The Carotid Intima Media Thickness: A Predictor of the Clincal Coronary Events
Jinzy Mariam George1, Raghavendra Bhat2, K. Mohan Pai3, Arun S.4, Jayakumar Jeganathan5
1 Senior Resident, Department of Medicine, Kasturba Medical College Mangalore, Manipal University, India.
2 Professor and HOD, Department of Medicine, Kasturba Medical College Mangalore, Manipal University, India.
3 Professor, Department of Medicine, Kasturba Medical College Mangalore, Manipal University, India.
4 Associate Professor, Department of Medicine, Kasturba Medical College Mangalore, Manipal University, India.
5 Associate Professor, Department of Medicine, Kasturba Medical College Mangalore, Manipal University, India.
NAME, ADRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Jinzy Mariam George, KMC staff Quarters (RNE), Room cIII4B, Lighthouse Road, Mangalore 575001 (India).
Phone: 9620814619
E-mail: jinzygeorge@gmail.com
Background: The Carotid Intima-Media Thickness (CIMT) is a simple and an inexpensive tool which can be used to assess the cumulative effect of atherosclerotic risk factors and it is also an independent predictor of the future cardiovascular risk. Nevertheless, criticism has been raised throughout the scientific community, based on the observations which indicated a weak correlation between CIMT and coronary atherosclerosis.
It has been suggested by the International Atherosclerosis Project, that the atherosclerotic process occurs at the same time in the carotid, cerebral and the coronary arteries. Measurement of the Carotid Intima-Media Thickness (CIMT) of the Common Carotid Artery (CCA) by B-mode ultrasound was found to be a suitable non-invasive method, to visualize the arterial walls and to monitor the early stages of the atherosclerotic process.
Aim: This study sought to determine the usefulness of B-mode ultrasound as a non-invasive marker to examine the association between CIMT and the extent and the severity of coronary artery disease and its association with the cardiovascular risk factors, if any.
Methods: A cross-sectional study was done among hundred cases and hundred age and sex matched controls who were in the age group of 30-65 years. The cases included those who had undergone coronary angiography. The controls included non-diabetic non-hypertensives with no cardiovascular risk factors. The CIMT was assessed by using a 7MHz linear array transducer. Fasting blood samples were collected for measuring the blood sugar and the lipid profiles.
Results: The statistical analysis was done by using the Student’s t test and ANOVA and a p value of <0.001 was considered to be significant. The Average Carotid Intima Media Thickness (AVCIMT) was higher in the cases (0.90 vs 0.47 in controls, p<0.001, very highly significant). The AVCIMT was found to be higher in those with triple vessel disease (1.00mm) <double vessel disease (0.91mm) <single vessel disease (0.82mm) <normal coronaries (0.65mm).
Conclusion: The easy applicability and the non invasive nature of B-mode ultrasonography make it suitable for use as a surrogate endpoint for measuring the atherosclerotic burden in people with cardiovascular risk factors. Even in this present study, we found a significant association between the extent of carotid atherosclerosis which was measured by B-mode ultrasound, and the presence, its extent, or the lack of coronary atherosclerosis which was documented by coronary angiography.
Atherosclerosis, Carotid, Intima, Coronary
INTRODUCTION
During the past 30 years, the Coronary Artery Disease (CAD) rates have doubled in both urban and rural India, while they have been halved in the United States. By 2015, cardiovascular diseases are expected to account for 34% of the male deaths and 32% of the female deaths, amounting to a total of 1.5 million deaths [1].
It is imperative to shift the focus to disease prevention rather than palliation. Prevention requires an early identification of the individuals who are at a risk of developing cardiovascular disease, but are clinically asymptomatic, so that intensive preventive measures may be instituted to arrest the progression of the disease. The various diagnostic modalities which are being used currently (exercise electrocardiography, stress echocardiography, thallium scanning and coronary angiography) can detect atherosclerotic disease only when it becomes well advanced and occlusive [2].
The Carotid Intimal Media Thickness (CIMT) measurement is a promising tool for detecting atherosclerosis in its pre-occlusive phase [3–6].
An increase in the Carotid Intimal Media Thickness (CIMT) is associated with an increased risk of ischaemic heart disease and cerebrovascular disease [7,8]. Atherosclerosis is an inevitable accompaniment of ageing and its rate of development depends on several factors. The well known risk factors for accelerated atherosclerosis include hypertension, smoking, dyslipidaemia and dysglycaemia. As several practical life style and pharmacological interventions for attenuating atherosclerosis are available, it is necessary to identify the subjects who are at a risk of developing atherosclerosis early, especially since subclinical atherogenesis has become an emerging risk factor for coronary artery disease [9]. Atherosclerosis, unless it is in a severe form, is often asymptomatic, so that a direct examination of the vessel wall is necessary to detect the affected individuals in the early stages. It has been suggested by the International Atherosclerosis Project that the atherosclerotic process occurs at the same time in the carotid, cerebral and the coronary arteries [10]. Measurement of the Carotid Intima-Media Thickness (CIMT) of the Common Carotid Artery (CCA) by B-mode ultrasound was found to be a suitable non-invasive method for visualizing the arterial walls and for monitoring the early stages of the atherosclerotic process [11–13].
The purpose of this study was to correlate the carotid intimal thickness and the extent of CAD, as well as the effect of various risk factors on IMT in a subset of the Indian population, which differed from the western counterparts with respect to the risk factors profile, mortality and the morbidity.
MATERIAL AND METHODS
The study design was a cross sectional study which was carried out for a duration of about 2 years, from August 2009 to July 2011.
The study population included 200 subjects;100 cases and 100 controls who were in the age group of 30-65 years.
Inclusion Criteria
Age 30-65 years, those who underwent elective/emergency coronary angiography, following the diagnosis of Acute coronary syndrome (unstable angina, Non ST Elevation Myocardial infarction/ST Elevation Myocardial Infarction).
Controls
Normal healthy subjects with no traditional cardiovascular risk factors.
Exclusion Criteria
Diabetic subjects who were on insulin therapy.
Patients with a history of pancreatitis, pancreatectomy, haemochromatosis, Cushing’s syndrome, Glucagonoma, hyperthyroidism and hypothyroidism.
Patients who were on medications which can elevate the blood glucose levels-glucocorticoids, thyroidhormones, diazoxide, diuretics, Beta adrenergic agonists and nicotinic acid.
A history of Coronary Artery Bypass Grafting (CABG), carotid surgery, endarterectomy, cerebrovascular accidents and peripheral vascular disease.
The history with regards to smoking was taken. A clinical examination which included the assessment of the Body Mass Index (BMI) which was calculated as the body weight (kg) divided by the squared height (m2) was undertaken and the blood pressure (systolic and diastolic) was taken with the use of a mercury sphygmomanometer.
Ultrasound Evaluation
B mode ultrasound was done with the use of a 7 MHz linear array transducer by a single radiologist following a standard operating procedure. The scanning included the left and right carotid arteries. The carotid artery was focussed in the far wall and the 3 segments were identified on each side: the distal 1.0cm of the common carotid proximal to the bifurcation, the carotid bulb and the proximal 1.0 cm of the internal carotid artery. The average carotid intima media thickness was calculated by taking the mean of all these three values.
Biochemical Studies
Fasting blood samples were collected the morning for the analysis of the following parameters by using standard techniques:
FBS (Fasting Blood Sugar)
TC (Total Cholesterol)
TG (Triglycerides)
HDL (High Density Lipoprotein)
LDL (Low Density Lipoprotein)
RESULTS
The statistical analysis was done using the Student’s t test and ANOVA and a p value of <0.001 was considered to be significant.
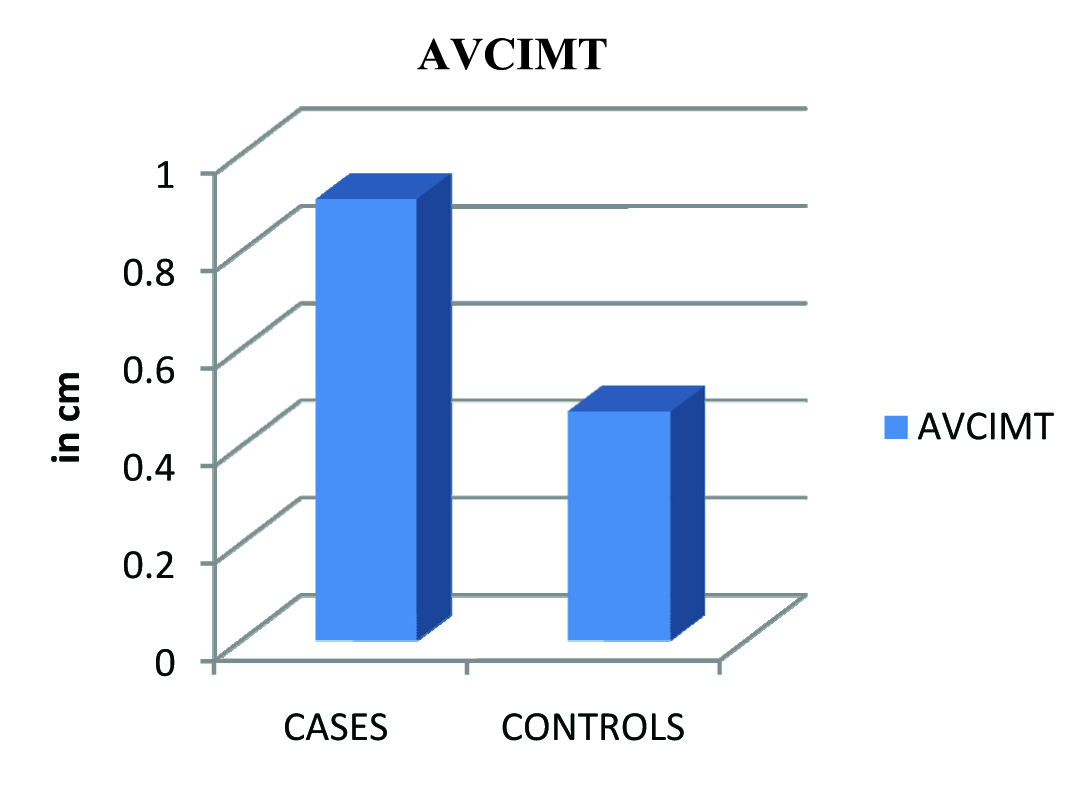
The mean age of the cases was 49.82 years and that of the controls was 44.30 years. There were 71 males and 29 females. Among the controls, there were 57 males and 43 females. 81 cases were diabetics, and 87 had hypertension. The AVCIMT of cases and controls in our study is shown in [Table/Fig-1] and [Table/Fig-2].
Average Carotid intima media thickness(AVCIMT)
| Group | N | Mean | Std Deviation | t |
|---|
| Cases | 100 | 0.9071 | 0.11191 | 36.21200 |
| Controls | 100 | 0.4704 | 0.4154 | p <0.001 vhs |
The average carotid intimal media thickness was higher in cases(0.90mm Vs 0.47mm)p<0.001( very highly significant)
Average Carotid intima media thickness(AVCIMT)
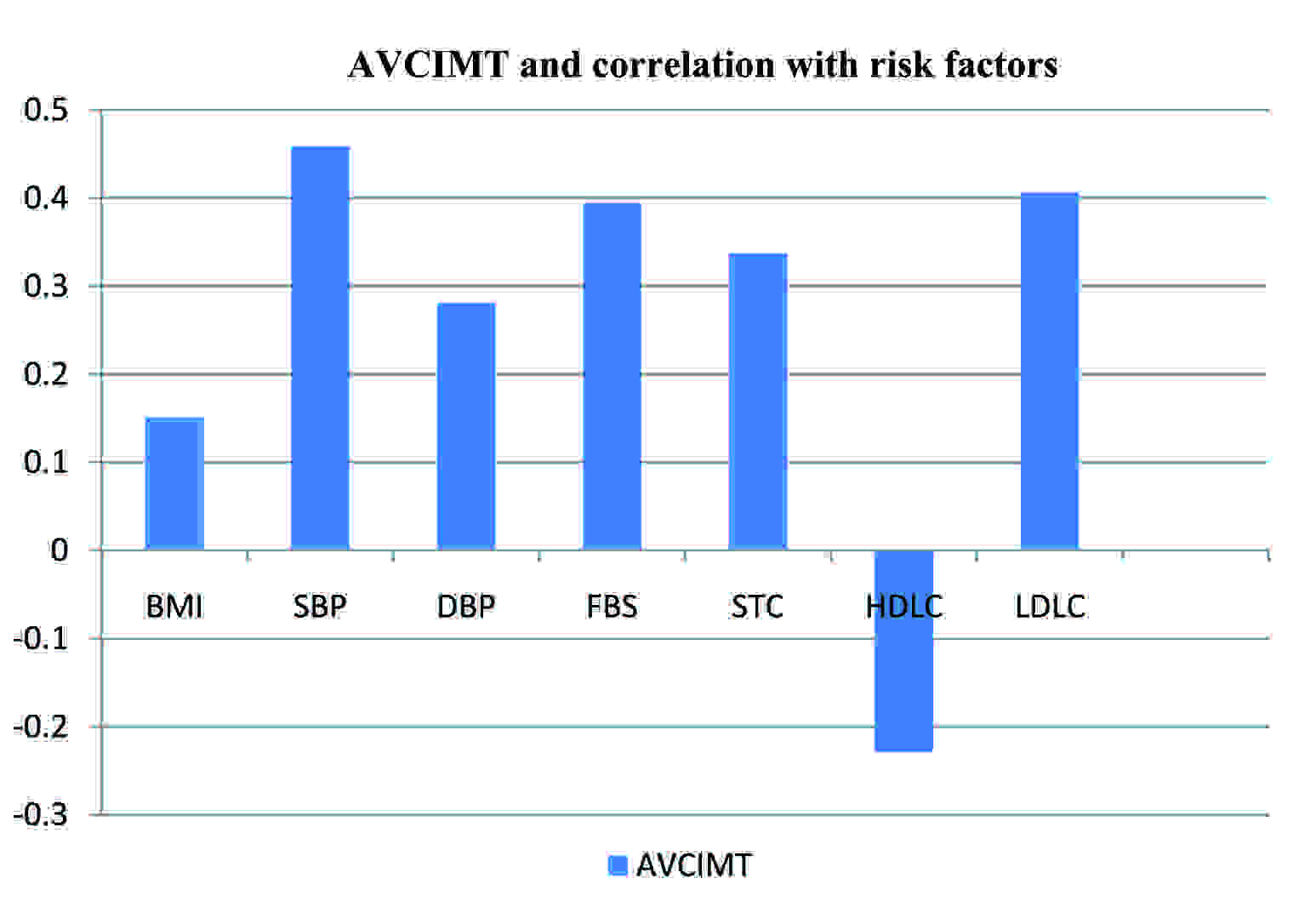
In a comparison between the average CIMT and the risk factors, the association with smoking was not found to be significant (p=0.737). As seen in [Table/Fig-3] and [Table/Fig-4], the observations were that the AVCIMT and BMI did not have a statistically significant association (p=0.138) and that the AVCIMTs associations with the SBP, FBS, serum total cholesterol and LDL were found to be statistically significant (p<0.001).The correlation coefficient was however not very high and hence, the statistical analysis could not predict which among the traditional risk factors had a more predictive value. Nevertheless, the statistical significance implied that the Framingham’s traditional risk factors indeed had a role in contributing to CIMT.
Risk Factor profile among subjects
| Group | n | mean | Std deviation | t |
|---|
| BMI | Case | 100 | 24.0874 | 3.90531 | 4.87900 P=0.138 |
| Control | 100 | 21.9402 | 1.89417 |
| TC | Case | 100 | 226.0612 | 45.13983 | 17.33200 P<0.001vhs |
| Control | 100 | 137.6837 | 22.59304 |
| HDL-C | Case | 100 | 35.1512 | 9.17953 | 5.77800 P<0.001vhs |
| Control | 100 | 43.4914 | 10.95752 |
| LDL-C | Case | 100 | 168.7816 | 35.29315 | 30.10600 P<0.001vhs |
| control | 100 | 44.0745 | 20.87948 |
Relationship between AVCIMT and individual risk factors. AVCIMT had a negative correlation with HDL, with highest positive associations with Systolic blood pressure,FBS and LDL cholesterol
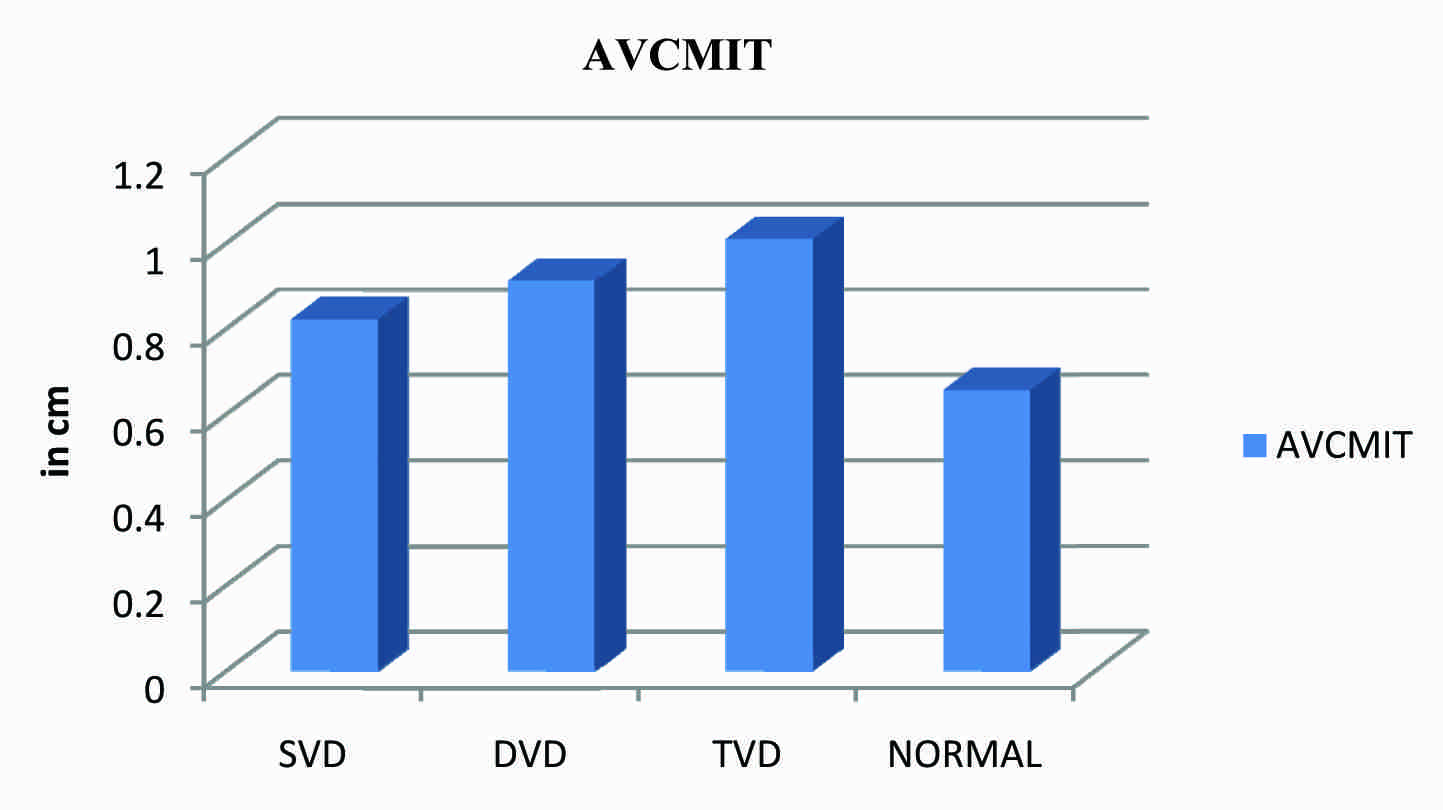
Further, as seen in [Table/Fig-5] the AVCIMT was found to be higher in triple vessel disease (1.00mm) <double vessel disease (0.91mm) <single vessel disease (0.82mm) <normal (0.65mm). Hence, a significant association between the extent of the carotid atherosclerosis and the presence of coronary artery disease was found.
Graph Showing Relationship Between Avcimt and Vessel Disease in Cases (p<.001) As the carotid intimal media thickness increased so did the extent of coronary artery disease in the study population AVCIMT was found to be higher in triple vessel disease (1.00mm) > double vessel disease (0.91mm) >single vessel disease (0.82mm) > normal coronaries (0.65mm)
DISCUSSION
The Carotid Intima Media Thickness (CIMT) is a valid marker of early atherosclerosis and thus, it has the potential to detect cardiovascular disease in its subclinical phase. The average CIMT was used in the analyses, as it has the advantage of stability and as it reflects the extent of the disease. Several studies have shown that the carotid IMT is strongly associated with the cardiovascular risk factors [14,15].
B-mode ultrasound has been proved to be a useful noninvasive means of quantitatively assessing the amount of atherosclerosis in the carotid arterial system [16]. The advantage of B-mode ultrasound lies in its ability to image the atherosclerosis within the arterial wall rather than that in the lumen of the artery. Its acceptance by medical researchers as a continuous measure of the localized atherosclerosis is reflected in its use in ongoing cohort studies and clinical trials [17,18].
The role of CIMT as an indicator of Coronary Artery Disease (CAD) has been assessed in various studies [18]. In the Atherosclerosis Risk In Communities study (ARIC) which included 13,870 sub-jects, the carotid IMT was found to be consistently greater in those with clinical cardiovascular disease than in the disease free controls [19].
Even in this study, we found a significant association between the extent of the carotid atherosclerosis which was measured by B-mode ultrasound and the presence (and its extent) or absence of the coronary atherosclerosis which was documented by coronary angiography. In the multivariate modelling which included an analysis between the risk factors (Hypertension , Diabetes Mellitus , smoking and Dyslipidaemia) and CIMT [20], although the correlation co efficient was not very high with respect to the risk factors and CIMT, it was found to be statistically significant (p<.001). Among the risk factors, the carotid intima-media thickness seemed to be a better predictor of the presence of coronary artery disease. We were able to analyse the morphology of the carotids among the 34 patients who had triple vessel disease. 12 were found to have plaques in their carotids, which reflected the severity of the atherosclerotic burden. Structural changes, especially plaques, are associated with a 4.15 fold risk of acute myocardial infarction, as was suggested by the work of Salonen et al., [10] Hence, B mode ultrasound of the carotids gives an added advantage to analyze, subsequently categorize and intervene at an early stage, in those who are at a greater risk of acute coronary events.
In a study which was done on 75 male patients who underwent coronary angiography for chest pain, Geroulakos and colleagues [20] showed that the common carotid IMT was not only higher in the patients with CAD, but that it also had a significant linear relationship with the number of involved arteries (r=0.54,p<0.001).
Visona and colleagues showed that the common carotid artery IMT in the CAD patients (1.45+/-0.95mm) was significantly higher than that in the controls (0.87+/-0.1mm;p<0.005) [21].
In this respect, the results of our study are in agreement with those of previous studies, which showed a significant association between the raised IMT and the presence of CAD.
A limitation of our study was that we could not document the CAD by angiography in the control population for ethical reasons. However, in view of the absence of risk factors or symptoms, CAD was presumptively excluded. Also, we could not derive a predictive cut off value of IMT for the detection of CAD. We could only show that the average CIMT was significantly higher in the affected population.
Although the normal CIMT values are being debated on in various studies, which have ranged from 0.7+/-0.1mm [17], our control population had a mean of 0.47+/-0.04mm,p<0.001.
CONCLUSION
We conclude through this study, that the easy applicability and the non invasive nature of B-mode ultrasonography make it suitable for use as a surrogate endpoint for measuring the atherosclerotic burden in people with cardiovascular risk factors. Its role in predicting the extent of CAD has already been established in the western population through various studies. This study suggests a significant association between the carotid IMT and the presence of CAD in the Indian population.
The average carotid intimal media thickness was higher in cases(0.90mm Vs 0.47mm)p<0.001( very highly significant)
[1]. Reddy KS, Yusuf S, Emerging epidemic of cardiovascular disease in developing countriesCirculation 1998 Feb 17 97(6):596-601. [Google Scholar]
[2]. Hansa G, Bhargava K, Bansal M, Tandon S, Kasliwal RR, Carotid intima-media thickness and coronary artery disease: an Indian PerspectiveAsian Cardiovasc Thorac Ann 2003 Sep 11(3):217-21. [Google Scholar]
[3]. Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R, Intimal plus media thickness of the arterial wall: a direct measurement with ultrasound imagingCirculation 1986 Dec 74(6):1399-406. [Google Scholar]
[4]. Folson AR, Eckiefeldt JH, Weitzman S, Ma J, Chambless LE, Barnes RW, Relation of carotid artery wall thickness to diabetes mellitus, fasting glucose and insulin, body size, and physical activity. Atherosclerosis Risk in Communities (ARIC) Study InvestigatorsStroke 1994 Jan 25(1):66-73. [Google Scholar]
[5]. Adams MR, Nakagomi A, Keech A, Robinson J, Mc Credie R, Bailey BB, Carotid intima-media thickness is only weakly correlated with the extent and severity of coronary artery diseaseCirculation 1995 Oct 15 92(8):2127-34. [Google Scholar]
[6]. Bots ML, Baldassarre D, Simon A, de Groot E, O’Leary DH, Riley W, Carotid intima-media thickness and coronary atherosclerosis: weak or strong relations?Eur Heart J. 2007 Feb 28(4):398-406. [Google Scholar]
[7]. Lekakis JP, Papamichael CM, Cimponeriu AT, Stamatelopoulos KS, Papaioannou TG, Kanakakis J, Atherosclerotic changes of extracoronary arteries are associated with the extent of coronary atherosclerosisAm J Cardiol 2000 Apr 15 85(8):949-52. [Google Scholar]
[8]. Simon A, Chironi G, The relationship between carotid intima media thickness and coronary atherosclerosis revisitedEur Heart J 2007 Sep 28(17):2049-50. [Google Scholar]
[9]. Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu CR, Liu CH, The role of carotid arterial intimal-media thickness in predicting clinical coronary eventsAnn Intern Med 1998 Feb 15 128(4):262-69. [Google Scholar]
[10]. Salonen R, Salonen JT, Progression of carotid atherosclerosis and its determinants: a population-based ultrasonography studyAtherosclerosis 1990 Feb 81(1):33-40. [Google Scholar]
[11]. Handa N, Matsumoto M, Maeda H, Hougaka H, Ogawa S, Fukunaga R, Ultrasonic evaluation of early carotid atherosclerosisStroke 1990 Nov 21(11):1567-72. [Google Scholar]
[12]. O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr, Carotid artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults: Cardiovascular Health Study Collaborative Research GroupN Engl J Med 1999 Jan 7 340(1):14-22. [Google Scholar]
[13]. Peter Libby, The Pathogenesis of Atherosclerosis“Harrison’s Principles of Internal Medicine”Vol II16th editionNew YorkMcGraw Hill Health Professional Division Publication:1425-30. [Google Scholar]
[14]. Gomez-Marcos MA, Recio-Rodríguez JI, Patino-Alonso MC, Agudo-Conde C, Gomez-Sanchez L, Gomez-Sanchez M, Protocol for Measuring Carotid Intima-Media Thickness That Best Correlates With Cardiovascular Risk and Target Organ DamageAm J Hypertens 2012 Jun 21 [Google Scholar]
[15]. Kanters SD, Algra A, van Leeuwen MS, Banga JD, Reproducibility of in-vivo carotid intima-media thickness measurement: A reviewStroke 1997 Mar 28(3):665-71. [Google Scholar]
[16]. Mohan V, Ravikumar R, Shanthi Rani S, Deepa R, Intima medial thickness of the carotid artery in south Indian diabetic and non diabetic subjects: the Chennai Urban Population Study (CUPS)Diabetologia 2000 Apr 43(4):494-99. [Google Scholar]
[17]. O’Leary DH, Polak JF, Intima Media Thickness. A Tool for Atherosclerosis imaging and Event PredictionAm J Cardiol 2002 Nov 21 90(10C):18L-21L. [Google Scholar]
[18]. Robertson CM, Fowkes FG, Price JF, Carotid intima-media thickness and the prediction of vascular eventsVasc Med 2012 Jun 13 [Google Scholar]
[19]. Heiss G, Sharrett AR, Barnes R, Chambless LE, Szklo M, Alzola C, Carotid atherosclerosis measured by B-mode ultrasound in populations: associations with cardiovascular risk factors in the ARIC studyAm J Epidemiol 1991 Aug 1 134(3):250-56. [Google Scholar]
[20]. Geroulakos G, O’Gorman DJ, Kalodiki E, Sheridan DJ, Nicolaides AN, The carotid intima-media thickness as a marker of the presence of severe symptomatic coronary artery diseaseEur Heart J 1994 Jun 15(6):781-85. [Google Scholar]
[21]. Visona A, Pesavento R, Lusiani L, Bonanome A, Cernetti C, Rossi M, Intimal medial thickening of the common carotid artery as an indicator of coronary artery diseaseAngiology 1996 Jan 47(1):61-66. [Google Scholar]