Depression is a major heterogenous disorder that affects a person’s mood, physical health and behaviour. Depressive disorder is a prevalent mental health disorder that was identified by the World Health Organization as the fourth leading cause of disability and premature death in the world in 2001 [1]. It has been estimated that by the year 2020, MDD would be only second to ischaemic heart disease with regards to the disease burden [2]. The drugs which are used are capable of causing a number of Adverse Drug Reactions (ADR), some of which may be fatal [3,4]. Although the past decade has resulted in clear advances in our understanding of Depressive Disorder, several issues still remain uncovered regarding the disease diagnosis and an effective clinical management. In recent years, a number of different drugs of different classes have been flooding in the market for being used for a better management of this common disorder [5]. Thus, the monitoring and the evaluation of the prescribing practices and pharmacovigilance studies are essential to emphasize the rationality of the medical care or to spark off a remedial message to the prescriber and the regulatory authorities.
PATIENTS AND METHODS
A longitudinal, observational clinical study was carried out in the Outpatients Department of Psychiatry in S.C.B. Medical College and Hospital in collaboration with the I.M.S and SUM Hospital in collaboration with S.C.B. Medical College and Hospital, for one year. This study had obtained the necessary administrative and the institutional ethics committee clearance. About 160 subjects were included in this study. The screening was done by trained doctors in the presence of a clinical psychologist. The subjects were selected from among the patients who had presented to the O.P.D. of the Department of Psychiatry and had complied with the protocol for the evaluation and the treatment of depression.
Inclusion Criteria
Outdoor patients who were suffering from depressive disorder, who attended the Psychiatry O.P.D.
Patients from all age groups and both the sexes were included.
Pregnant ladies who were suffering from depressive disorders.
Those who understood the purpose of the study and were ready to provide information regarding their health status and those who signed an informed consent document.
Exclusion Criteria
Patients who were suffering from malignancies and terminally ill patients.
Those who were judged clinically to be at a suicidal risk (too serious to be included in the study).
Those who had a history of allergic or serious adverse reactions (to study the medications).
Those who had a history of substance abuse.
At the study entry, all the patients who were on TCAs, SSRIs and Newer Antidepressants (SNRIs/NDRIs) were assessed by doing a physical examination, by assessing the vital signs (BP, pulse, body weight, and temperature), neurological examinations and relevant laboratory tests. These parameters were examined at the subsequent study visits for up to one year. Any adverse effects which were observed were recorded in the ‘Adverse Drug Event Reporting Form’ which was prepared by the CDSCO, Govt. of India. The causalities of the event were assessed by the World Health Organization–Uppasala Monitoring Centre (WHO-UMC) [6]. For the analysis of the safety, all the data which was related to various adverse drug reactions were subjected to the Chi-Square Test, with a p-value of less than 0.05, which was considered to indicate a statistical significance.
RESULTS
Ninty one prescriptions (56.87%) among the 160 which were studied, contained SSRIs, while 13 (8.12%) contained TCAs and 32 (20%) contained newer antidepressants (SNRI/ NDRI). SSRI plus NDRI and SSRI plus TCA were used in 17 (10.62%) and 7 (4.37%) patients respectively. Among the 136 cases which received the Monotherapy, 37 (23.12%) received Escitalopram, 33(20.62%) subjects received Fluoxetine, 19 (11.87%) subjects received Sertraline and 2 (1.25%) received Paroxetine. 11 (6.87%) received Amitriptyline, 2 (1.25%) received Dotheipin, 9 (5.62%) received Venlafaxine, 15 (9.37%) received Duloxetine and 8 (5%) received Bupropion. It was observed that the most frequently prescribed antidepressant was Escitalopram (in 37 cases i.e. 23.12%) and that the most frequently prescribed newer antidepressant was Duloxetine (in 15 cases i.e. 9.37%) [Table/Fig-1].
utilisation pattern of different antidepressant drugs in a psychiatry outpatient department
| Sl. No | Specific Drug | Frequency | Percent |
|---|
| 1 | Fluoxetine | 33 | 20.62 |
| 2 | sertraline | 19 | 11.87 |
| 3 | Escitalopram | 37 | 23.12 |
| 4 | Paroxetine | 2 | 1.25 |
| 5 | Amitriptyline | 11 | 6.87 |
| 6 | Dotheipin | 2 | 1.25 |
| 7 | Venlafaxine | 9 | 5.62 |
| 8 | Duloxetine | 15 | 9.37 |
| 9 | Bupropion | 8 | 5 |
| 10 | Fluoxetine+Bupropion | 8 | 5 |
| 11 | Escitalopram+Bupropion | 2 | 1.25 |
| 12 | Sertraline+Bupropion | 7 | 4.37 |
| 13 | Sertraline+Amitriptyline | 2 | 1.25 |
| 14 | Fluoxetine+Amitriptyline | 4 | 2.5 |
| 15 | Escitalopram+Amitriptyline | 1 | 0.62 |
| Total | 160 | 100 |
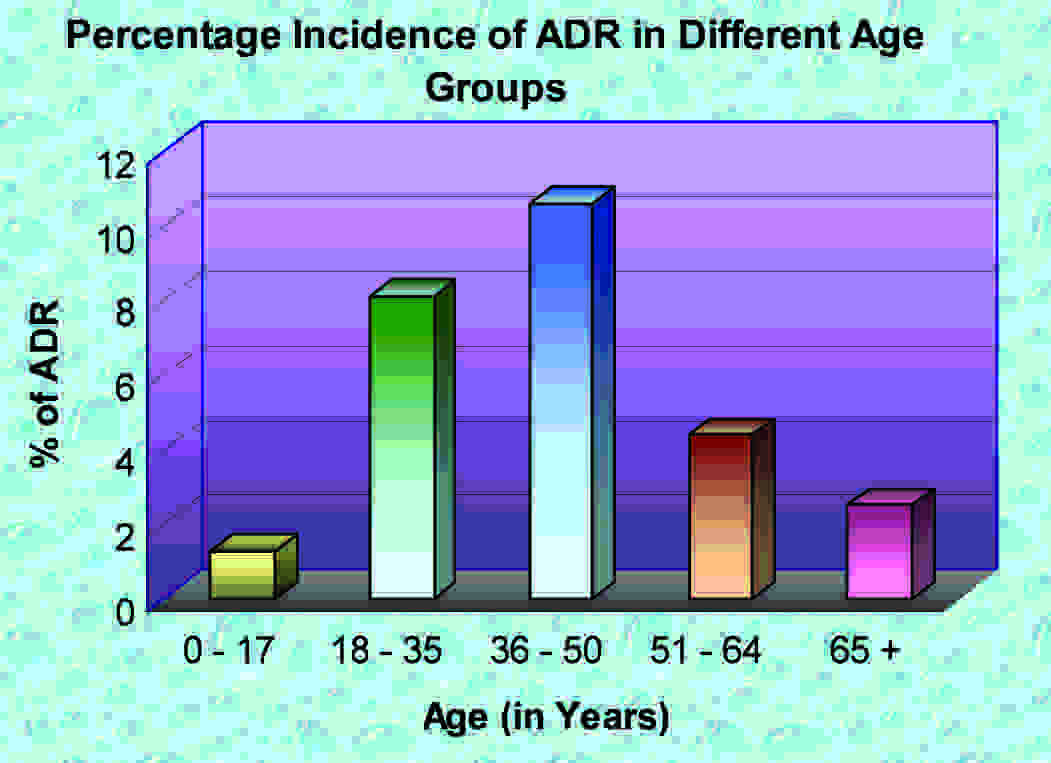
Adverse drug reactions were maximally observed in the age group of 36–50 years (10.62%) and it was minimum in the age group of 0 – 17 years (1.25%) [Table/Fig-2]. Adverse drug reactions occurred in most of the systems like the CVS and the Neurological, Genitourinary and the Gastrointestinal systems. 28.57% patients who took SSRIs had adverse drug reactions, whereas 58.84% patients who took TCAs, 28.12% patients who took the newer antidepressants and 5.88% patients who took SSRIs plus NDRI had them. After the drug administrations, 7 (7.7%) subjects out of 91 who took SSRIs like Escitalopram and Sertraline and 4 (30.37%) out of 13 who took TCAs like Amitriptyline developed insomnia, whereas 2 (15.38%) subjects who took TCAs and 1 (1.1%) who took SSRIs developed blurring of vision. Fatigue was seen in 2 (2.2%) subjects who were on SSRIs and 2 (6.25%) who were taking the newer antidepressants like SNRIs (Duloxetine), whereas sweating was seen only in 1 (1.1%) patient who was on an SSRI. Only 1 (7.69%) out of 13 patients who were on TCAs developed postural hypotension and 1 (7.69%) developed tachycardia. 3 (3.29%) subjects among 91 who received SSRIs and 4 (30.77%) subjects among 13 who received TCAs developed dry mouths, whereas 4 (4.39%) subjects who were on SSRIs and 3 (9.37%) who were on the newer antidepressants complained of nausea. Headache was seen in 2 (2.2%) persons out of 91 subjects who received SSRIs and only in 1 (1.1%) subject who was on SSRIs and 2 (6.25%) who were on the newer antidepressants like Douloxetine complained of tremors. SSRIs produced severe agitation than the TCAs. Nervousness was found in 4 patients who were on SSRIs (4.39%), whereas anxiety was seen in 7 patients who were on SSRIs (7.69%) like Escitalopram and Sertraline and in 2 patients who were on the newer antidepressants like venlafaxine (6.25%). Urinary hesitancy occurred in 1 (7.69%) out of 13 patients who were on TCAs and 4 (4.39%) patients out of 91 who received SSRIs complained of sexual dysfunction. The commonest ADR was insomnia, followed by agitation and anxiety [Table/Fig-3]. Out of 160 patients who were on antidepressants, 43 reported with at least one ADR.On causality assessment, 31 were found to belong to the probable category and 42 were found to belong to the possible category, according to the WHO-UMC scale. No case could be labeled as certain, as a rechallenge was not attempted.
Different ADRs with different group of Antidepressants
| ADR | SSRI(91) | TCA(13) | NEWER(32) | TOTAL |
|---|
| Insomnia | 7 | 4 | - | 11 |
| Blurring of vision | 1 | 2 | - | 3 |
| Fatigue | 2 | - | 2 | 4 |
| Sweating | 1 | - | - | 1 |
| Postural Hypotension | - | 1 | - | 1 |
| Tachycardia | - | 1 | - | 1 |
| Dry mouth | 3 | 4 | - | 7 |
| Nausea | 4 | - | 3 | 7 |
| Loss of appetite | 2 | - | - | 2 |
| Headache | 2 | 1 | - | 3 |
| Tremor | 1 | - | 2 | 3 |
| Agitation | 11 | - | 1 | 12 |
| Nervousness | 4 | - | - | 4 |
| Anxiety | 7 | - | 2 | 9 |
| Urinary hesitancy | - | 1 | - | 1 |
| Sexual dysfunction | 4 | - | - | 4 |
| Total | 49 | 14 | 10 | 73 |
Incidence of ADRs in different age groups
DISCUSSION
A majority of the studies which are related to antidepressant drugs merely analyze the drug utilization pattern, so that an objective data on the preference of any particular group over the other can be known. This study highlighted the incidence and nature of the adverse drug reactions which were associated with antidepressant drugs, so that a correlation between the ADR and the pattern of drug use could be established. In this study, it was found that among all the adverse drug reactions, the general adverse drug reactions like blurring of vision, insomnia, sweating and fatigue were more common in the study population.Out of these adverse reactions, insomnia was more common with the TCAs (30.77%) than with the SSRIs (7.7%). However, sweating (1) & loss of appetite (2) were found only in the patients who received SSRIs.
The cardiovascular side effects like tachycardia and postural hypotension were associated with the TCAs (7.69%). While the gastrointestinal side effects were studied, the TCAs were found to be most commonly associated with dry mouth (30.77%) than the SSRIs (3.29%), whereas nausea was found to be most commonly associated with the SSRIs. The neurological side effects like headache were more common with the TCAs (7.69%), whereas tremor was more associated with the SSRIs (1.1%).
The SSRIs showed more psychiatric adverse drug reactions like agitation (12.09%), nervousness (4.39%) and anxiety (7.69%). A similar study concluded that agitation was seen in 52% of the study population who received Fluoxetine and Escitalopram in comparison to the newer antidepressants like Venlafaxine [7].
Sexual dysfunction (4.39%) was most commonly associated with the patients who were on SSRIs than with the patients who were on TCAs in our study population. But, urinary hesitancy was observed in 7.69% cases which were on TCAs. Similar studies which were done, have observed that sexual dysfunction was a common side effect of nearly all the standard antidepressants like SSRIs and also of some of the newer drugs [8]. Some of the newer antidepressants such as Bupropion, may be effective alternatives without as high a risk for this problem [9]. The psychotropic drugs like SSRIs are the 3rd after the typical and the atypical antipsychotics in causing ADRs [10]. ADR rates were higher for TCAs (imputed in 1.0% of patients) and lower for MAO inhibitors and SSRIs (0.7% for both, respectively 0.3% and 0.4%) [11].
The TCAs were associated with the known risks, such as increased liver enzymes, urinary retention or orthostatic hypotension. In the SSRI-treated patients (non-delirious) the psychic and the neurological ADRs were the most prominent ones [11].
Antidepressants, antipsychotics and mood stabilizers are associated with adverse effects which can affect the compliance and the course of the treatment in mental disorders [12].
CONCLUSION
Agitation, anxiety and insomnia are the common ADRs which are associated with the use of antidepressants. This study offered a representative profile of the ADRs which could be expected in the psychiatry outpatients department. The side effects like dry mouth and blurring of vision are more common with the TCAs, whereas agitation and sexual dysfunction are common with the SSRIs and nausea and fatigue are more common with the newer antidepressants.
LIMITATIONS AND FUTURE IMPLICATIONS
The sample size was small, the study subjects were confined to the OPD only and the study was conducted only for a short period at a single centre only.
But at the same time, by knowing the incidence, the demographic profile and the causative agents of the various ADRs, many common ADRs which are caused by antidepressants can be avoided. This study represented the adverse effects scenario in the patients of eastern India and it provided the baseline data for its comparison with other similar studies which were done in different parts of the country. Awareness should be created among the physicians as well as the paramedical staff regarding the various ADRs which are caused by antidepressants, so that the morbidity can be reduced. Lastly, this study may act as a further step for strengthening the pharmacovigilance activities, for providing information regarding the management of ADRs and for making the drug therapy safer and more rational.