Animal related injuries are frequently reported in India and other countries, where bulls are used for sporting events as well as in places where farming and livestock rearing is practised. The presentation is, many times, atypical and misleading as well.
They have unique mechanics of injury. The patterns of the injury are reviewed. An intra-peritoneal urinary bladder injury which is caused by a perineal bull gore with a pneumoperitoneum is unusual and it has not been reported in the literature which was reviewed. We are reporting a successfully treated 25 years old male patient from the slopes of the southern district of Manipur, India, who had presented 40 hours after he was injured. The identification and prompt exploration, keeping in mind the mechanics of bull goring, helps the surgeons to adequately deal such atypical injuries, for optimal outcomes.
Bull gore, Perineum, Urinary bladder perforation, Pneumoperitoneum, India
INTRODUCTION
Animal related injuries are frequently reported in countries where bulls are used for sporting events as well as in places where farming and livestock rearing is practised [1, 2]. In India, it is commonly seen in the “Jallikattu” event of taming bulls, which is organized as a part of Pongal - a festival of the harvest season which is celebrated across Tamil Nadu, India. Injuries, minor to fatal, are caused by bull gores. An intra-peritoneal urinary bladder injury which was caused by a perineal bull gore has not been reported in the available literature. One of the oldest reports which had described a bladder injury had come from Baron Jean Dominique Larry, who was a military surgeon to Napoleon Bonaparte, who had witnessed a drunken soldier trying his hand as a matador and entering the bull-ring. He was gored. Larry took him to the hospital, explored the wound, decompressed his bladder with a gum elastic catheter, and reduced the herniated bladder mucosa through the torn muscles of the groin. He was found to be cured six months later [3].
The mechanics of bull goring are unique and often misleading and thence, they deserve reporting. We are reporting an unusual case with a bull gore injury to the perineum, who presented with a pneumoperitoneum and urinary bladder perforation.
CASE SUMMARY
A 25 year old male patient from the slopes of the southern district of Manipur, presented 40 hours after receiving a bull horn injury to the perineum. There was a history of extravasation of blood mixed urine through the perineal wound and the anus. At presentation, his vitals were found to be stable but he had signs of peritonitis and mild abdominal distention. He had a penetrating wound which was 3x1cms lateral to the anal orifice, on the right side [Table/Fig-1], which was large enough to be digitally explored under local anaesthesia, with minimal patient discomfort. There was an abrasion on his buttocks, of nearly 10 cm, which tapered into it. A digital rectal examination and proctoscopy neither revealed any urine leak nor any sign of a rectal injury; there was no loss of the sphincter tone. A per urethral Foley’s catheter which was inserted without difficulty, drained haematuria. A pneumoperitoneum was evident radiographically and there was no fracture of the pelvis. His haemoglobin was 10.8g/dl. The patient was resuscitated. Broad spectrum antibiotics and Tetanus immunoglobulins were administered.
The 3cm perineal entry wound lateral to anal orifice on right side just sparing the anal sphincters at 2 weeks of healing

Operative Findings
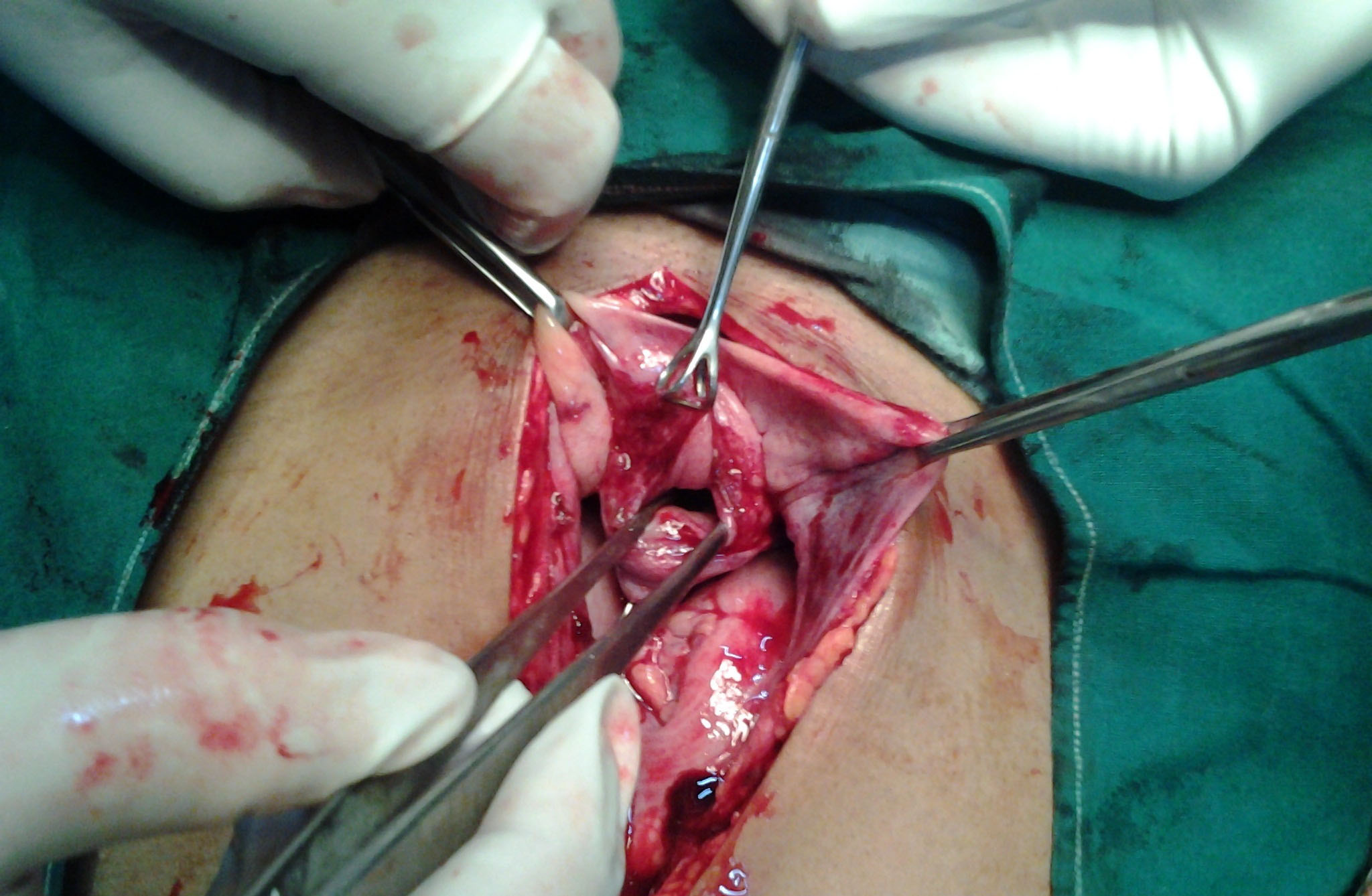
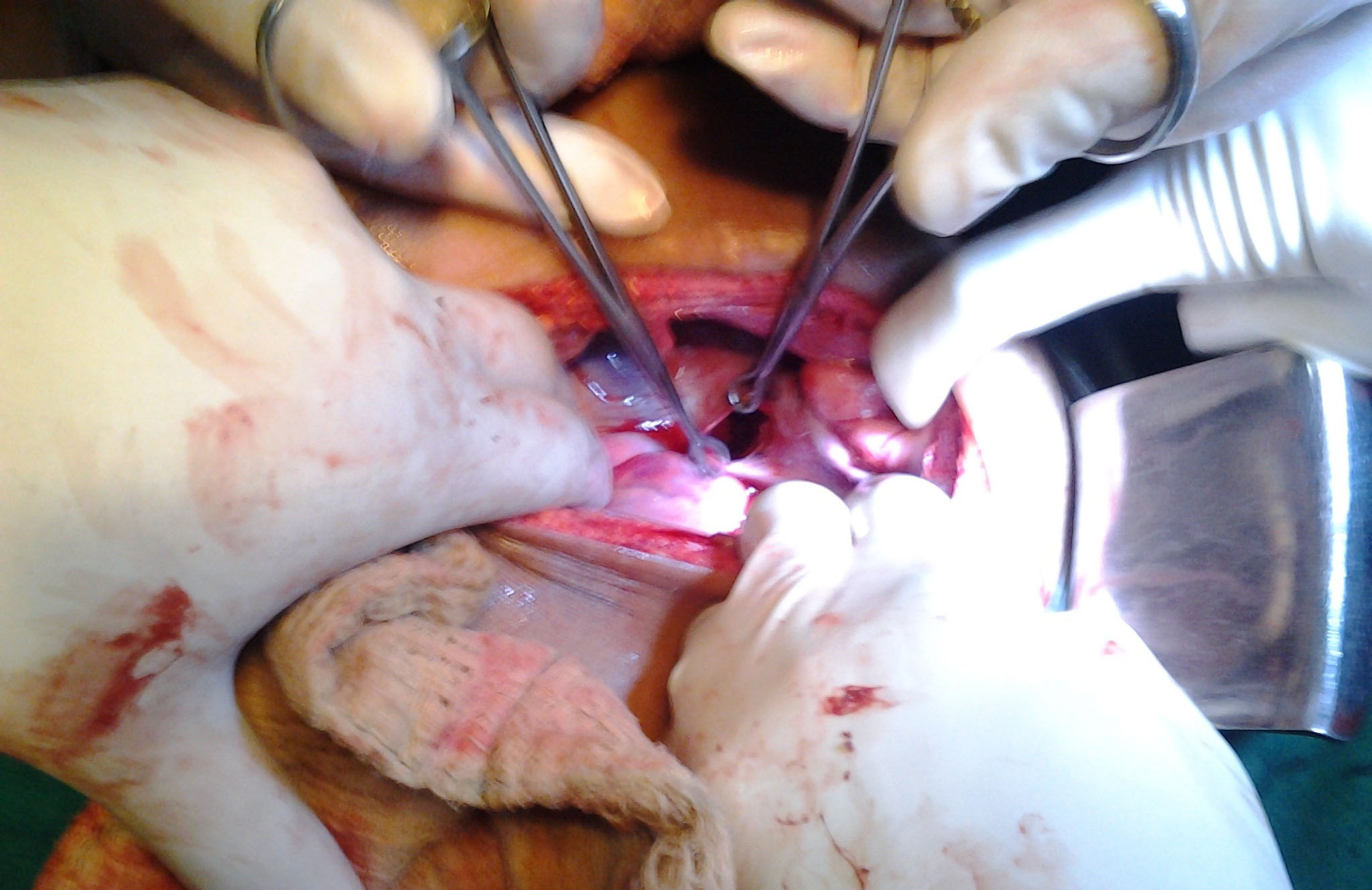
After resuscitation, abdomen was explored through a infraumbilical midline incision. There was a peritoneal contamination with urine but not faecal matter. A perforation in the dome of the bladder [Table/Fig-2] and a breach in its peritoneum [Table/Fig-3] were noticed. The urinary bladder exploration revealed a laceration of around 2 cm in the right lateral wall of the extraperitoneal bladder, through which a finger could reach the bladder. The urinary bladder was repaired with Vicryl 2-0 in two layers. A Supra Pubic Cystotomy (SPC) was done by using a Malecots catheter. An exploration through the peritoneal rent failed to reveal any breach in the rectal wall. A loop transverse colostomy was done and the abdomen was closed. The perineal wound was cleaned with hydrogen peroxide and it was packed. Post-operatively, the urine was drained through both SPC and per urethral catheters.
Intra-Operative photograph showing perforation of urinary bladder intraperitionally at its dome
Intra-Operative photograph showing the rent in posterior peritoneum
The patient was started on oral feeds on the 3rd post-operative day. Dressing of the perineal wound was done regularly. There was haematuria, which subsided by two weeks. At the end of three weeks, the Foley’s catheter was removed, and a micturating cystourethrogram which was done, was found to be normal. The next day, the SPC was clamped and the patient passed urine per urethra comfortably. Hence, the SPC was removed. By then, the perineal wound had healed completely. The patient was discharged and the colostomy closure was done at a later date.
DISCUSSION
The ox, cow and buffalo are docile as compared to the bull, which can easily become raged. Injuries may be sustained from the horns of these animals, either accidentally or as a result of an attack, more so, when they become raged, as in sports shows. The pattern of injury at different places, seems to vary. In India, perineal followed by abdominal injuries predominate in contradistinction to those in the Latin countries, where lower extremity injuries are more common. It is summarized in the [Table/Fig-4] [1, 4–9].
Pattern of bull gore injuries
| Place | Most common injuries | Other injuries |
|---|
| India [4] | Perineum and Genitalia (36.6%) | Abdomen (24.8%), head and neck (15.8%), thorax (13.9%), extremities (9.8%) |
| Turkey [1] | Abdomen (60.9%) | Chest (39.1%) |
| Fulani [6] | Abdomen (50%) | Scrotum (18.9%), neck (9.3%), other sites (22.8%) |
| Latin countries [7,8,9] | Lower extremity (>50%) | Perineum (7-10.5%) |
Apparently abdominoperineal injuries are common in the Indian rural setup. The perineum is considered to be a highly protected region due to the reflex adduction of the thighs [8]. However, severe lesions with high mortality rates which are caused by bleeding, have been observed [4]. Our patient did not have any major vascular injury, luckily. A perineal bleeding in trauma is notoriously difficult at times, to control by packing alone. The surgeon may ligate the internal iliac artery as a last resort in such circumstances (Personal data-unpublished). Bull gores to the perineum cause vulvovaginal, anorectal, rectovaginal, urethrorectal injuries and foetal death which may require medical termination of pregnancies, have been described in the literature. Bladder neck ruptures and prostatic urethra injuries with pelvic fractures are also reported [9–12]. A through and through bladder perforation, sparing the sphincters and urethra, with a pneumoperitoneum, is very unusual. The presentations of urinary peritonitis are diverse, with hidden and misleading symptoms which can delay the diagnosis long enough to endanger the patient’s life. Dramatic presentations like shock may be absent unless they are complicated by urinary sepsis, pelvic fractures, or visceral bleeding [13].
The mechanisms of bull gore injuries are interestingly unique and they have been well reviewed by Mark Sheldon [7]. The bulls gore the offender through an upward and a lateral angulation, with the path of penetration following an arc. The tearing injuries are attributed to the strong neck muscles of the animal. The patient’s entire body weight may be lifted up. The severity of the injuries and the depth of penetration depend on the momentum and the patient’s height, along with his/her position. When the animal tries to disengage its horn, the patient’s weight additionally acting in the opposite direction predisposes to repeat penetration, and possibly multiple tracks. Multiple entry wounds have also been reported [9]. The rotational or semicircular movements make the deep injuries rare, as the skin of the abdomen and the perineum are tangential to the arc of the gore. The horn will many times traverse in a plane between the skin and the abdominal wall muscles of the victims and this has been well documented.
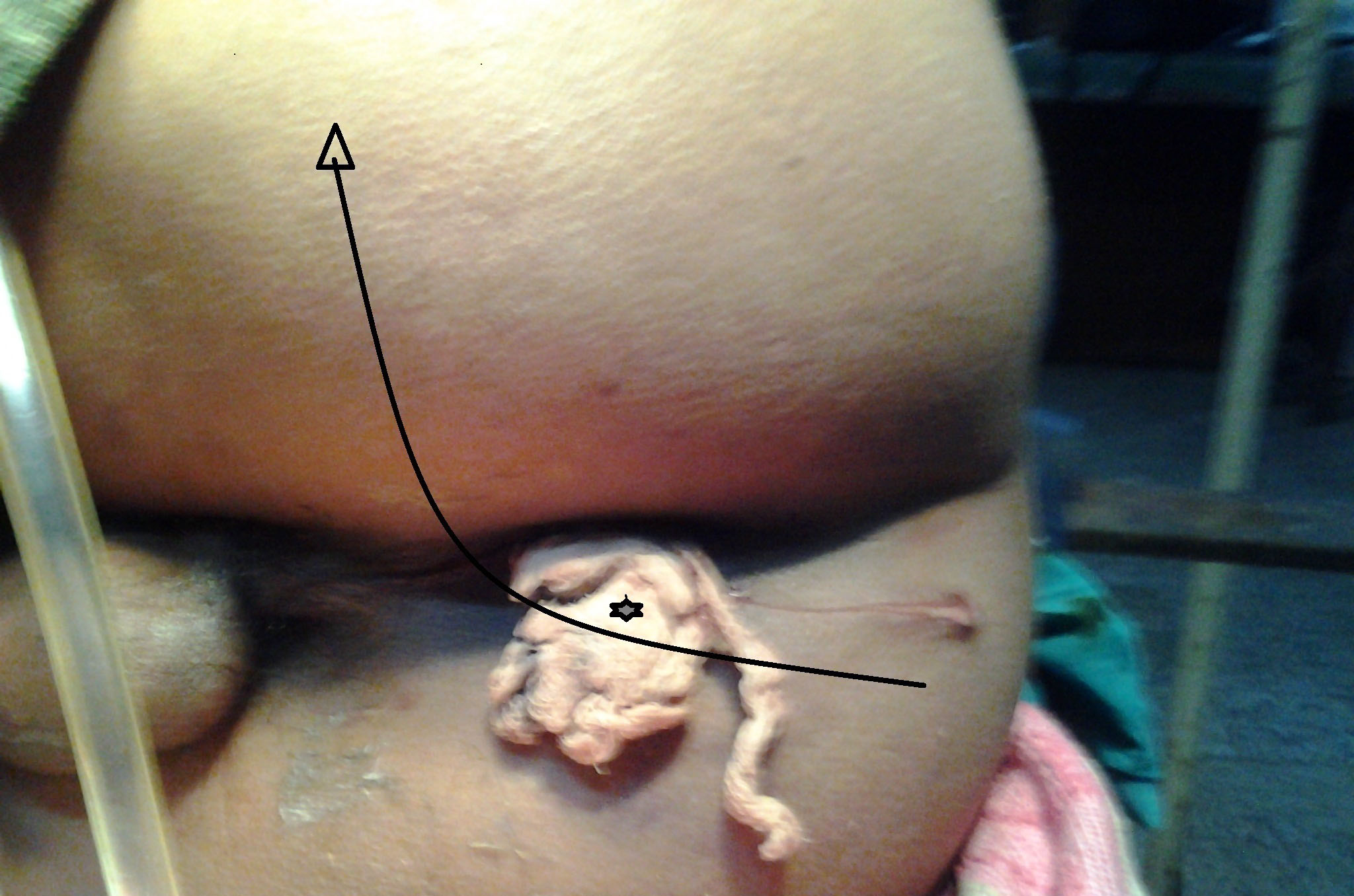
A proper history which elicits the mode of injury and the position of the patient should be sought from the patient himself/herself or from an eyewitness, if it is available. An abrasion in the perineum [Table/Fig-5] may guide the direction of the tract and the possible organ which may be injured. The entry wound may be misguidingly smaller; all the wounds should be explored under anaesthesia, either local or general and they should be cleaned with hydrogen peroxide and debrided. Anti-tetanus globulins should be instituted, as Clostridium welchi and C. tetani spores may complicate the horn gores due to their frequent contamination with dung [2] The antibiotics should include penicillins, metronidazole and aminoglycosides to cover gram positive, gram negative and anaerobic bacteria and other microbial organisms [2].
Photograph showing the abrasion due to bull gore, a tell-tale sign of possible path of penetration. The arc of goring is depicted. The entry wound (marked by asterisk) was plugged at presentation
The patient was directly taken to the operating room for exploration, as there was an obvious bladder injury, and an anticipated bowel injury and contamination. But, whenever in doubt, a retrograde urethro-cystography (RGU) which is considered as the gold standard for the identification of bladder and urethral ruptures, should be done [14]. The extraperitoneal bladder can be repaired in layers from within, through the rent. Many studies have supported the Foley’s catheter drainage as the sole treatment in extraperitoneal bladder injuries, where a majority of them heal within 3 weeks [14]. This was true, even with vesico-cutaneous fistulas. The grave nature of the infections including gas gangrene which could interfere with the bladder healing prompted us to have an SPC insitu for prolonged drainage. SPCs have a low rate of infection, urethral complications and better patient compliance for a long term drainage, as compared to per-urethral catheters.
Though no clear cut guidelines exist, a diversion colostomy helps in a better wound management in patients with perineal wounds, after trauma or burns is suggested. We had a low threshold to consider a colostomy in our case, as there was a rent in the peritoneum and an associated pneumoperitoneum. A proximal transverse loop colostomy was done, as the sigmoid colon was less mobile. This helped the perineal wound to heal faster without any secondary faecal sepsis. A special rectal catheter to divert the faeces, has also been described in the literature, which can be used as an alternative to avoid the morbidity which is associated with the stoma, when expertise is available [15]. Whether a through and through bladder perforation can cause a pneumoperitoneum or whether the rectal perforation cannot be visualized intra-operatively (possibly because of tissue resilience or an oedema which closed a small rectal perforation), is a matter of debate. But since there was neither a breach in the rectal wall nor was there any faecal contamination in the peritoneal cavity, we attributed the pneumoperitoneum to a bladder perforation. Whatsoever, the adherence to the basic principles of surgery helped the patient to go back home to celebrate Christmas.
CONCLUSION
Bull gore injuries to the perineum which perforate the bladder intraperitoneally, sparing the anal sphincter or the urethra, are unusual and rare. An identification and a prompt exploration, keeping in mind the mechanics and the nature of bull gores, helps the surgeon to adequately deal such atypical injuries, for optimal outcomes.
[1]. Dogan KH, Sunam GS, Erkol Z, Serafettin D, Zerrin E, Guven SS, Injuries and Deaths Occurring as a Result of Bull AttackJournal of Agromedicine 2008 13(3):191-96. [Google Scholar]
[2]. Martinez-Ramos D, Miralles-Tena JM, Escrig-Sos J, Traver-Martinez G, Cisneros-Reig I, Salvador-Sanchis JL, Bull horn wounds in Castellon General Hospital. A study of 387 patients. (In Spanish.)Cir Esp 2006 80:16-22. [Google Scholar]
[3]. Crumplin MK, Matador versus Taurus: bull gore injuryAnn R Coll Surg Engl 2004 86(5):402doi 10.1308/147870804821. PMID: 15333186 [Google Scholar]
[4]. Idikula J, Moses BV, Sadhu D, Agarwal S, Jahan G, Thomas J, Bull horn injuriesSurg Gynecol Obstet 1991 172:220-22. [Google Scholar]
[5]. Shukla HS, Mittal DK, Naithani YP, Bull horn injury: a clinical studyInjury 1977 9:164-67. [Google Scholar]
[6]. Sabo SY, Yusufo LMD, Injuries from cow gore in adults among FulaniTrop Doct 2007 Apr 37(2):111-12. [Google Scholar]
[7]. Lloyd MS, Matador versus taurus: bull gore injuryAnn R Coll Surg Engl 2004 86:3-5. [Google Scholar]
[8]. Rudloff U, Gonzalez V, Fernandez E, Holguin E, Rubio G, Lomelin J, Dittmar M, Barrera R, Chirurgica Taurina: a 10-year experience of bullfight injuriesJ Trauma 2006 Oct 61(4):970-74. [Google Scholar]
[9]. Padilla Fernandez B, Diaz Alferez FJ, Garcia MA, Herrero Polo M, Velasquez Saldarriaga JF, Lorenzo Gomez MF, Bladder Neck Rupture Following Perineal Bull Horn Injury: A Surgical ChallengeClin Med Insights Case Rep 2012 5:123-28. [Google Scholar]
[10]. Singhal VP, Neelam Ankur H K, Kaur P, Katiyar N, Traumatic massive vulval haematomasInternational Journal of Gynae Plastic Surgery 2010 2:35-37. [Google Scholar]
[11]. Kulkarni MG, Mahendra G, Kulkarni SR, Bull Gore Injury of the VaginaJ Clin Diagn Res 2012 Nov ID: JCDR/2012/4959:2580 [Google Scholar]
[12]. Wasadikar PP, Paunikar RG, Deshmukh SB, Bull horn injuries, in rural IndiaJ. Indian Med Assoc 1997 19(1):3-4. [Google Scholar]
[13]. Dubey IB, Mohanty D, Jain BK, Diverse presentation of spontaneous rupture of urinary bladder: review of two cases and literatureAm J Emerg Med 2012 Jun 30(5):832 [Google Scholar]
[14]. Kotkin L, Koch MO, Morbidity associated with nonoperative management of extraperitoneal bladder injuriesJ Trauma 1995 Jun 38(6):895-98. [Google Scholar]
[15]. Sharma RK, Parashar A, The management of perineal woundsIndian J Plast Surg 2012 May 45(2):352-63.doi: 10.4103/09700358.101318 [Google Scholar]