Malaria poses a great socioeconomic burden on humanity, causing about 2414 deaths daily and slowing the economic growth by 1.3% per year in the endemic areas. According to the World Malaria Report 2011, in the South East Asian (SEA) region, both the highest number of confirmed cases (1,495,817) and the highest number of deaths (1023) were reported from India. So, extensive and in-depth studies are imperative and urgent in this region [1].
Further, among the population which lives in the malaria endemic areas, infants, young children and pregnant women have been identified as the high risk groups [1]. This study was conducted on infants and children to observe the behavioural pattern of the P. Vivax infections. However, recently, a few reports have been published with a limited number of cases, where complications which owed to P.vivax in adults [2,3], as well as in children were Sectionreported [4,5]. Here, we are presenting a large retrospective, hospital-based study on complicated malaria, which was caused by a mono-infection with P. Vivax in the paediatric population. In the present study, the patients who were admitted with P. Vivax malaria were analyzed for a whole spectrum of severe illnesses. The possibilities of other co-morbid conditions, like P. Falciparum malaria and dengue, were excluded.
MATERIALS AND METHODS
The present, retrospective, observational study was conducted at a tertiary-care hospital in the National Capital Region (NCR), India. All the cases of malaria which were confirmed by blood smear examinations (both thick and thin films) and the rapid malarial antigen test, who were between the age group 0 to 18 years, who were admitted during the period from October 2009 to September 2011, were enrolled. PCR for malaria could not be performed, since this was a retrospective study. The clinical and epidemiological findings were noted after categorizing the patients into 3 categories, depending on their age; into 0-5 years, 5+-12 years and 12+-18 years.
Exclusion criteria
Those who tested positive for P. Falciparum or were co-infected with P. Falciparum.
Co-existing infections which were confirmed by investigations.
The patients who were treated with antibiotics along with antimalarials.
The patients who had positive peripheral blood smears or positive rapid malaria tests alone.
Incompletely investigated cases as were defined in the investigations.
Investigations
A complete haemogram, a typhi-dot test, the Dengue serology, blood culture, the liver function test, the renal function test, urine analysis and X-ray of the chest were performed in all the cases as a part of the routine investigations on febrile patients. Whenever they were indicated, blood gas analysis, prothrombin time, fundus examination, lumbar puncture and CSF examination, CT scan, Electroencephalogram (EEG), Ultrasonography (USG) of the whole abdomen, specific tests for viral markers (in cases of liver impairment and clinical jaundice), the glucose-6-phosphate dehydrogenase enzyme level, the reticulocyte count and peripheral blood smears (in cases of haemolysis) were also assessed.
For this study, Haemoglobin (Hb) levels of <5g/dl were defined as suggestive of severe anaemia and haemoglobin levels between 5-10g/dl was defined as suggestive of moderate anaemia. Thrombocytopaenia was defined as platelet counts of <150X103 cells/μL. Renal impairment was defined as oliguria (urinary output <1ml/kg/hr.) with a rise in both blood urea (>40mg/dl) and serum creatinine (>2mg/dl) as per our laboratory normal values. An isolated increase in either parameter was not considered as a marker of the renal impairment. Liver impairment was defined as a serum bilirubin level of >2mg/dl or a fourfold rise in the liver transaminase level than the normal baseline values of our lab. A circulatory impairment/shock was defined as a systolic BP of < the 70th percentile for age. Clinically, hepatomegaly was defined as a palpable liver which was >2.5 cm below the costal margin and splenomegaly was defined as any degree of palpable spleen below the costal margin. The clinical syndromes were defined according to the WHO (2000) guidelines [6] for severe malaria, except the Multi Organs Dysfunction Syndrome (MODS), which was classified on the basis of the involvement of two or more organs. The antimalarial treatment was prescribed according to the WHO guidelines for severe and non-severe malaria.
The technique which was used
The haemograms were done by using a Sysmex auto-analyzer. A rapid malaria diagnostic test was performed by using the OPTIMAL-IT kit which can detect peripheral parasitaemia levels of .001-.002% (50-100 parasites per litre of blood). This kit detects the presence of Plasmodium lactate dehydrogenase (pldh), an enzyme which is produced by both the sexual and asexual forms of the parasite. The liver function test and the kidney function test were done by using a COBAS C111 (ROCHE) auto-analyzer.
Ethics: This study was approved by the ethics committee of the institution and the medical superintendent of the hospital granted permission to access and publish the hospital data.
Statistics: A descriptive statistical analysis was done by using the SPSS software and an Excel worksheet, whenever they were required.
RESULTS
The records of 763 patients of fever who were between the ages 0-18 years, who were admitted in the study hospital from October 2009 to September 2011, were studied. Among these, both the peripheral blood examinations and the rapid diagnostic test were positive for malaria in 231 patients. Among these, 63 patients were excluded due to the exclusion criteria (P.falciparum-34, mixed-5 and other exclusion criteria-24). The subsequent analysis was done in 168 children. The age and sex distribution is shown in [Table/Fig-1 and 2].
Table showing age and sex distribution
| Age group (yrs) | Male | Female | Total |
|---|
| N | % | N | % | N | % |
|---|
| 0-5 | 21 | 12.5 | 13 | 7.7 | 34 | 20.2 |
| 5+ -12 | 32 | 19.1 | 36 | 21.4 | 68 | 40.5 |
| 12+-18 | 38 | 22.6 | 28 | 16.7 | 66 | 39.3 |
| Total | 91 | 54.2 | 77 | 45.8 | 168 | 100.0 |
Figure showing age and sex distribution
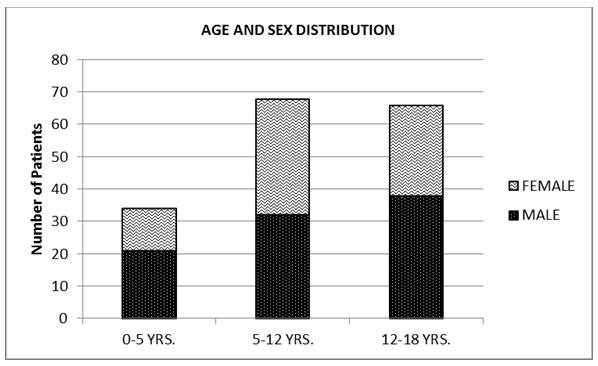
A majority of the children in the present study were between 5-18 years of age (79.7%, n=134), while 20.3% of the children (n=34) were between 0-5 years of age. There was a predominance of the male children (54.2%, n=91) over females (45.8%, n=77). The mean duration of the fever, prior to the admission at our centre, was 6±1.2 days. The average stay of the patients was 11.1 days. The various complications have been depicted in [Table/Fig-3 and 4] and the haematological/ biochemical abnormalities have been illustrated in [Table/Fig-5 and 6].
Table showing various clinical manifestations
| Age | 0-5 (n=34) | 5+-12 (n=68) | 12+-18(n=66) | Total (n=168) |
|---|
| Findings | N | % | N | % | N | % | N | % |
|---|
| Abdominal Findings | 30 | 88.2 | 25 | 36.8 | 20 | 30.3 | 75 | 44.6 |
| Hepatomegaly | 8 | 23.5 | 6 | 8.8 | 2 | 3.0 | 16 | 9.5 |
| Splenomegaly | 16 | 47.1 | 10 | 14.7 | 6 | 9.1 | 32 | 19.0 |
| Hepato and/or splenomegaly | 30 | 88.2 | 25 | 36.8 | 20 | 30.3 | 75 | 44.6 |
| Ascites | 0 | 0.0 | 2 | 2.9 | 0 | 0.0 | 2 | 1.2 |
| Hematological Findings | 34 | 100.0 | 68 | 100.0 | 66 | 100.0 | 168 | 100.0 |
| Pallor | 34 | 100.0 | 68 | 100.0 | 66 | 100.0 | 168 | 100.0 |
| Icterus | 16 | 47.1 | 7 | 10.3 | 5 | 7.6 | 28 | 16.7 |
| Petechiae | 25 | 73.5 | 12 | 17.6 | 8 | 12.1 | 45 | 26.8 |
| Gross bleeding | 6 | 17.6 | 2 | 2.9 | 1 | 1.5 | 9 | 5.4 |
| Respiratory Findings | 6 | 17.6 | 8 | 11.8 | 8 | 12.1 | 22 | 13.1 |
| Tachypnea | 6 | 17.6 | 8 | 11.8 | 8 | 12.1 | 22 | 13.1 |
| Pleural effusion | 0 | 0.0 | 1 | 1.5 | 1 | 1.5 | 2 | 1.2 |
| ARDS | 1 | 2.9 | 1 | 1.5 | 0 | 0.0 | 2 | 1.2 |
| Renal Findings | 12 | 35.3 | 3 | 4.4 | 5 | 7.6 | 20 | 11.9 |
| Oliguria | 10 | 29.4 | 2 | 2.9 | 5 | 7.6 | 17 | 10.1 |
| Hematuria | 5 | 14.7 | 1 | 1.5 | 1 | 1.5 | 7 | 4.2 |
| C.V.S. Findings | 4 | 11.8 | 2 | 2.9 | 1 | 1.5 | 7 | 4.2 |
| Shock | 4 | 11.8 | 2 | 2.9 | 1 | 1.5 | 7 | 4.2 |
| C.N.S.Findings | 5 | 14.7 | 3 | 4.4 | 2 | 3.0 | 10 | 6.0 |
| Cerebral malaria | 5 | 14.7 | 3 | 4.4 | 2 | 3.0 | 10 | 6.0 |
| Convulsions | 3 | 8.8 | 3 | 4.4 | 2 | 3.0 | 8 | 4.8 |
Figure showing various clinical manifestations
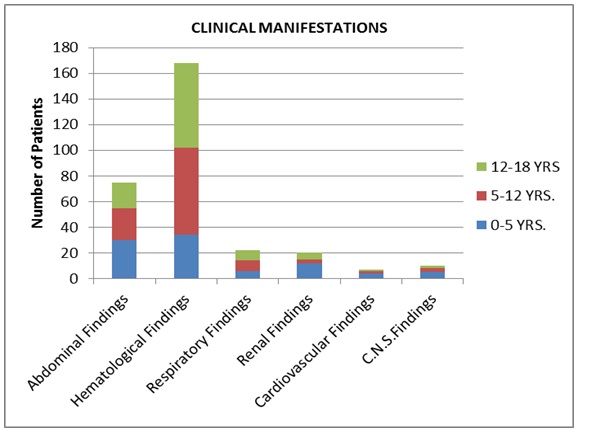
Table showing abnormal laboratory findings
| Severe Malaria Defining Laboratory Parameters | N | % | Mean ± SD | Range | Standard Error of Mean |
|---|
| Hemoglobin (g/dL) 52.94 |
| <5 | 14 | 8.3 | 3.92 ± 0.87 | 2.1 - 4.9 | 0.23 |
| 5-10 | 137 | 81.5 | 7.70 ± 1.26 | 5.0 - 10.0 | 0.10 |
| Platelet count (X103/μL) 5.88 |
| <20 | 12 | 7.1 | 13.07 ± 4.97 | 2.5-19.9 | 1.43 |
| 0–150 | 126 | 75.0 | 82.45 ±42.99 | 2.5 – 149.9 | 3.83 |
| Total leucocyte count (X103/μL) 5.88 |
| <4 | 25 | 14.9 | 3.12 ± 0.84 | 1.30 - 3.90 | 0.16 |
| Hypoglycemia |
| Blood sugar <40 mg/dl | 5 | 3.0 | 31.60 ± 5.5 | 24 - 38 | 2.48 |
| Liver dysfunction |
| Serum bilirubin >2 mg/dl | 28 | 16.7 | 4.28 ± 1.84 | 2.40 – 10.10 | 0.36 |
| AST >4 times baseline(IU/L) | 18 | 10.7 | 252.22±267.47 | 80 - 1250 | 63.04 |
| ALT >4 times baseline(IU/L) | 18 | 10.7 | 202.78±178.44 | 70-825 | 42.05 |
| Renal dysfunction |
| Serum creatinine >2 mg/dl | 16 | 9.5 | 2.65 ± 0.53 | 2.10 – 3.90 | 0.13 |
| Blood urea >40 mg/dl | 16 | 9.5 | 72.91 ± 26.30 | 44.50-151.90 | 6.57 |
Figure showing abnormal laboratory findings

The abdominal findings and the liver dysfunction: Hepatomegaly and/or splenomegaly was a frequently detected abdominal finding which was present in 44.6 %( n=75) of the cases. Among these, hepatomegaly or splenomegaly alone were present in 9.5 % ( n=16) and 19.0 % ( n=32) of the cases respectively. Further, it was observed that hepatosplenomegaly was more common in the younger children (88.2% in 0-5 age group (30/34) and that it decreased gradually with age (36.8% in the age group of 5-12 years [25/68] and 30.3% in the age group of 12-18 years (20/66). Ascites was noticed in 1.2 % ( n=2) of the total cases, both in the age group of 5-12 years. USG of the abdomen which was done in both these cases showed a mild to moderate amount of fluid in the peritoneal cavity, which was transudate in nature, which resolved with time. Liver dysfunction in the form of increased serum bilirubin>2mg/dl, was found in 16.7 %( n=28) of the cases with a mean of 4.28mg/dl, while a fourfold increased AST/ALT than the baseline was seen in 10.7 %( n=18) cases with means of 252.22 IU/L and 202.78 IU/L respectively. Hypoglycaemia (blood sugar<40 mg/dl) was seen in 3.0 %( n=5) of the cases, with a mean of 31.6mg/dl.
Haematological findings: The haematology-related clinical findings were ubiquitous and clinical pallor of various degrees was observed in all the 168 patients. A clinical icterus was observed in 16.7 % ( n=28) of the cases. As with the hepatosplenomegaly, the icterus was commonest in the 0-5 years age group (47.1%, [16/34]), thus exhibiting an incidence which decreased from 47.1% through 10.3% to 7.6% with the increasing age groups. Another common 863clinical haematological finding was a petechial rash of various degrees, which was found in 26.8% (n=45) of the children, which again showed a declining graph from 73.5% through 17.6% to 12.1% with increasing age. Gross bleeding, either per-rectum and/or haematemesis was observed in 5.4 %( n=9) of the cases. This too was most frequent in the 0-5 years age group (17.6%, (6/34). On assessing the laboratory parameters, the haematological abnormalities were found to be commonest, decreasing in frequency and severity with increasing age, as in the clinical findings. Such changes were found in 76.5%, (26/34) of the cases in the 0-5 years age group, decreasing to 17.6%, (12/68) and 13.6%, [9/66] in the subsequent age groups. Severe anaemia was observed in 8.3 %( n=14) of the cases with a mean of 3.92g/dl, while moderate anaemia was observed in 81.5% of the cases (n=137) with a mean of 7.7g/dl. Thrombocytopaenia was present in 75 %( n=126) of the cases, with a mean 82.45X103/μL. Further, it was observed that of these 126 cases, 12(7.1%) cases had a platelet count of <20X103/μL with a mean of 13.07 X103/μL. Leucopaenia was also observed, with a total leucocyte count of <4X103/μL in 14.9 %( n=25) of the cases, with a mean of 3.12X103/μL.
Respiratory findings: Respiratory manifestations in the form of tachypnoea were found in 13.1 %( n=22) of the cases and the incidence was almost equal in all the age groups. Pleural effusions (transudates) were found in 1.2 %( n=2) cases in the age group of 5-18 years. The X-rays were suggestive of combinations of infiltrates, increased bronchovascular markings, hyper inflated lungs, interstitial oedema and effusion. Acute Respiratory Distress Syndrome (ARDS) was also seen in 1.2 %( n=2) patients who were between the age group of 0-12 years. These patients were managed as per the standard protocol.
Renal findings: Renal involvement was observed clinically in a total of 11.9 %( n=20) cases, in the form of oliguria and/or haematuria/ haemoglobinuria. This renal involvement was more frequent in children who were between the age group of 0-5 years (35.3%, [12/34]) and it was less frequent in the age group of 5-18 years (6%, [8/134]). Haematuria was gross in 4 patients. Renal dysfunction, as was defined earlier by using biochemical parameters, was observed in 9.5 %( n=16) cases with a mean serum creatinine level of 2.65mg/dl and a mean urea level of 72.91mg/dl.
Cardiovascular findings: Shock was observed in 4.2 %( n=7) of the cases and it was more common in the age group of 0-5 years (11.8%, [4/34]). The mean blood pressure of the patients without shock (n=161) was 104.45/60.45mm Hg,SD±7.07/±6.52mm Hg, while the mean blood pressure of the patients with shock was 90/48mm Hg,SD±6.1/±5.53mm Hg.
Central Nervous System findings: Cerebral malaria was present in 6.0 %( n=10) cases. 80 %( n=8) of these cases presented with convulsions. The convulsions were multiple in 50 %( n=5) cases. The Cerebrospinal Fluid (CSF) examination, CT scan of the head and EEG were unremarkable in these patients. One child had an evidence of a retinal haemorrhage (the flame-shaped and the dot-blot type) on fundus examination, which resolved in due course of time. The Multi Organs Dysfunction Syndrome (MODS), as was defined earlier, was present in 6.5 %( n=11) cases and all the patients in this group recovered completely after the treatment.
No mortality was recorded in our study. All the patients recovered either before their discharge or during the follow-up of 4 weeks. All the biochemical and haematological tests returned to normal levels.
DISCUSSION
Till the last decade, severe or complicated malaria was synonymous with the P. Falciparum infection; the burden and the virulence of vivax malaria had been underestimated. The severity of the malaria which was caused by P. Vivax has increased significantly [7], but most of the public literature on severe P.Vivax malaria consists of case reports or small descriptive clinical series, which lack denominators. It was only recently that the severe disease which was caused by P. Vivax was reported in the larger studies on malaria from the SEA region, which however, included all the demographic groups and all the species of Plasmodium [2,3]. For instance, in a study which was conducted in Indonesia, 3.2% (36/1135) of the P. Vivax infected patients showed severe malaria 3 and in another study, the proportion of the malarial admissions which were caused by P. Vivax was 23% as compared to 20% P. Falciparum admissions, with the highest rate (31%) being seen in mixed infections [2]. Similarly, a study from India which was done on children who were hospitalized with malaria, showed that the risk of severe disease was greatest with the P. Vivax infections (63.1%), followed by the P. Falciparum infections (42.7%) and the mixed infections (40%) [4]. Studies from Asia and the Pacific region showed that P. Vivax malaria accounted for a substantial proportion of the hospitalized patients [2,3,8] and that it also contributed to the mortality [4,8]. This was the phase of acknowledging a new problem in an old disease. On comparing the statistics between the two major species of Plasmodium, the increasingly malignant behaviour of P. Vivax was noted and documented. However, in the next phase, studies which dealt exclusively with severe malaria which was caused by a mono-infection with P. Vivax, has just begun. Such studies are scarce [9] and a comprehensive analysis of these changing clinico-pathologic manifestations in the mono-infection with P. Vivax is awaited.
In the malaria endemic areas, infants and young children have been identified as the high risk groups, both by the WHO 1 and by independent studies [2,3,8]. The WHO has issued guidelines which have defined the potentially fatal severe malaria in children [6]. However, studies which are based on the paediatric population, are rare [4,5]. Hence, further studies are required to elucidate the pattern of severe vivax malaria in children.
Most of the previous case reports/ studies were sporadic. The studies which were undertaken so far, have revealed mainly anaemia, thrombocytopaenia and respiratory problems in severe malaria, while the involvement of other organ systems has generally been notified in the form of isolated case reports or series. The complete range of complications of vivax malaria still remains largely unexplored. The other associated co-morbid conditions have often not been ruled out or commented upon.
This hospital-based study on paediatric cases with complicated P .Vivax malaria makes a comprehensive analysis of the changing clinico-pathological manifestations, by studying the wide spectrum of both the clinical and laboratory parameters, after excluding the patients who suffered from various other infections. This retrospective study on mono-infection P. Vivax malaria included 168 patients who were between the age group of 0-18 years. Both the sexes were equally involved. It was further observed that the children who were in the age group of 0-5 years had more severe manifestations as compared to the children who were in the age group of 5-18 years. A similar observation was concluded in another study which was done in Bikaner, north-west of India, in which, the proportion of severe P. Vivax malaria was 67.4% in children who were below 5 years of age [4].
The haematological findings dominated the picture. Thrombocytopaenia (platelet counts of <150x103/μL) was a major manifestation in this study, which was detected in 75% of the cases of severe P. Vivax malaria, of which 7.1% exhibited severe thrombocytopaenia (platelet counts of <20x103/μL), which was comparable with the findings of other studies [4,5,9]. Thrombocytopaenia was described as the most common manifestation of malaria in the WHO report. Recent reports from various parts of the world suggest that the incidence of thrombocytopaenia, which was earlier considered to be rare in P. Vivax malaria, is currently similar in vivax and falciparum malaria [10]. Severe thrombocytopaenia with bleeding from the skin and the mucosal surfaces has been reported in children with P.vivax malaria [11]. In the present study, 26.8% of the children had petechial rashes, out of which 5.4% cases had severe bleeding either from the GIT and/or the renal sites. The high incidence of the petechiae and the gross bleeding may be due to the inclusion of the children who were between the ages of 0-5 years, who had exhibited a greater severity of the haematological findings (petechiae in 73.5% patients and gross bleeding in 17.6% of the patients), whereas the other studies were done either on grown-up children or in adults. The exact mechanism of the P.vivax associated thrombocytopaenia is not known. Both immunological and non-immunological factors are involved [12,13].
P. Vivax malaria has always been associated with severe and protracted anaemia. In our study, clinical pallor was noticed in 100% cases and anaemia was noticed in 89.9% cases, but severe anaemia was found in 8.3% of the cases, which was comparable with the findings of some studies 5,9but another study concluded a very high incidence (75.4%) of severe anaemia [4]. This gross difference could have been due to the prevalence of anaemia in the concerned geographical area.
Both the haemoglobin and the platelet s improved during the stay in the hospital and/or during the follow-up of those patients, although neither a blood transfusion nor a platelet transfusion was administered during their admissions. This suggested that both the anaemia and thrombocytopaenia could be attributed to malaria. In the present study, hepato- and/or splenomegaly was observed in 44.6% cases,among which hepatomegaly and splenomegaly alone were observed in 9.5% and 19.0% of cases respectively, which was comparable with the findings of other studies [4]. This was again found to be higher in the children who were below 5 years of age and this could partly explain the pathogenesis of anaemia, thrombocytopaenia and the deranged liver function tests.
Liver dysfunction was observed in 16.7% cases in the present study. Increased serum bilirubin was noticed in all the cases, but AST and ALT were markedly raised in 10.7% of children only. The WHO describes liver dysfunction, which includes hepatic encephalopathy, as the most common abnormality in the adult population with severe malaria [6]. A transient derangement of the liver function is a common feature of childhood malaria, but it can also progress to a significant deterioration in the P. Vivax mono-infection. In this study too, the predominance of conjugated hyperbilirubinaemia and raised liver enzymes which were indicative of “malarial hepatitis”, was similar to the observations of other studies [9,14]. Severe hepatic complications like hepatic encephalopathy were not observed in our study, probably because of our focus on the paediatric population. However, recently, a 35.3% incidence of hepatic encephalopathy in children has been reported from India [4].
In the present study, respiratory involvement was seen in 13.1% cases in the form of tachypnoea and respiratory distress in all the cases. This complication was almost equally distributed in all the age groups, with a slight predominance in the age group of 0-5 years, as was observed in other studies also [4]. The respiratory syndrome/respiratory distress in P. Vivax has been described by various authors [2,4,9]. Pleural effusions were observed in 2 cases. The pleural fluid was transudative in nature, it was not related to hypoproteinaemia and it recovered completely with the antimalarial treatment. Pleural effusions were also reported in another study which was done in Uttarakhand in India [9]. The exact aetiology of this effusion could not be found out, but it could be due to the sequestration [2,4], which commonly occurred in P. Falciparum, although P. Falciparum could not be detected in these cases. The acute respiratory distress syndrome (ARDS) was noted in 9.1% cases among those patients who had respiratory complications. ARDS was also reported by various authors [4,9,14,15]. The exact mechanism of the respiratory distress syndrome in P.vivax malaria is not known, but it has been postulated that the sequestration of the infected erythrocytes within the pulmonary microvasculature caused an alveolar-capillary dysfunction, which was secondary to the changes in the red blood cells and the microcirculation [15].
In the present study, hypoglycaemia was observed in 3% cases, among the patients who had respiratory complications and/or hepatic dysfunction. Many authors have described hypoglycaemia as a feature of P. Falciparum [9], while other studies confirmed our observation [4,6,14].
Renal complications were observed clinically in 11.9% cases and the incidence was much higher (35.3%) in the age group of 0-5 years. Most of the patients (10.1%) presented with oliguria. Among the cases which exhibited renal findings, haematuria/ haemoglobinuria was observed in 35% (7/20) cases and the incidence of haematuria was higher 41.6%(5/12) in the age group of 0-5 years. On laboratory estimation, both serum creatinine and blood urea were found to be raised in 9.5% of the cases. Similar complications have been reported by various authors [4,9,14]. Although the incidence of acute renal failure (ARF) was observed to be more common in P. Falciparum malaria [16], there have been reports of acute renal failure, electrolyte abnormalities, abnormal urinary sediments, and an increased urinary protein excretion in P. Vivax malaria in children, in the recent past [4,9]. The possible mechanisms like a mechanical obstruction which was caused by parasitized RBCs, microcirculatory disorders, a disseminated intravascular coagulation, fluid loss and a hypoxic or immune-mediated necrosis of the glomeruli and the renal tubules may be implicated in the vivax infection [16].
Shock was observed in 4.2% cases and it was more common (11.8%,) in the age group of 0-5 years. These patients were managed as per the standard protocol. Various studies also reported shock in P. Vivax [4,9,14,15]. This shock may be attributed to various factors like an intravascular haemolysis, fluid loss and absorption of toxins from the GIT [9].
The central nervous system involvement was traditionally linked exclusively to P. Falciparum. But in the present study, 6.0% cases presented as cerebral malaria (Blantyre coma scale ≤ 2). Among these 10 cases of cerebral malaria, 80% of the children presented with convulsions which were generalized or focal and single or multiple. The EEG and the CT scan were unremarkable. Our findings were consistent with those of many other studies/case reports, where it was documented that P.vivax also caused cerebral malaria [3,4,6,9,14,17]; some of these were documented in children [4,17]. The gravity of this recently observed “malignant” complication can be estimated by the fact that a study which analyzed the causes of death among the patients with severe malaria, which included P. Vivax malaria, observed that the commonest complication in fatal malaria was cerebral malaria [8].
Multi organ failure was found in 6.6% cases in this study, in various combinations, which included predominantly hepatic dysfunction, renal failure, severe anaemia, haemoglobinuria, ARDS and convulsions. The multi organ dysfunction syndrome has been reported by various authors from India and other parts of world [2,4,9,14]. The changing clinico-pathological spectrum of P. Vivax and its increasing virulence can be appreciated by a recent study which was done on hospitalized children, according to which, P. Vivax has a higher propensity than P. Falciparum to cause a multiorgan dysfunction in the 0-5 year age group [4].
Mortality
P. Vivax malaria is supposed to be a benign condition with no mortality, but many recent reports have suggested a significant mortality, even in P. Vivax malaria, which was caused by cerebral malaria, ARDS, hepatic encephalopathy, renal complications and/or multi organ failure [2,4,14]. In the present study, no death was reported.
CONCLUSIONS
The present retrospective study which was done on admitted cases of a mono-infection of P. Vivax concluded that P. Vivax also caused complicated malaria, leading to a spectrum of clinico-pathological manifestations which were similar to those which were described in P. Falciparum malaria. Although in the past, P. Vivax was supposed to be a benign condition, a change in virulence has been noted in the last decade or so in India and other parts of the world, with which this study is consistent.
This study was probably the largest study which was done on the P. Vivax morbidity on the admitted cases. This was a retrospective study and a large number of multi-centric prospective studies are required to strengthen our results and to judge the extent of the complicated P. Vivax malaria, after the exclusion of other concomitant infections and mixed malarial infections, with the use of the latest techniques.
It is also necessary to know why there is a change in the virulence, and whether any genetic mutation in P. Vivax is responsible for this changing pattern. Now that the P. Vivax genome is available (GenBank accession no. AAKM00000000), it will be possible to compare the isolates which are associated with the severe/ complicated cases from different geographical regions [18]. Hence, further research should be initiated regarding these issues which are related to complicated P. Vivax malaria, as it is turning into a species with the malignant potential of P. Falciparum.