An Impacted Denture in the Oesophagus-An Endoscopic or A Surgical Emergency-A Case Report
Parvinder Singh1, Amritpal Singh2, Puneet Kant3, B. Zonunsanga4, Amarjit Singh Kuka5
1 Assistant Professor (Surgical Gastroenterology), Department of General Surgery,
2 Assistant Professor, Department of General Surgery,
3 Junior Resident, Department of General Surgery,
4 Junior Resident, Department of General Surgery,
5 Associate Professor, Department of General Surgery, Guru Gobind Singh Medical College & Hospital, Sadiq Road, Faridkot-151 203, Punjab, India.
NAME, ADRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Parvinder Singh, Assistant Professor (Surgical Gastroenterology), Department of General Surgery, 81, Medical Campus, Sadiq Road, Faridkot-151 203, Punjab, India.
Phone: 09988099532
E-mail: drperrysingh@yahoo.com
Accidentally swallowed dentures can lead to severe complications in the gastrointestinal tract. Therefore, an early detection and an effective therapeutic management are important. In the era of advanced endoscopy, though the primary treatment of an impacted foreign body in the oesophagus is an endoscopic removal, a primary surgical treatment is advised for dentures with sharp hooks. Also, a prolonged impaction of dentures with sharp hooks leads to an increase in the complication rates. We are reporting a case of accidentally swallowed denture. After the diagnosis of an impacted denture was made, upper GI endoscopy revealed that an endoscopic removal was not feasible and thus, a late surgical removal was performed in the form of a transhiatal oesophagectomy and reconstruction. This case highlights the importance of an early and preferred treatment in the form of a controlled surgical intervention as compared to an endoscopic extraction for patients with impacted dentures with sharp hooks.
Impacted foreign body in the oesophagus, Impacted denture, Denture with sharp hooks, Oesophagectomy
INTRODUCTION
Impacted foreign bodies in the oesophagus are common both in adults as well as in children. In children, coins, pieces of toys, etc. are the commonly seen foreign bodies, while in adults, orthodontic appliances are the most common cause of an accidental swallowing. An accidental ingestion of an appliance can create a medical or a surgical emergency that can lead to serious complications, including death from aspiration of the foreign body [1]. Because of their sizes, rigidity and pointed edges; dentures get frequently impacted in the oesophagus and are difficult to retrieve endoscopically [2].
CASE REPORT
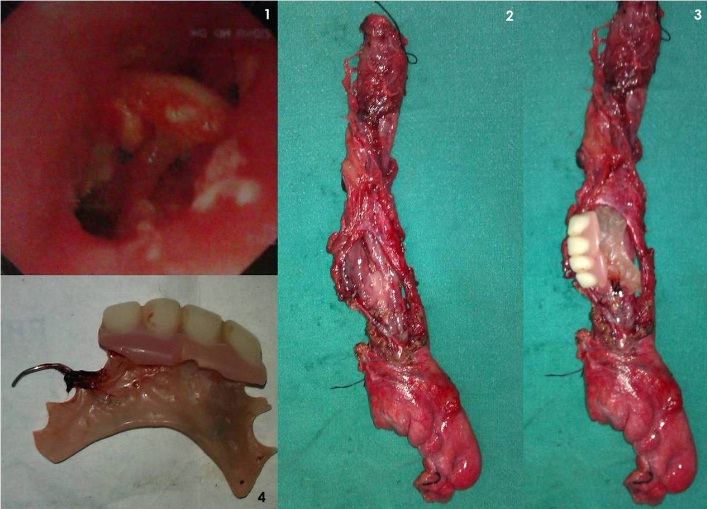
A 40 years old male patient, a labourer by occupation, reported to the emergency department of our hospital with the complaint of accidental swallowing of the upper denture, around 5 days back. On questioning, he couldn’t tell the shape of the swallowed denture. He had fever (100o F) with raised total leucocyte counts (14000), without any respiratory distress. He had no history of a significant dysphagia. He also had a history of get this denture removed endoscopically around 4 days back but could not be successful. On examining the endoscopic report, he was found to have an impacted denture at 40 cm from the incisor tooth [Table/Fig-1]. As the patient was very poor, a CECT scan was not performed. A plain X-ray of the chest didn’t reveal any evidence of any pleural effusion or any pneumomediastinum. Keeping in view, the impacted denture at the lower end of the oesophagus, a laparotomy was planned, with removal of the denture. On laparotomy, it was found that there was inflammation at the GE junction and that the denture was impacted in the lower oesophagus instead of the GE junction, which was removed (which consisted of four teeth along with the jaw plate and the hook) after an oesophagotomy was made in the anterior wall of the lower one third of the oesophagus. Around 7-8 cm of the posterior and the lateral walls of the lower oesophagus were necrotic because of the impaction of the sharp hooks as well as the denture. As such, there was no periesophageal soilage. Keeping in view, the large extent of the oesophageal involvement, a transhiatal oesophagectomy was planned, which was done successfully. Post op, he had a leakage from the neck anastomosis, which got healed in 2 weeks. At follow up after 3 months, he was doing well.
1. Endoscopic view showing impacted denture at lower end of oesophagus
2. Excised esophagus specimen showing necrotic walls of oesophagus
3. Position of denture in the oesophagus
4. Removed denture with sharp hooks
DISCUSSION
Though coins are the commonest foreign bodies which are seen in the oesophagus in children, dentures are common in aged people due to the decreased sensation of the oral cavity in denture wearers and the poor motor control of the laryngopharynx [3]. Following foreign body ingestion, the patients usually present with dysphagia (92%). The other symptoms include hypersalivation, retroster nal fullness, regurgitation of undigested food, and odynophagia. Sometimes, the patient can be asymptomatic in the early period of ingestion of the foreign body, which can lead to a voluntary or an involuntary delay in the presentation, as it happened in our case. A radiological imaging can determine the exact site of the radioopaque impacted foreign body. Dentures, however, are frequently made of acrylic resin, which is a radiolucent material and thus, they are difficult to assess on plain X-Rays, though the radio-opaque wire hooks of the dentures can sometimes be seen, if they are present [1,4]. Most of the swallowed foreign bodies are impacted at the cervical and the upper oesophagus. The small dentures without hooks usually travel through the alimentary tract to the anus. A prolonged impaction of the dentures with sharp hooks in the oesophagus can cause peri-oesophagitis, necrosis and perforation of the wall or a fistula formation. It has been reported that more than 24 hours after the ingestion, the rate of complications multiplies from 3.2% at 24 hours to as high as 23.5% after 48 hours [4]. Thus, there is no room for an expectant or a conservative management in the cases of impacted dentures, as the risk of the complications increase, the longer it takes before an appropriate intervention. Few reports have described the usefulness of an endoscopic removal, even for sharp or penetrating foreign bodies [5–7]. However, the sharp hooks of the dentures are likely to damage the oesophageal or the pharyngeal wall [3]. Consequently, it is difficult to remove the dentures endoscopically. Many articles have supported this primarily surgical approach over an endoscopic removal for sharp dentures [2–4], [8–9].
CONCLUSION
The experience of this present case illustrates that the prompt management of an impacted denture in the oesophagus is preferably surgical rather than endoscopic. Also, if the patient does not have dysphagia, even than, the patient should be investigated thoroughly with respect to the position of the denture and its associated complications and it should be treated as early as possible, so that any catastrophe can be prevented.
[1]. Rohida Neeraj S, Bhad Wasundhara A, Accidental ingestion of a fractured Twin-block applianceAm J Orthod Dentofacial Orthop 2011 139:123-25. [Google Scholar]
[2]. Dalvi AN, Thapar VK, Jagtap S, Barve DJ, Savarkar DP, Garle MN, Thoracoscopic removal of impacted denture: Report of a case with review of literatureJ Min Access Surg 2010 Oct-Dec 6:119-21. [Google Scholar]
[3]. Toshima T, Morita M, Sadanaga N, Yoshida R, Yoshinaga K, Saeki H, Surgical Removal of a Denture with Sharp Clasps Impacted in the Cervicothoracic Esophagus: Report of Three CasesSurg Today 2011 41:1275-79. [Google Scholar]
[4]. Chua YKD, See JY, Ti TK, Oesophageal-impacted denture requiring open surgerySingapore Med J 2006 47(9):820-21. [Google Scholar]
[5]. Rathore PK, Raj A, Sayal A, Meher R, Gupta B, Girhotra M, Prolonged foreign body impaction in the oesophagusSingapore Med J 2009 50(2):e53-54. [Google Scholar]
[6]. Weissberg D, Refaely Y, Foreign bodies in the esophagusAnn Thorac Surg 2007 84:1854-57. [Google Scholar]
[7]. Athanassiadi K, Gerazounis M, Metaxas E, Kalantzi N, Management of esophageal foreign bodies: A retrospective review of 400 casesEur J Cardiothorac Surg 2002 21:653-56. [Google Scholar]
[8]. Stiles BM, Wilson WH, Bridges MA, Choudhury A, Rivera-Arias J, Nguyen DB, Denture esophageal impaction refractory to endoscopic removal in a psychiatric patientJ Emerg Med 2000 18:323-26. [Google Scholar]
[9]. Vivaldi C, Vallbohmer D, Holscher M, Holscher AH, Accidentally swallowed dentures-what is the correct diagnostic and therapeutic management?Zentralbl Chir 2008 133:82-85. [Google Scholar]