ECG Changes in Smokers and Non Smokers-A Comparative Study
M.R. Renuka Devi1, T. Arvind2, P. Sai Kumar3
1 Associate Professor, Department of Physiology, Sree Balaji Medical College and Hospital, Chromepet, Chennai, India.
2 Post Graduate, Department of Physiology, Sree Balaji Medical College and Hospital, Chromepet, Chennai, India.
3 Professor and HOD, Department of Physiology, Sree Balaji Medical College and Hospital, Chromepet, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M.R. Renuka Devi, Associate Professor, Department of Physiology, 20/582, 16th Street, 4th Sector, K.K. Nagar, Chennai -78, India.
Phone: 9884190928 E-Mail: renudarshini2004@rediffmail.com
Introduction: Tobacco consumption is the single most cause of the preventable deaths globally. Tobacco is consumed in the form of cigarettes. It contains nicotine which causes physical and psychological dependencies. Cigarette smoking increases the blood coagulability. Nicotine facilitates conduction block, re-entry and it increases the vulnerability to ventricular fibrillation. Hence, Nicotine and other components of cigarette can produce profound changes in the heart, which can be assessed by doing an ECG, which is the, cheapest and the most reliable method for assessing cardiovascular abnormalities.
Aim: To compare the ECG changes between smokers and non- smokers.
Materials: Eighty eight healthy male volunteers who were in the age group of 18-30 years, who attended the outpatients department of SBMCH were recruited for the study. Among the volunteers, 44 were smokers as per the ICD-10 criteria for substance abuse and the rest of the 44 were non-smoker subjects without any systemic illnesses and a drug and alcohol intake.
Methods: After a thorough examination, all the subjects were asked to abstain from smoking and caffeine beverages, 2 hours prior to the taking of the ECG recording. The ECG was recorded in the lab of the Department of Physiology of SBMCH. The following parameters were assessed, namely, the heart rate, the p- wave, the PR interval and the QRS complex. The QTc (corrected QT interval) was calculated by using Bazet’s formula. The QT interval, the ST segment and the T wave duration were evaluated in seconds. The results which were obtained were statistically analyzed by using the Students ‘t’ test.
Results: The analysis showed that QTc interval was shortened and that the QRS complex duration was widened in the smokers, although the values did not show any statistical significance. The heart rate was increased in the smokers, which was statistically significant. The RR interval, the QT interval and the ST segment were shortened in the smokers as compared to those in the non smokers, which was highly significant statistically.
Conclusion: All the above changes in our study were either a result of the acute effects or the chronic effects of smoking, which led to cardiovascular disorders which could be easily identified by the wave duration in electrocardiography. This may be used by physicians as a tool for counselling the smokers to stop smoking as early as possible. Smoking even a sin
Electrocardiography, Nicotine, Smoking
INTRODUCTION
Tobacco consumption has many worse health outcomes. Tobacco consumption is the single most cause of the preventable deaths globally. Tobacco is consumed in many forms and one such form is cigarette smoking. Its use leads to heart attacks, chronic obstructive pulmonary disease, cancer, peripheral vascular disease, hypertension and the list is endless [1,2]. It contains nicotine which causes physical and psychological dependencies.
It was estimated that there were 100 million deaths worldwide in the 20th century and currently, there are 5.4 million deaths every year. It has also been estimated that by 2030, there will be more than 8 million deaths every year [3]. Nicotine, which is the main component of tobacco, causes sudden coronary death [4]. Nicotine also causes cardiac death by provoking ventricular arrhythmias [5,6]. The cardiac effects of nicotine are attributed to the release of catecholamine [7], which are released due to the binding of nicotine to the nicotinic cholinergic gate on the cation channels in receptors (nAchRs) throughout the body. A longer retention of nicotine occurs in the blood and in other specific tissues such as the oesophagus, fundus ,antrum, spleen, caecum, pancreas,testes, heart and the muscle via a constant exposure”[8]. Nicotine facilitates a conduction block and a re-entry and it increases the vulnerability to a ventricular fibrillation [9]. Nicotine is a potent inhibitor of the cardiac A type potassium channels, which contributes to the changes in the electrophysiology and it also induces arrhythmias [10].
Hence, nicotine and other components of cigarette smoking produce profound changes in the heart which can be assessed by doing an ECG, which is the easiest and the cheapest method for assessing cardiovascular abnormalities. Maintaining abstinence from smoking as early as possible can prevent further damage. This study was aimed at creating an awareness on the smoking hazards.
AIM
To compare the ECG changes between smokers and non- smokers.
MATERIALS
Eighty eight healthy male volunteers who were in the age group of 18-30 years, who attended the outpatients department of Sree Balaji Medical College and Hospital, were recruited for the study after obtaining written informed consents from them. The institutional ethical committee clearance was also obtained. This study was done over a period of 3 months. Out of the volunteers, 44 smokers were selected as per the World Health Organization’s (WHO’s) 10th revision of the International Statistical Classification of Diseases and related health problems (ICD-10) criteria of harmful use [11] and the rest of the 44 were non-smoker subjects without any systemic illnesses and drug and alcohol intake.
All the subjects were asked to abstain from smoking and caffeine beverages 2 hours prior to the ECG recording. Thorough clinical and systemic examinations were done. With the subjects in the resting supine position, a 12 lead electrocardiogram was recorded by using a single channel ECG cardiant (heart view 1200 ECG recorder-manufactured by Brown Dove Healthcare Pvt Ltd ) [12] in the research lab of the Department of Physiology of Sree Balaji Medical College and Hospital, India.
The following parameters were assessed, namely, the heart rate , the PR interval and the QRS complex. The QTc (corrected QT interval) was calculated by using Bazet’s formula (QT interval/square root of the RR interval) [13]. The QT interval, the ST segment and the T wave duration were evaluated in seconds.
The results which were obtained were statistically analyzed by using the Student’s ‘t’ test. The probability (p- value) was calculated . A p-value of < 0.001 was taken as highly significant, a p-value of <0.05 as significant and a p-value of >0.05 as non- significant.
RESULTS
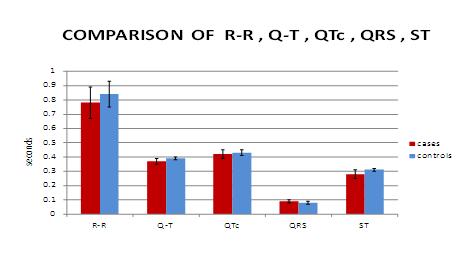
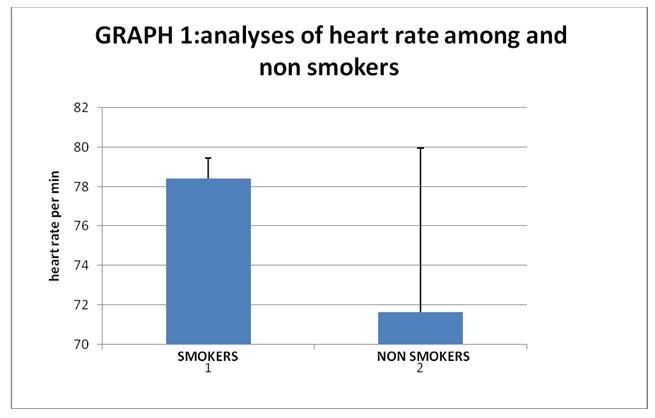
[Table/Fig-1 and 2] show that the QTc interval was shortened and that the QRS complex duration was widened in the smokers, although the values did not show statistical significance. The heart rate [Table/Fig-3] was increased in smokers, which was statistically significant. The [Table/Fig-2] shows that the RR interval, the QT interval and the ST segment were shortened in the smokers as compared to those in the non smokers, which was highly significant statistically.
Showing analyses of ECG waves among smokers and non- smokers
| Parameters | Smokers (n-44) | Non-Smokers (n-44) | P-Value |
|---|
| Heart rate per min | 78.40±11.06 | 71.65±8.31 | 0.002* |
| RR interval in sec | 0.78±0.11 | 0.84±0.09 | 0.003* |
| QT segment in sec | 0.37±0.02 | 0.39±0.01 | 0.000* |
| QTc Interval in sec | 0.42±0.03 | 0.43±0.02 | 0.121 |
| QRS complex in sec | 0.09±0.01 | 0.08±0.009 | 0.040 |
| ST segment in sec | 0.28±0.03 | 0.31±0.01 | 0.000* |
*p- value (<0.001) – statistically significant
Comparison of ECG wave duration among smokers and non smokers
Analyses of heart rate among and non smokers
DISCUSSION
According to a similar study which was done by Venkatesh G et al., recently, in the year 2010, the results showed a significant shortening of the QRS complex, whereas the other waves did not show much change [12]. Our study showed [Table/Fig-3] widening of the QRS complex and shortening of the QTc interval in smokers and non smokers, which were not statistically significant, which were similar to the results of a study which was done by Karjalainen et al., [14], which explained that a shortened QT interval was as a risk factor for smokers, which could cause death.
The shortened QT and ST segments [Table/Fig-3] warn that there may be Shortening in the ventricular filling phase, during which the coronary supply occurs. This may lead to an insufficient myocardial perfusion, which may invite ischaemic episodes. Such altered ventricular electrical activities, like a widened QRS complex and a shortened ST segment also predisposes smokers to episodes of arrhythmia. The increase in the heart rate which was shown in our study was due to an increased catecholamine secretion from the adrenal medulla [7]. There are studies whose results prove that single cigarette smokers also may develop coronary vasoconstriction [15]. There are also studies which are very similar to our study, which were done by Vandan V et al., where they have assessed the blood pressure and the ECG in smokers and have compared them with those of the non smokers. They found that the pulse rate and the blood pressure were raised in the smokers to that of hypertensive values but with no significant change in the ECG [16]. These findings were similar to those of our study, where the heart rate was raised and there were changes in the ECG, which were not statistically significant, but clinically, each ECG wave had to be analyzed and it has to be attributed to smoking.
These changes, namely, coronary spasms and a shortened ventricular filling, together decrease the coronary perfusion, leading to coronary artery disease.
CONCLUSIONS
All the above changes in our study were either result of the acute effects or the chronic effects of smoking, which could lead to cardiovascular disorders, which could be easily identified by the wave duration in electrocardiography, which could have been used by the physician to counsel the smokers to stop smoking as early as possible. Smoking even single cigarette can increase the risk of sudden cardiac deaths. In the long term, the mortality which is caused by smoking is either due to coronary artery disease or due to electrophysiological disturbances, which lead to arrhythmias.
*p- value (<0.001) – statistically significant
[1]. Ockene IS, Miller NH, Cigarette Smoking, CVS disease and Stroke. A Statement for healthcare professionals from the American Heart AssociationCirculation 1997 96(9):3243-47. [Google Scholar]
[2]. Health effects of cigarette smoking, Centers for Disease Control and Prevention [Google Scholar]
[3]. WHO Report on the Global Tobacco epidemic 2008, WHO [Google Scholar]
[4]. Lakier JB, Smoking and cardiovascular diseaseAm J Med 1992 93:8S-12S. [Google Scholar]
[5]. Chevalier HJ, Hunnigh C, Bandilla B, Dontenwill Hanel JW, Effect of high doses of nicotine in pig, I: Changes of the electrocardiogramBasic Res Cardiol 1976 71:68-75. [Google Scholar]
[6]. Escobed LG, Zack MM, Of sudden and non sudden coronary deaths in the United StatesCirculation 1996 93:2044-36. [Google Scholar]
[7]. Stewart PM, Cetterall JR, Chronic nicotine ingestion and atrial fibrillationBr.Heart J. 1985 54:222-23. [Google Scholar]
[8]. Chowdhury P, Doi R, Chang LW, Rayford PL, Tissue distribution of [3H]-nicotine in ratsBiomed Environ Sci 1993 6:59-64. [Google Scholar]
[9]. Yashima M, Ohara T, Cao JM, Kim YH, Fishbein MC, Mandel WJ, Nicotine increases ventricular vulnerability to fibrillation in hearts with healed myocardial infarctionAm.J Physiol Heart Circ Physiol 2000 Jun 278(6):H2124-33. [Google Scholar]
[10]. Huizhenwang Hang Shi MD, Baofeng Yang, Nicotine is a potent Blocker of the cardiac A- type K+ChannelsCirculation 2000 102:1165-71. [Google Scholar]
[11]. WHO Geneva Diagnostic criteria for research .ICD -10 classification of mental and behavioural disorders. 1993;75 [Google Scholar]
[12]. Venkatesh G, Swamy RM, A study of electrocardiographic changes in smokers compared to normal human beingsBiomedical Research 2010 21(4):389-92. [Google Scholar]
[13]. Bazett HC, “An analysis of the time-relations of electrocardiograms”Heart 1920 7:353-70. [Google Scholar]
[14]. Karjalainen J, Reunanen A, Ristola P, Vitasalo M, QT interval as a cardiac risk factor in a middle aged populationHeart 1997 Jun 77(6):543-48. [Google Scholar]
[15]. Tsuchiya. M Smoking a single cigarette rapidly reduces combined concentrations of nitrate and nitrite and concentrations of antioxidants in plasma. Department of Biochemistry and Molecular Pathology. Osaka city University Medical School, Abenobu, Osaka, Japan [Google Scholar]
[16]. Chiddarwar Vandan V, Chiddarwar VA, Jain Jinendra M, Singhania Snita S, Int J Pharm Biomed Sci 2012 3(4):220-23. [Google Scholar]