The Aesthetic Management of a 180 Degree Rotated Maxillary Central Incisor With Two Root Canals- A Case Report
Shweta Jain1, Praful Narang2, Rohit Sharma3, Vijay Agarwal4
1 Reader, Department of Conservative Dentistry & Endodontics, NIMS Dental College & Hospital, Jaipur, Rajasthan, India.
2 Assistant Professor, Department of Prosthodontics, NIMS Dental College & Hospital, Jaipur, Rajasthan, India.
3 Assistant Professor, Department of Oral Medicine & Radiology, NIMS Dental College & Hospital, Jaipur, Rajasthan, India.
4 Reader, Department of Orthodontics, NIMS Dental College & Hospital, Jaipur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shweta Jain, 148, Gurunanakpura, Adarsh Nagar, Jaipur, India.
Phone: 09982000741, 0141-2621989
E-mail: vshwetamds@rediffmail.com
The success of the root canal treatment is based on a thorough knowledge of the normal tooth, the root and the root canal morphology, which include variations. Tooth rotation is a common finding in the premolar-molar region, but a 180 degree rotation of the maxillary central incisor is extremely rare and it has not documented anywhere in the dental literature. This case report describes the aesthetic correction of a maxillary central incisor with a 180 degree rotation and two root canals.
Maxillary central incisor, 180 degree rotation, Root canal
INTRODUCTION
A minor-to-pronounced axial rotation has been noted of individual teeth, which is caused by crowding in the arch, retained primary teeth, cleft lip/palate, heredity, supernumerary teeth or odontomes and an ectopic canine or due to trauma in the deciduous dentition [1]. Winging and counter-winging, either unilateral or bilateral, of the maxillary central incisors, which is seen predominantly in the native American Indians, is one example of a minor rotation of a tooth [2]. A more pronounced axial rotation of an individual tooth typically involves 90 to 180 degree rotations. There are only very few case reports on the 180 degree rotations of the maxillary second premolars [3], but 180 degree rotations of the maxillary central incisors have not been reported.
However, evidences of three or four canals and two or more roots in the maxillary central incisor are there [4]. These generally present with a single root and a 98% incidence of a single canal and only a 2% incidence of two canals [5]. This report illustrates a case of a maxillary central incisor with a 180 degree rotated crown with two root canals, that required an aesthetic correction and was managed by a multi-disciplinary approach.
CASE HISTORY
A 23 years old male with a non contributory medical history came to the dental office for an aesthetic make over of one, unusual appearing, upper front tooth [Table/Fig-1a]. The clinical examination revealed a left maxillary central incisor with an anatomical labial crown surface which was placed palatally and vice versa [Table/Fig-1b, c]. The patient had no history of trauma. The pulp sensibility test which was done with an electric pulp tester (Parker Electronics Division, Farmingdale, NY, USA) gave a positive response. The tooth was not mobile and a periodontal probing which was done around the tooth was within physiological limits. The preoperative diagnostic radiograph revealed a large radiolucency of the root canal space, upto the junction of the middle and the apical third of the root, which suddenly disappeared in the apical third [Table/Fig-1d]. This finding strongly indicated the presence of a bifurcation of the root canal. All the treatment options which included an orthodontic correction and a prosthodontic rehabilitation of the affected tooth were explained to the patient. As the patient needed an immediate aesthetic management, a prosthodontic rehabilitation of the left maxillary incisor was planned. Due to a labial inclination, the chances of the pulp exposure were very high during the tooth preparation. So, an intentional root canal treatment was advised.
Esthetic treatment of 180 degree rotated maxillary central incisor with two root canals
(a) Preoperative extraoral presentation of maxillary incisors
(b) labial view palatal view of left maxillary central incisors showing 180 degree rotation (c) palatal view (d) Preoperative radiograph (e) working length determination (f) Postoperative radiograph (g) Follow-up radiograph (h) Clinical presentation after prosthetic rehabilitation
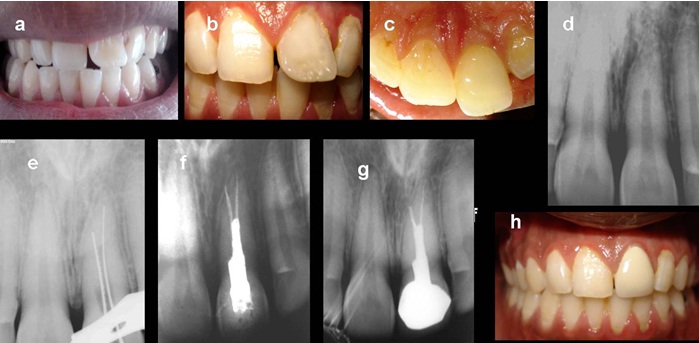
Following local anaesthesia with 2% lignocaine which contained 1:200,000 epinephrine (Xylocaine: Astra Zeneca Pharma Ltd, Banglore, India), an access cavity was prepared under a rubber dam isolation. Two canals were negotiated and the working lengths were determined [Table/Fig-1e].
Cleaning and shaping of the root canal was done. The canals were dried with absorbent points and they were obturated by a combined thermomechanical gutta percha obturation technique (E and Q Plus, Meta, Biomed) with an AH plus sealer (Dentsply Tulsa) [Table/Fig-1f]. The access cavity was sealed with composite resin. Later on, a full coverage metal-ceramic crown was given for the aesthetic correction [Table/Fig-1g, h].
DISCUSSION
This case is being reported because of two unusual aspects, one, the 180 degree rotation and the second, the presence of two root canals in a single root. The aetiology of the rotation could not be identified, as the patient did not have any orofacial deformities which are the possible aetiological factors for the presence of rotated tooth [6]. The clinical examinations of his parents and sibling did not reveal any malformed teeth.
The rotation of teeth is very common in the premolar molar region and it is frequently corrected by using an orthodontic intervention. Once they erupt into this crowded state, the fibres that secure the teeth in position, develop and increase their resistance to change orthodontically, as well as they increase their tendency to relapse or to return to their original positions once they are straightened. As rotations are easy to treat but very difficult to retain, the treatment of the affected teeth are advised in the pre-adolescent ages. In our case, a circumferential supracrestal fibrotomy was advised next to an overcorrection of the tooth, followed by a fixed retention [7]. A surgical derotation or an intentional derotation can be used for the treatment of rotated tooth, but an ideal case selection is important to achieve the desired results.
This maxillary central incisor represented the Weine’s Type IV canal and the Vertucci’s Type V canal configurations. A surgical microscope and magnifying loops are very helpful in locating additional root canals. When radiographic images are interpreted, it is important to recognize the imaging artifacts to make an accurate diagnosis. These too should be supplemented by clinical pictures. A new CT (Computed Tomography) technique, SCT (Spiral Computed Tomography) or volume acquisition CT, has been developed and it has been used successfully in clinical dentistry for the confirmatory diagnosis of morphologic aberrations in the root canal anatomy, and it might provide a better, more accurate, and a faster diagnostic method in all the 3 dimensions [8]. CBCT (Cone Beam Computed Tomography) is advantageous as it has a low effective dose in the same order of the magnitude as the conventional dental radiographs [9].
[1]. Winzar CF, Rotated anterior teethAustralian Dental Journal 1967 12:417-20. [Google Scholar]
[2]. Dahlberg AA, Analysis of the American Indian dentition. In: Brothwell DR, ed.Dental Anthropology 1963 New York, NYPergamon:149-77. [Google Scholar]
[3]. Stefan VH, Brief Communication: Rotation of the Maxillary Premolars: Evidence in Support of Premolar Morphogenetic FieldDental Antropology 2006 19:70-73. [Google Scholar]
[4]. Gondim E, Setzer F, Zingg P, Karabucak B, A Maxillary Central Incisor with Three Root Canals: A Case ReportJ Endod 2009 35:1445-47. [Google Scholar]
[5]. Sert S, Bayrili GS, Evaluation of the root canal configurations of the maxillary and mandibular permanent teeth by gender in the Turkish populationJ Endod 2004 30:391 [Google Scholar]
[6]. Scott GR, Potter RHY, Noss JF, Dahlberg AA, Dahlberg T, The dental morphology of Pima IndiansAm J Phys Anthropol 1983 61(1):13-31. [Google Scholar]
[7]. Jahanbin A, Baghaii B, Parisay I, Correction of a severely rotated maxillary central incisor with the Whip deviceThe Saudi Dental Journal 2010 22:41-44. [Google Scholar]
[8]. Hu H, He HD, Foley WD, Fox SH, Four multidetector-row helical CT: image quality and volume coverage speedRadiology 2000 215:55-62. [Google Scholar]
[9]. Patel S, Dawood A, Pitt Ford T, Whaites E, The potential applications of cone beam computed tomography in the management of endodontic problemsInternational Endodontic Journal 2007 40:818-30. [Google Scholar]