The Prospect of Serum Magnesium and an Electrolyte Panel as an Adjuvant Cardiac Biomarker in the Management of Acute Myocardial Infarction
Ramesh Ramasamy1, Sathish Babu Murugaiyan2, Niranjan Gopal3, Rachel Shalini4
1 Professor & Head, Department of Biochemistry, Mahathma Gandhi Medical College and Research InstitutePillayarkuppam Puducherry - 605 402, India.
2 Assistant Professor, Department of Biochemistry, Mahathma Gandhi Medical College And Research Institute, Pillayarkuppam, Puducherry - 605 402, India.
3 Assistant Professor, Department of Biochemistry, Mahathma Gandhi Medical College And Research Institute, Pillayarkuppam, Puducherry - 605 402, India.
4 First year MD Student, Department of Biochemistry, Mahathma Gandhi Medical College And Research Institute, Pillayarkuppam, Puducherry - 605 402, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ramesh Ramasamy, Professor & Head, Department of Biochemistry, Mahathma Gandhi Medical College and Research Institute Pillayarkuppam Puducherry - 605 402, India. Tel: +91 – 4132615449, Extension- 602 Fax: +91 - 0413 -2615457
E-mail: rameshrdr30@gmail.com
Background: Ischemic heart disease accounts 12.2% deaths worldwide. Serum magnesium (Mg+) status is often ignored in Acute Myocardial Infarction (AMI). Studies showed alterations in the levels of serum electrolytes including magnesium in AMI.
Aim: To evaluate serum Mg+ and other electrolytes as adjuvant markers in the diagnosis of AMI.
Design and Settings: Case control study was conducted in South Indian male population with AMI within six hours of onset of symptoms.
Patients and Methods: Study includes sixty patients with AMI and 100 controls. Serum electrolytes were estimated using electrolyte analyzer. Data were compared by using student‘t’ test. ROC was drawn to find out optimum cutoff for diagnosing AMI. Pearson’s correlation was done to see the association among the markers.
Results: Serum Ca, Mg, K and Na electrolytes were significantly lower (‘p’<0.001) in AMI. Ca:Mg, K:Mg, and Na:K ratios were significantly higher when compared to controls (‘p’<0.001). There was significant correlation of serum Mg levels with other cardiac markers (Total CK, CK–Mb, Troponin –T) of AMI (‘p’ <0.05).ROC analysis of Na:Mg (40.9), Ca:Mg (3.43) and K:Mg (2.74) ratios showed optimum cutoffs in diagnosis of AMI.
Conclusion: Serum Mg, Ca:mg, K:mg and Na:K ratios could be useful adjuvant markers in diagnosis of AMI.
Acute myocardial infarction, Magnesium, Electrolytes, Diagnostic marker, optimum cut off
INTRODUCTION
The prevalence of myocardial infarction (MI) is more in the middle income world; (WHO report, 2004) and it is well known that males are more commonly affected than females. In the era of evidence based medicine, biochemical markers have become a prime factor in the diagnostic evaluation of patients with symptoms of myocardial infarction, which include myoglobin, troponins and creatine-kinases, ischsemia modified albumin (IMA), heart fatty acid-binding protein, hsCRP, brain natriuretic peptide, etc [1-4].
Magnesium is the second most abundant intracellular cation and it is vital for more than 300 enzymatic reactions which are involved in various metabolic processes in our body, but still, it is often a parameter which is overlooked by the clinicians [5]. Magnesium is a cardio protective element because of its β adrenoreceptor blocking action, antiplatelet action and inhibitory effect on the cardiac conducting system [6,7]. The ion stabilizing effect of magnesium helps in maintaining stable intra and extracellular concentrations of other electrolytes. Studies have documented significant alterations in magnesium (Mg+2) and other electrolytes in patients with Acute Myocardial Infarction (AMI) [8,9].
The status of intracellular Mg+2 is closely linked to the cellular ionic balance of sodium, potassium and calcium. Magnesium deficiency is associated with a decrease in the intracellular potassium and an increase in the calcium and sodium concentrations. Moreover, Mg deficiency can even potentiate oxidative injuries on the post ischaemic myocardium [10]. However, the correlation between the serum electrolytes and the established biochemical and clinical markers remains unclear till date. Despite the numerous reports on the use of magnesium as an adjuvant therapy in MI, its effective use in the diagnosis of AMI is still not validated. So, the present study was conducted to explore the role of magnesium and other electrolytes in the diagnosis and management of myocardial infarction.
MATERIALS AND METHODS
After obtaining an ethical clearance from the institute, the present study was conducted on the male population, which included 100 healthy volunteers and 60 patients with recent onset acute myocardial infarction according to the European Society of Cardiology (ESC), the American College of Cardiology (ACC), the American Heart Association (AHA) and the World Heart Federation (WHF) jointly [11]. The age of the study groups was 50- 65 years. The patients with Diabetes, a past history coronary disease with or without heart failure, hepatorenal disorders, tuberculosis and endocrinal disorders and those who received drugs which affected the magnesium levels were excluded from the study. The blood samples were collected within 12 hours after the onset of chest pain. The samples which were collected from the patients were separated at 3000 rpm minutes by using a Remi-clinical centrifuge. Sera were separated from the samples and they were used for the estimation of Magnesium, Troponin, and Creatine –kinase by IFCC approved commercial reagent kits which had adapted to an Olympus Auto analyzer. The serum levels of sodium, potassium and ionized calcium were estimated by using an ion selective electrode and an instrumentation labelled Electrolyte analyzer.
STATISTICAL ANALYSIS
The data was analyzed by using the SPSS software, version 17. The values were expressed as mean and standard deviation. The independent “t” test was performed to compare the mean values between the cases and the controls. Pearson’s correlation analysis was performed to assess the association between the various test parameters. A p value of <0.05 was considered to be significant. Receiver Operating Curves (ROCs) were drawn to find the optimum sensitivity, specificity and the cut-off values. The sample size was calculated by using the Master 2.0 software, CMC, Vellore, India with a power of 80%.
RESULTS
As compared to the control group, the patients with AMI were found to have significantly low levels of serum magnesium, calcium, sodium and potassium, with ‘p’ values of <0.001 [Table/Fig-1]. There was a significant increase in the serum total CK, CK–Mb, Troponin –T and the relative index, with ‘p’ values of <0.001. The serum Ca/Mg and K/Mg values and the Na/K ratio were significantly higher in the AMI patients as compared to those in the control group, with ‘p’ values of <0.001 [Table/Fig-2]. As has been depicted in [Table/Fig-3], there were significant correlations of the serum magnesium ratios with CK–Mb and Troponin in the AMI patients with ‘p’ values of <0.05.
Mean and S.D of serum electrolytes and magnesium levels in AMI cases and controls.
| Parameters | Control (n=100) | Acute Myocardial Infarction (n=60) | P Value |
|---|
| Serum Mg (mmol/L) | 1.57±0.2 | 0.78±0.1* | <0.001 |
| Serum Na (mmol/L) | 135.4±3.1 | 125.4±2.5* | <0.001 |
| Serum K (mmol/L) | 3.8 ± 0.2 | 2.5±0.19* | <0.001 |
| Serum | 5.1± 0.2 | 3.17±0.14* | <0.001 |
| Ionized Ca (mg/dl) |
| Serum Total CK (IU) | 216.3 ± 32.4 | 594.8±90.1* | <0.001 |
| Serum CK-Mb (IU) | 3.1± 2.56 | 55.7±6.4* | <0.001 |
| Serum Troponin –T | 0.038±0.03 | 0.608±0.15* | <0.001 |
| Relative index | 1.55±0.2 | 9.48±1* | <0.001 |
Data presented are mean ± SD. The *depicts p < 0.05 in comparison with Control group; Analysis of data was done independent “t”-test
Comparison of serum Ca/Mg, K/Mg, Na/K ratio between control and AMI patient
| Parameters | Control (n=100) | Acute Myocardial Infarction (n=60) | P Value |
|---|
| Ca/Mg ratio | 3.27±0.44 | 4.1± 0.67* | <0.001 |
| K/Mg ratio | 2.46±0.36 | 3.2 ±0.47* | <0.001 |
| Na/k ratio | 35.5±2.1 | 49.8±0.37* | <0.001 |
Data presented are mean ± SD. The *depicts p < 0.05 in comparison with Control group; Analysis of data was done independent “t”-test
Correlation analyses of serum electrolyte panel ratios with other biochemical parameters in acute myocardial infarction
| Parameters | ‘r’ value | ‘p’ value |
|---|
| Ca/Mg ratio | Vs CK nac | 0.424 | <0.001 |
| Ca/Mg ratio | Vs CK-MB | 0.899 | <0.001 |
| Ca/Mg ratio | Vs Troponin | 0.872 | <0.001 |
| K /Mg ratio | Vs CK nac | 0.524 | <0.001 |
| K /Mg ratio | Vs CK-MB | 0.781 | <0.001 |
| K /Mg ratio | Vs Troponin | 0.822 | <0.001 |
Pearson correlation analysis was done;p < 0.05 considered significant
[Table/Fig-4]. The Receivor Operating Charesteristic curve (ROC) of Na/Mg showed an optimum cut off at 40.9 with 100% sensitivity and 90% specificity, with a significant area under the curve. The 818iCa/Mg ratio of showed an optimum cut off at 3.43 with 96% sensitivity and 78% specificity, with a significant area under the curve (AUC=0.883). The K/Mg ratio showed an optimum cut off at 2.74 with 89% sensitivity and 80% specificity, with a significant area under the curve (AUC=0.924) in the Acute Myocardial Infarction patients [Table/Fig-5].
ROC of serum electrolyte and its ratios in diagnosis of Acute Myocardial Infarction
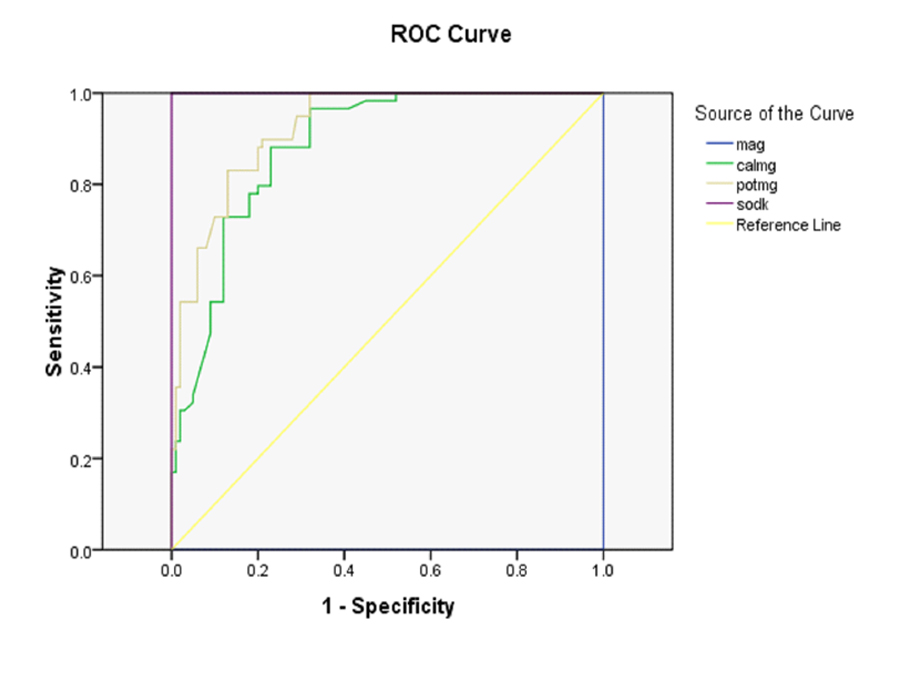
Roc of ratios of serum Mg ratio with acute myocardial infarction
| Parameters | Optimum cutoff | Sensitivity | specificity | AUC |
|---|
| Ca/Mg ratio | 3.43 | 96% | 78% | 0.883 |
| K/Mg ratio | 2.74 | 89% | 80% | 0.924 |
| Na/Mg | 40.9 | 100 | 90 | 1.00 |
DISCUSSION
In the present study, the serum magnesium, ionized calcium, sodium and potassium levels were significantly lower in the AMI patients, which was similar to those which were seen in other studies [12–15]. Our study also supported the hypothesis that the alterations in the electrolyte levels could prompt the pathological events in coronary heart diseases [12]. A study which was done by Shimoswa T et al., demonstrated that the action of magnesium on the vascular smooth muscles was primarily mediated through the L-type calcium channels. When the status of the magnesium concentration is low in the body, the normal vascular muscle tone will be lost, which can worsen the event of a myocardial infarction [16].
A study which was done by Singh RB et al., stated that the addition of Mg and K salts to the AMI treatment regimen could enhance the tissue levels of these cations, leading to a significant reduction in the complications and the mortality after 2 years [17]. The possible mechanism for the low concentrations of sodium and potassium in AMI is the impairment of the Na/K pump and the Na/Ca exchanger. The active transport of these ions across cell membrane involves ATPase, which is in turn, dependent on Mg for its activity [18].
Although Mg+ and Ca+ share similar chemical properties, their actions are opposite to those of one another. The theory of Seelig and Heggtveit states that the magnesium deficient status and an altered electrolyte concentration are caused by the reduction of the Na/K ATPase activity, leading to sodium accumulation in the cardiac myocytes. Elevated myocardial sodium levels would result in the reversal of the Na+/k+ exchange and a rise in the intracellular calcium levels [19].This intracellular shift in calcium decreases the ionized calcium levels in the serum. This explains the electrical instability in the hearts of magnesium deficient individuals. In our study, we compared the levels of magnesium with those of other routine electrolytes and we also calculated the Ca: Mg, the K: Mg and the Na: K ratios which were comparatively higher in the AMI patients than in the control groups. The Ca: Mg and the K: Mg ratios showed significant correlations with other established cardiac markers like creatine kinase- MB and troponin.The present study showed that at the optimum cut-off of 3.43, the Ca: Mg ratio had a sensitivity of 96% and a specificity of 78% to detect AMI. The optimum cut-off for the Na/Mg ratio was 40.9 with 100% sensitivity and 90% specificity and the K/Mg ratio showed an optimum cut-off at 2.74 with 89% sensitivity and 80% sensitivity for the diagnosis of AMI. Only one study which was done by Speich M et al., documented an alteration in the Mg: Ca and the K: Na ratios in heart muscles after an acute myocardial infarction [20].
Few previously documented reports have shown a correlation between the magnesium levels and other electrolytes, but studies which were related to a correlation between magnesium and the cardiac enzymes showed inconclusive results [21,22]. This can be due to the variations in the time of the sample collection and the infarct size [23]. In our study, there was a negative correlation between the cardiac markers and the K/Mg ratio and the Ca/Mg ratio. This could be because of a greater decrease in the levels of Mg than in those of calcium and potassium. Further, the decrease in the serum potassium concentration was greater than that of sodium in the AMI patients. More than the serum Mg levels, the intracellular Mg concentration reflects the total Mg status accurately. This may be the reason why many studies could not establish the exact role of the serum Mg measurement in AMI. To overcome this and also keeping in mind the fact that measuring the intracellular Mg could be time consuming, in this study, we calculated the ratios of serum Mg and other electrolytes to explore their relevance in the management of AMI. However, in this study, we didn’t correlate the ratios with the infarct size or the left ventricular function, which could have provided more information regarding the relationship between these ratios and the clinical outcome of the patients with AMI. This could be the scope of future studies, to further document the utility of these ratios in the day to day management of AMI.
CONCLUSIONS
The Ca: Mg, the K: Mg and the Na: K ratios should be included in the routine panel as a part of the management of AMI. These could be cost effective and time saving adjuncts in the management of myocardial infarction. Further studies are needed to establish the utility of these markers as effective cardiac biomarkers.
Data presented are mean ± SD. The *depicts p < 0.05 in comparison with Control group; Analysis of data was done independent “t”-test
Data presented are mean ± SD. The *depicts p < 0.05 in comparison with Control group; Analysis of data was done independent “t”-test
Pearson correlation analysis was done;p < 0.05 considered significant
[1]. Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB, Prediction of coronary heart disease using risk factor categoriesCirculation 1998 May 12 97(18):1837-47. [Google Scholar]
[2]. The global burden of disease 2004 updateWHO 2008 :16-18. [Google Scholar]
[3]. van Belle E, Dallongeville J, Vicaut E, Degrandsart A, Baulac C, Montalescot G, Ischemia-modified albumin levels predict long-term outcome in patients with acute myocardial infarction. The French Nationwide OPERA studyAm. Heart J 2010 Apr 159(4):570-76. [Google Scholar]
[4]. Lewandrowski K, Chen A, Januzzi T, Cardiac Markers for Myocardial Infarction: A Brief ReviewAmerican Journal of Clinical Pathology 2002 118:S93-S99. [Google Scholar]
[5]. Shaikh S, Karira KA, Magnesium deficiency in heart failure patients with diabetes mellitusJ Pak Med Assoc 2011 Sep 61(9):901-3. [Google Scholar]
[6]. Rasmussen HS, Justification for intravenous magnesium therapy in acute myocardial infarctionMagnes Res 1988 Jul 1(1-2):59-73. [Google Scholar]
[7]. Myoishi M, Kitakaze M, A role of magnesium: magnesium in the therapy for cardiovascular diseasesClin Calcium 2005 Feb 15(2):265-70. [Google Scholar]
[8]. Maciejewski P, Bednarz B, Chamiec T, Górecki A, Łukaszewicz R, Ceremuzynski L, Acute coronary syndrome: potassium, magnesium and cardiac arrhythmiaKardiol Pol 2003 Nov 59(11):402-07. [Google Scholar]
[9]. Aziz F, Doddi S, Penupolu S, Del Castillo D, Raza W, Kallu S, Prognostic Implication of Hyponatremia in Setting of Myocardial InfarctionChest 2011 Oct 1 140(4 Meeting Abstracts):986A-986A. [Google Scholar]
[10]. Kharb S, Singh V, Magnesium deficiency potentiates free radical production associated with myocardial infarctionJ Assoc Physicians India 2000 May 48(5):484-85. [Google Scholar]
[11]. Thygesen K, Alpert JS, White HD, Jaffe AS, Apple FS, Galvani M, Universal definition of myocardial infarction Kristian Thygesen, Joseph S. Alpert and Harvey D. White on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial InfarctionEur Heart J 2007 Jan 10 28(20):2525-38. [Google Scholar]
[12]. Solini A, Zamboni P, Passaro A, Fellin R, Ferrannini E, Acute vascular events and electrolytes variations in elderly patientsHorm. Metab. Res 2006 Mar 38(3):197-202. [Google Scholar]
[13]. Ising H, Günther T, Bertschat F, Ibe K, Stoboy V, Heldman E, Alterations of electrolytes in serum and erythrocytes after myocardial infarctionMagnesium 1987 6(4):192-200. [Google Scholar]
[14]. Product Abstract: MAGNESIUM [Internet]. LifeExtension.com. [cited 2012 Aug 25]. Available from: http://www.lef.org/prod_hp/abstracts/php-ab236.html [Google Scholar]
[15]. Aalbers TG, Houtman JPW, Relationships between trace elements and atherosclerosisScience of the Total Environment 1985 Jun 43(3):255-83. [Google Scholar]
[16]. Shimosawa T, Fujita T, [Magnesium and N-type calcium channel]Clin Calcium 2005 Feb 15(2):239-44. [Google Scholar]
[17]. Singh RB, Pella D, Neki NS, Chandel JP, Rastogi S, Mori H, Mechanisms of acute myocardial infarction study (MAMIS)Biomedicine and Pharmacotherapy 2004 Oct 58(Supplement 1(0)):S111-S115. [Google Scholar]
[18]. Sheehan JP, Seelig MS, Interactions of magnesium and potassium in the pathogenesis of cardiovascular diseaseMagnesium 1984 3(4-6):301-14. [Google Scholar]
[19]. Seelig MS, Heggtveit HA, Magnesium interrelationships in ischemic heart disease: a reviewAm. J. Clin. Nutr 1974 Jan 27(1):59-79. [Google Scholar]
[20]. Speich M, Bousquet B, Nicolas G, Concentrations of magnesium, calcium, potassium, and sodium in human heart muscle after acute myocardial infarctionClinical Chemistry 1980 26(12):1662-65. [Google Scholar]
[21]. Forster A, Stalder R, Bloch A, Suter P, The value of serum magnesium estimations in the diagnosis of acute perioperative myocardial infarction after coronary artery surgeryJ Cardiovasc Surg (Torino) 1981 Apr 22(2):163-65. [Google Scholar]
[22]. Bunton RW, Value of serum magnesium estimation in diagnosing myocardial infarction and predicting dysrhythmias after coronary artery bypass graftingThorax 1983 Dec 38(12):946-50. [Google Scholar]
[23]. Boshtam M, Najafian J, Sarraf-Zadegan N, Rafiei M, The relation between creatine kinase, magnesium and fibrinogen in patients with acute myocardial infarctionIsfahan cardiovascular research institute 2009 [Google Scholar]