in the activity of both the sympathetic and the parasympathetic systems. However, Haskell [27] and Martin [28] found that a rise in the blood pressure during the handgrip could also be achieved by an increased peripheral vascular resistance alone.
CONCLUSIONS
An early diagnosis of underlying hypertension in the offsprings of hypertensive parents should be done, to prevent any future cardiovascular complications.
* p<0.001 versus group I
*Percent value was calculated by taking group I as 100%
[1]. Das SK, Sanyal K, Basu A, Study of urban community survey in India: growing trend of high prevalence of hypertension in a developing countryInt J Med Sci 2005 2:70-78. [Google Scholar]
[2]. Gupta R, Gupta VP, Hypertension epidemiology in India: lessons from Jaipur heart watchCurrent Science 2009 97:3 [Google Scholar]
[3]. Ganong WF, Cardiovascular homeostasis in health and disease. In: Ganong WF, edReview of medical physiology 2005 22nd edNew YorkMcGraw Hill:631-46. [Google Scholar]
[4]. Pal GK, Pal P, Nanda N, Lalitha V, Dutta TK, Adithan C, Sympathovagal imbalance in prehypertensive offspring of two parents versus one parent hypertensiveInternational Journal of Hypertension 2011 [Google Scholar]
[5]. Lopes HF, Silva HB, Consolim-Colombo FM, Baretto Filho JA, Riccio GM, Giorgi DM, Autonomic abnormalities demonstrable in young normotensive subjects who are children of hypertensive parentsBrazilian Journal of Medical and Biological Research 2000 33:51-54. [Google Scholar]
[6]. Ferrara LA, Moscato TS, Pisanti N, Marotta T, Krough V, Capone D, Is the sympathetic nervous system altered in children with familial history of arterial hypertensionCardiology 1988 75(3):200-05. [Google Scholar]
[7]. Mitchell JH, Wildenthal K, Static( Isometric) exercise and the heart: Physiological and clinical considerationsAnnual Review of Medicine 1974 25:369-81. [Google Scholar]
[8]. Wang NY, Young JH, Meoni LA, Ford DE, Erlinger TP, Klag MJ, Blood pressure change and risk of hypertension associated with parental hypertension; the Johns Hopkins Precursors studyArchives of Internal Medicine 2008 168(6):643-48. [Google Scholar]
[9]. Hietanen E, Cardiovascular responses to static exerciseScand J Work Environ Health 1984 10:379-402. [Google Scholar]
[10]. Mathias CJ, Bannister R, Investigation of autonomic disorders. In Bannister R, Mathias CJ edsAutonomic failure: A text book of clinical disorders of the autonomic nervous system 1992 OxfordOxford University Press:266 [Google Scholar]
[11]. Helfant RH, De Villa MA, Meister SG, Effect of sustained isometric handgrip exercise on left ventricular performanceCirculation 1971 44:982-93. [Google Scholar]
[12]. Riendl AM, Robert WG, Reinke JA, Smith JJ, Cardiovascular response of human subjects to isometric contractions of large and small muscle groupsExperimental Biology and Medicine 1977 154(2):171-74. [Google Scholar]
[13]. Fagard RH, Exercise intensity and blood pressure response to endurance trainingHypertension 2011 28:20-23. [Google Scholar]
[14]. Garg R, Tripathi Y, Malhotra V, Sympathetic reactivity to cold pressor test in medical students of hypertensive parentsInternational Journal of Current Review and Research 2012 18 [Google Scholar]
[15]. Garg R, Kumar A, Effect of isometric handgrip exercise training on resting blood pressure in normal healthy adultsSantosh University Journal of Health Sciences2012(1)(1):29-34. [Google Scholar]
[16]. Mostoufi-Moab S, Widmaier EJ, Cornett JA, Gray K, Sinoway LI, Forearm training reduces the exercise pressor reflex during ischemic rhythmic handgripJournal of Applied Physiology 1998 84:1277-83. [Google Scholar]
[17]. Ferrier C, Cox H, Esler M, Elevated total body noradrenaline spillover in normotensive members of hypertensive familiesClin Sci. 1993 84:225-30. [Google Scholar]
[18]. Krzeminski K, Cybulski A, Ziemba A, Nazar K, Cardiovascular and hormonal responses to static handgrip in young and older healthy menEur J Appl Physiol 2012 112(4):1315-25. [Google Scholar]
[19]. Bakke EF, Hisdal J, Kroese AJ, Jergensen JJ, Stranden E, Blood pressure response to isometric exercise in patients with peripheral atherosclerotic diseaseClin Physiol Funct Imaging 2007 27(2):109-15. [Google Scholar]
[20]. Bianchetti MG, Weidmann P, Beretta-Piccoli C, Rupp U, Boehringer K, Link L, Disturbed noradrenergic blood pressure control in normotensive members of hypertensive familiesBr Heart J 1984 51:306-11. [Google Scholar]
[21]. De Lima JJ, Dias MM, Bernardes-Silva H, Belloti G, Pressor response to norepinephrine in essential hypertension. A study in familiesHypertension 1990 15(2 Suppl):I-137-39. [Google Scholar]
[22]. Hamada Mareomi, Kazatani Yukio, Shigematsu Yuji, Ito Taketoshi, Kokubu Tatsuo Ishise, Enhanced blood pressure response to isometric handgrip exercise in patients with essential hypertension: Effects of propranolol and prazosinJournal of Hypertension 1987 5(3):305-09. [Google Scholar]
[23]. Yamada Y, Miyajima E, Tochikubo O, Matsukawa T, Shinoiri H, Ishii M, Impaired baroreflex changes in muscle sympathetic nerve activity in adolescents who have a family history of hypertensionJ Hypertens Suppl 1988 6:S525-28. [Google Scholar]
[24]. McDonald HR, Sapru RP, Taylor SH, Donald KW, Effects of intravenous propranolol (Inderal) on the systemic circulatory response to sustained handgripAmer J Cardiol18:333-1966. [Google Scholar]
[25]. Mangieri E, Tanzilli G, Barilla F, Handgrip increases endothelin-1 secretion in normotensive young male offspring of hypertensive parentsJ Am Coll Cardiol 1998 31:1362-66. [Google Scholar]
[26]. De Visser DC, van HooftI M, van Doornen LJ, Hofman A, Orlebeke JF, Grobbee DE, Cardiovascular response to physical stress in offspring of hypertensive parentsJournal of Human Hypertension 1996 10(12):781-88. [Google Scholar]
[27]. Haskell WL, Savin WM, Schroeder JS, Cardiovascular responses to handgrip exercise in patients following cardiac transplantationCirc Res 1981 48:156-61. [Google Scholar]
[28]. Martin CE, Shaver JA, Leon DF, Thompson ME, Reddy PS, Leonard JJ, Autonomic mechanisms in hemodynamic responses to isometric exerciseJ Clin Invest 1974 54:104-15. [Google Scholar]