INTRODUCTION
Ozone therapy can be defined as a versatile bio-oxidative therapy in which oxygen/ozone is administered via gas or it is dissolved in water or an oil base to obtain therapeutic benefits in a diseased living system. Now-a-days, ozone gas which is dissolved in an oil base is gaining importance due to its excellent curative results, simple application, longer-term effects and non toxic nature [1–4]. In the past years, the therapeutic effect of ozonated oil was attributed to its antibacterial, antifungal, antiviral, antiparasitic, antihypoxic, analgesic and immunomodulatory effects on biological systems [1, 5–12]. In the present context of time, these empirical mechanisms of actions are supported by few published case reports and scientific studies, which restrict the application of the ozonated products in different fields of medicine and dentistry. With the few published and anecdotal information on ozonated oil and its therapeutic effect on the biological tissues, we designed a therapeutic approach for an exophytic fibrous enlarged lesion on the human gingiva. As a consequence, a human case was selected, who presented with an exophytic gingival lesion (which was indicated for an excisional biopsy), to which ozonated oil could be applied and for which further morphometrical and histopathological evaluations could be made. Thus, an experimental attempt was made to provide initial information about the morphometrical and the histological changes which occur after topical ozonated oil application on an exophytic gingival lesion.
CASE REPORT AND METHODOLOGY
We selected a 42 years old female patient who was referred to our department with the chief complaint of an enlarged lesion on her upper anterior gingiva [Table/Fig-1]. The patient revealed that initially, the lesion had been small, but that it had gradually increased in size since the past 6 months. The lesion was mild to moderately painful during brushing or mastication. It was not associated with pregnancy or any other systemic outcomes. The patient gave a history that she was systemically healthy and that she was not on any medication. On intraoral examination, an enlarged lesion was seen, which was confined to the attached gingiva of the maxillary left central and lateral incisors. The lesion was 10 × 14 mm in size, exophytic, pedunculated, roughly oval, reddish, and ulcerated. On palpation, the lesion was found to be firm and fibrotic in consistency, with bleeding on provocation. The overall oral hygiene status was good, with minimal deposition beneath the lesion or around the associated teeth.
Gingival lesion before treating with ozonated oil. Note the surface ulceration and inflammatory sign on the lesion.

A treatment plan was designed, which included, the therapeutic application of ozonated oil, followed by excisional biopsy and a histopathologic evaluation as a diagnostic and a therapeutic approach for treating the lesion. The patient was scheduled for recall appointments. As a part of the routine procedure, a complete blood examination was done and further procedures were carried out only after the confirmation of all the normal haematological values. Furthermore, an intraoral periapical radiograph (IOPAR) of the associated tooth/ lesion was taken, to rule out any bony or periapical pathology which was associated with the tooth structure. On the initial appointment, no scaling or mechanical debridement was done. Only the relevant medical history and the complete dental history was recorded, which were accompanied by a thorough clinical examination of the subjected lesion. Preoperative photographs were taken for image analysis. Then, a one-week appointment was scheduled for implementing the therapeutic application of ozonated oil and for training the patient as to how to apply the oil on the enlarged lesion. Before implementing the therapeutic application of ozonated oil on the lesion, a small section of the tissue mass, which measured 9.8 ×3.2 mm was excised from the distal margin of the exophytic gingival lesion under local anaesthesia (2% lignocaine, 1:80000 adrenaline) [Table/Fig-2]. The obtained sectioned specimen was submitted for a histopathological analysis. This was done as an attempt to take a control from the same lesion with which the final histopathological outcome which was obtained after the application of ozonated oil, could be compared.
Gingival lesion after excising the control specimen from the distal margin. Dotted area showing tissue mass excised.

Two ml of ozonated olive oil which was estimated at 80μg/ml was applied on the lesion. For home use, 21 premeasured disposable plastic vials which contained 2 ml of ozonated olive oil was given to the patient. The patient was advised to apply 2 ml of ozonated oil with a sterile cotton bud on the lesion site three times daily for 7 days, after meals. No antibiotics and/or analgesics were prescribed along with the prescribed ozonated oil.
On the next one-week recall visit, the patient’s centred clinical outcome, like pain and discomfort were recorded. Photographs of the lesion were taken for image analysis. Subsequently, the patient was prepared for the final biopsy procedure. A measured volume of ozonated oil (0.5 ml) was applied on the lesion, followed by complete excision of the gingival lesion under local anaesthesia (2% lignocaine 1:80000 adrenaline).The excised tissue specimen was formalin fixed and stained with the haematoxylin and eosin stain for the histopathological analysis. After the final biopsy procedure, the patient was again re-scheduled for the next week’s appointment and a further evaluation of the post-excised wound on the gingival surface was done.
Images were taken at each time interval of the recall visits for a computerized morphometrical analysis to evaluate the difference in the morphological size of the lesion. The methodology was adopted as has been described in our previous paper [12]. Finally, the obtained morphometrical data of the pre-ozone treated lesion and the post-ozone treated lesion were compared and the difference was considered as the change in the morphological size of the lesion.
RESULTS
After one week’s application of ozonated oil on the gingival lesion, the clinical picture demonstrated a well-localized, slightly shrunk gingival mass, which was less firm on palpation. The surface foci of the ulcerations were greatly reduced, with less sign of acute inflammation on the surface as compared to those of the previous pre-ozone treated lesion.
During the final biopsy procedure of the post-ozone treated lesion, a dramatic reduction in the bleeding was observed, when it was compared to the previous experience of bleeding during the excision of the marginal gingival specimen which was taken as the control [Table/Fig-3]. After the complete excision of the tissue, the final post-excised wound, healed uneventfully and it revealed no sign of scarring or other adverse outcomes [Table/Fig-4].
Final excision of enlarged lesion. Note the reduced bleeding during surgical excision after application of 0.5 ml of ozonated oil on the lesion during the procedure.

Gingival site after final excision of enlarged lesion.

The morphometrical changes revealed a decrease in the mean area of the gingival lesion. The original lesion was of size 140 mm2. After the excision of the control specimen (31.36 mm2), the remaining size of the lesion was 108.64 mm2. After one week of the ozone application, the lesion size was 96.35mm2, that demonstrated a reduction of 12.29 mm2 in the ozone treated lesion.
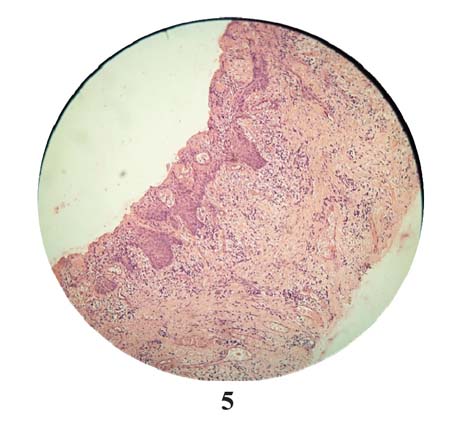
The histopathological examination of the pre-ozone treated specimen revealed stratified squamous epithelium with multiple foci of surface ulcerations. The connective tissue stroma showed thick collagen fibres in bundles with plump fibroblast cells. Dense chronic inflammatory cells were evident, which consisted of plasma cells, lymphocytes, and mast cells. Few blood vessels were also seen in the connective tissue stroma. From the observed histopathological features, the diagnosis of an inflammatory fibrous hyperplasia was confirmed [Table/Fig-5].
Pre-ozone treated histopathological section demonstrating numerous chronic inflammatory cells in highly collaginized connective tissue stroma. Ulcerated overlying epithelium with minimal keratinization [H&E, 10×].
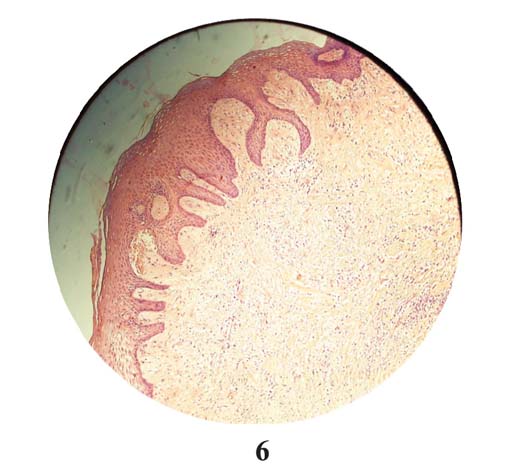
The post-ozone treated specimen revealed well-keratinized stratified squamous epithelium. There were fewer foci of surface ulcerations, with regenerating new epithelial cells covering the ulcerated areas. The connective tissue stroma showed less collagen fibres in bundles, with fewer fibroblast cells. There was a remarkable reduction in the number of chronic inflammatory cells in the connective tissue stroma [Table/Fig-6].
Post-ozone treated histopathological section demonstrating reduced chronic inflammatory cells with reduced collagen fibers bundles in connective tissue stroma. Overlying epithelium is well keratinized with generated new keratinocytes. [H&E, 10×].
DISCUSSION
This paper has reported a case in which ozone therapy was used in the form of topical ozonated oil on an exophytic enlarged gingival lesion and the therapeutic benefits which were obtained after short-term applications.
In the present study, the patient centred clinical benefits were observed after one-week of application of the ozonated oil on the enlarged gingival lesion. The patient reported less pain and discomfort, improved clinical inflammatory signs, and reduced ulcerations on the overlying epithelium of the lesion, with an improved sign of healing. The exact mechanism behind it is still unclear.
Few authors [3,4,9] have proposed that the base oils (olive oil, sunflower oil, coconut oil, etc.), during their ozonation processes, trap O3 in the form of a stable ozonide. Thus, the produced stable ozonide, when it encounters the warm exudates of the wound, slowly decomposes to reactive ozone. Which it readily dissolves in water, it generates hydrogen peroxide and lipoperoxides, which can explain its prolonged disinfectant and stimulatory activity on ulcerated chronic wounds [4]. Moreover, the phenomenon of an improved wound healing after the ozone therapy has been related to the rapidly changing cell types and to the release of cytokines that modulate the complex healing process [10–12].
The reduced inflammatory sign can be attributed to the oxidizing potential of ozone [13]. Ozone has been shown to oxidize prostaglandins [14]. Prostaglandin is a known biologically active compound that participates in inflammatory reactions and thus, the local application of ozonides may promote the removal of inflammatory phenomena.
The reduced pain can be related to the membrane-stabilizing effect of ozone on the pain receptor cells. Ozone has the potential to increase the excitability threshold of the pain receptor cell membranes. The direct oxidation of proteins (algopeptides) is another mechanism, which may be responsible for the reduction in the pain [15]. Algopeptides are proteins which are formed in the place of tissue damage and they help in the transportation of the pain impulses to the brain.
There is an evidence [10], where, an accelerated human oral wound healing with significantly improved postoperative outcomes after the application of ozonated water has been documented. The application of ozonated water had accelerated the wound healing in the oral cavity within the first 48 hours as compared to placebo water, resulting in an earlier epithelial wound closure after 7 days. Our study also supports the findings of Patel et al., [2,10,12] where an improved healing was found after one week of the ozone application.
The antimicrobial efficacy of ozonated oil is another mechanism, which can be attributed to the improved patient centred clinical outcomes. Various in vitro and in vivo studies [2,16–18] have revealed that when the ozonized oil encounters a microorganism, a severe alteration in the cytoplasm of the microbial cells occurs, consequently leading to membrane rupture and leakage of the cytoplasmic contents.
During the final excision of the post-ozone treated enlarged lesion, a dramatic reduction in the bleeding was observed. However, the exact mechanism is not clear, but it could be ascribed to the haemostatic changes that have been explained in a previous study [19]. This in vivo study indicated that the arrest of the bleeding under the influence of ozone, is due to the formation of a fibrin membrane on the surface of the flowing blood, leading to a rapid and an effective haemostasis. These haemostatic changes have also been attributed to increased releases of the growth factors after the ozone treatment, consequently leading to vasoconstriction and platelet aggregation.
The morphometrical analysis revealed a reduction in the mean area of the gingival lesion after the application of ozonated oil. A reduction in size from 108.64 mm2 to 96.35mm2, with a mean difference of 12.29 mm2 was observed. The exact mechanism behind the shrinkage of the enlarged lesion is still unclear. The reason could be ascribed to a reduction in size of the collagen fibres which were in bundles and the inflammatory cells infiltrate in the connective tissue stroma. These histopathological changes were confirmed by a histopathological examination of the sectioned lesion after the ozonated oil application. An enhanced production of the cytokines may have stimulated the fibroblast cells to activate phagocytary action on the excessive collagen fibers which were lying in the connective tissue stroma.
The histopathological analysis of the post-ozone treated sectioned mass displayed an improved keratinization over the epithelial cell layer and over the regenerating new epithelial cells which covered the ulcerated areas. These changes can be attributed to the proliferation of the keratinocytes and the enhanced mitotic turnover rates of the epithelial cells. The connective tissue stroma displayed reduced bundles of the collagen fibers, which were earlier highly collagenized with numerous plump fibroblasts [20–22].
In the present study, we observed the dual nature of ozone, where on one hand it stimulated wound healing, which resulted in wound contraction and improved post-operative outcomes. Whereas on the other hand, it showed lethal action on the excessively proliferated fibroblasts in the connective tissue stroma of the enlarged fibrous ginigva. This action is still unclear and it needs to be verified in the future researches.
The current study represents a unique methodology for analyzing a lesion and its outcomes after the application of the ozone therapy. A control histopathological specimen from the same lesion was taken, which provided the best control rather than those of the other tissues of the same or different individuals which were taken as the controls. The morphometrical analysis was done by using a computer software with a generated standardized scale setting technique. The computerized morphometrical analysis is a well-recognized, highly sensitive and an accurate method which can be used in such morphometrical procedures.
CONCLUSION
The result outcome of the present study demonstrated the potential benefits which were obtained from the topical ozone therapy on the enlarged fibrous gingival lesion. Improved patient centred outcomes, improved clinical signs of the inflammation, less bleeding during the surgical excision, morphometrical changes and histological changes were some potential benefits which have been documented in the present study. The observed potential benefits, if they are supported by a higher level of evidence in the future, can provide a scientific rationale behind the ozone therapy and its incorporation in the modern practice of dentistry.
[1]. Azapazhooh A, Limeback H, The application of ozone in dentistry: a systematic review of the literatureJ Dent 2008 36:104-16. [Google Scholar]
[2]. Patel PV, Patel A, Kumar S, Holmes JC, Effect of subgingival application of topical ozonated olive oil in the treatment of chronic periodontitis: a randomized, controlled, double blind, clinical and microbiological studyMinerva Stomatol 2012 61:381-98. [Google Scholar]
[3]. Travagli V, Zanardi I, Valacchi G, Bocci V, Ozone and Ozonated Oils in Skin Diseases: A ReviewMediators Inflamm 2010 6:10-41. [Google Scholar]
[4]. Travagli V, Zanardi I, Bocci V, Topical applications of ozone and ozonated oils as anti-infective agents: an insight into the patent claimsRecent patents on anti-infective drug discovery 2009 :4130-42. [Google Scholar]
[5]. Lamberto R, Mawsouf M N, Menéndez S, Olga S, León Sánchez G. M, Hernández F, Ozone therapy: Clinical and basic evidence of its therapeutic potentialArch Med Res 2008 39:17-26. [Google Scholar]
[6]. Agapov V S, Smirnov S N, Shulakov V V, Tsarev V.N, [Ozone therapy in treatment of local sluggish suppurative inflammation of maxillofacial soft tissues]Stomatologiia Mosk 2001 80:23-27. [Google Scholar]
[7]. Paulesu L, Luzzi L, Bocci V, Studies on the biological effects of ozone: Induction of tumor necrosis factor TNF-alpha on human leucocytesLymphokine Cytokine Research 1991 54:09-412. [Google Scholar]
[8]. Bocci V, Valacchi G, Corradeschi F, Fanetti G, Studies on the biological effects of ozone: 8. Effects on the total antioxidant status and on interleukin-8 productionMediators Inflamm 1998 7:313-17. [Google Scholar]
[9]. Rae Ian D, Ozonised oils as disinfectantsAmbix 2006 53:3-20. [Google Scholar]
[10]. Patel PV, Kumar S, Vidya GD, Patel A, Holmes JC, Kumar V, Cytological Assessment of Healing Palatal Donor Site wound and Grafted Gingival Wound after Application of Ozonated Oil: An Eighteen Months Randomized Controlled Clinical TrialActa Cytol 2012 56:277-84. [Google Scholar]
[11]. Werner S, Grose R, Regulation of wound healing by growth factors and cytokinesPhysiol Rev 2003 83:835-70. [Google Scholar]
[12]. Patel PV, Kumar V, Kumar S, Patel GD, Therapeutic Effect of Topical Ozonated Oil on Epithelial Healing of Palatal Wound Site: A Planimetrical and Cytological StudyJ Investig Clin Dent 2011 2:248-58. [Google Scholar]
[13]. Klichowska-Palonka M, Bachanek T, Ozone therapy for labial and oral inflammationsPolish Journal of Environmental Studies 2006 15:211-13. [Google Scholar]
[14]. Friedman M, Madden MC, Samet JM, Koren HS, Effects of ozone exposure on lipid metabolism in human alveolar macrophagesEnviron Health Perspect 1992 97:95-101. [Google Scholar]
[15]. Steppan JC, Boxley Murphy K, Muto M, Balagurunathan K, Meaders T, Ozone’s mechanism of action for relieving pain associated with herniated intervertebral discsJ Vasc Interv Radiol 2009 20:S16-S17. [Google Scholar]
[16]. Lee Seung-Jae, Jeun-Youb Ahn, Toshiaki Miura, Mun-Yhung Jung, Dong-Seong Choi, [Evaluation of Antimicrobial Activity and Mutagenicity of Ozonized Olive Oil]Korean Journal of Food Science and Technology 2006 38:805-09. [Google Scholar]
[17]. Lezcano I, Nuñez N, Espino M, Gómez M, Antibacterial activity of ozonized sunflower oil oleozón against staphylococcus aureus and staphylococcus epidermidisOzone Science Engineering 2000 22:207-14. [Google Scholar]
[18]. Fernandez I, Curtiellas V, Sánchez E, Gómez M, In vitro antimicrobial ctivity of ozonized theobroma oil against candida albicansOzone Science Engineering 2006 28:187-90. [Google Scholar]
[19]. Kashperskii YP, Adamyan AA, Makarov VA, Glyantsev SP, Zhukov VA, Study of the hemostatic properties of gaseous ozoneBull Exp Biol Med 1995 120:708-11. [Google Scholar]
[20]. Coletta RD, Almeida OP, Reynolds MA, Sauk JJ, Alteration in expression of MMP-1 and MMP-2 but not TIMP-1 and TIMP-2 in hereditary gingival fibromatosis is mediated by TGF-β1 autocrine stimulationJ Periodontal Res 1999 34:457-63. [Google Scholar]
[21]. Valacchi G, Pagnin E, Okamoto T, Corbacho A, Olano ME, Davis PA, Induction of stress proteins and MMP-9 by 0.8ppm of ozone in murine skinBiochem Biophys Res Commun 2003 30:5741-46. [Google Scholar]
[22]. Valacchi G, Fortino V, Bocci V, The dual action of ozone on the skinBr J Dermatol 2005 153:1096-100. [Google Scholar]