The Acute Coronary Syndrome (ACS) represents a spectrum of diseases which range from ‘Unstable Angina (UA)’ which is associated with a reversible myocardial cell injury, to an ST-segment elevation ‘Myocardial Infarction (MI)’ which is associated with irreversible myocardial necrosis [1]. In today’s world, about 17 million deaths occur due to Cardiovascular Disease. In India, the number of deaths which are caused by Ischaemic heart disease increased from 1.17 million in 1990 to 1.59 million in 2000 and to 2.03 million by 2010 [2]. The diagnostic approach and the clinical management of the patients who present with a suspected acute coronary syndrome or cardiac dysfunction are challenging [3].
The manifestations of myocardial ischaemia are varied and multiple, like chest pain, epigastric discomfort, breathlessness, nausea and vomiting. However, these symptoms may be subtle and they may not be easily recognized. Because of their varied Phatakepresentations and as they are associated with high mortality, an early identification of the patients with acute myocardial infarction is very critical [4].
Assessment of the cardiac biomarker levels (Myoglobin, Creatine Kinase-MB and Troponins) is one of the most essential and effective ways for detecting myocardial damage. The current conventional cardiac markers, CK-MB, Troponin I (TnI) and T are sensitive and specific tests for the detection of myocardial necrosis, but they show a greater rise approximately 3-6 hours after the onset of the myocardial cell injury and thus, the patients may wait before they are diagnosed and treated; moreover, the usual biomarkers may not rise during reversible myocardial ischaemia and other diagnostic tools such as stress testing, and echocardiology are not routinely available [5].
Recent research has found that Ischaemia Modified Albumin (IMA) is an ideal biomarker for ischaemia. IMA is a form of human serum albumin in which the N-terminal amino acids have been modified by ischaemia. This modification reduces the affinity of plasma albumin to bind to heavy metal ions such as cobalt [6]. Bhagwan et.al and others have shown increased IMA levels in patients with spontaneous coronary ischaemia, with abnormal values which are detectable before the subsequent increases in the cardiac Troponin [7]. Most of the biomarkers are negative in acute myocardial ischaemia such as UA, but IMA is highly sentisitive and detectable in the reversible early phase of ACS. Initially, the test was named as the Albumin Cobalt Binding (ACB) assay, since it was based on human serum albumin for the metal ions (cobalt COII) in patients with ischaemia [4].
Very few studies have been reported on the serum IMA testing and on its application in the Indian context. The aim of our study was to compare the clinical performance of IMA and cardiac TnI for an early diagnosis of ACS in patients who presented with the symptoms of acute chest pain.
MATERIAL AND METHOD
The present diagnostic case-control study was conducted at the Departments of Biochemistry in PDVVPF’s Medical College, Ahmednagar and at the Swasthya Hospital and Research Centre, Ahmednagar (Maharashtra, India), in collaboration with the Departments of Biochemistry, B.J. Medical College and the Sassoon General Hospital, Pune. This study was approved by the ethics committees of B.J. Medical College and Sassoon General Hospital, Pune, India. All the participants provided informed consents and utmost care was taken during the experimental procedure, according to the Declaration of Helsinki guidelines, 1975.
Patients: A total 102 patients with age group of 26 to 70 years, who were admitted in the Intensive Cardiac Care Unit (ICCU) with chest pain, were taken up for the study. The patients were diagnosed by physicians who were blinded to the results of the markers. The data included a history, physical examination, a serial 12-lead electrocardiogram and measurement of the cardiac markers.
Controls subjects: One hundred ten healthy age and sex matched individuals who didn’t have any evidence of ACS as per their clinical examination, were taken as the control subjects.
Exclusion criteria: The exclusion criteria were acute or chronic renal diseases, hepatic diseases, diabetes and heart diseases like congenital heart disease and diseases of the heart valves and the myocardium.
Approximately 2 ml blood was collected by venipuncture from the anticubital vein of the forearm of each subject in plain vaccutainers (Yucca Diagnostic) under aseptic conditions, within 6 hours after their admission in the ICCU and it was centrifuged for serum collection.
METHOD
(1) The determination of serum IMA by the albumin cobalt binding assay spectrophotometrically: This assay is based on the premise that myocardial ischaemia causes a change in the human serum albumin, that is demonstrated by a reduced exogenous cobalt (II) binding. The concentration of ischaemia modified serum albumin can be determined by the addition of a known amount of cobalt (II) to serum and the measurement of the unbound cobalt (II) by a colourimetric assay by using Dithiothereitol (DTT). The colour development with DTT was compared to a serum-cobalt blank without DTT and the results were reported in absorbance units (ABSU) [8].
(2) The determination of troponin I: TnI was estimated by a kinetic Immunofluroscence assay by using a Tosoh AIA-360 Immunoassay analyzer [9].
STATISTICAL ANALYSIS
The statistical analysis was carried out by using the SYSTAT software package for Windows. The Students “Z” test was applied for the statistical analysis and the results were expressed in mean± standard deviation (mean ±SD). p values of <0.05 for IMA and p values of <0.001 for TnI were considered to be statistically significant and highly significant respectively. The Receiver Operating Characteristic (ROC) curve analysis was performed and the area under the curve was determined for the assessment of the diagnostic performance of serum IMA and TnI in the all patients who were included in the study. The optimum cutoff values for the determination of serum IMA and TnI were selected from the ROC analysis. This optimum cutoff was used to dichotomously classify the positive or negative serum IMA and the TnI levels, and it was also used for calculating the diagnostic sensitivity and the specificity.
RESULTS
The baseline demographic and clinical characterizations of the patients and the healthy controls groups are given in [Table/Fig-1].
Baseline characteristics of all subjects: Values were expressed in mean with Standard Deviation (mean±SD),
| Variables | Controls (n=110) | ACS |
|---|
| Unstable Angina (n=43) | Myocardial Infarction (n=59) |
|---|
| Age in years | 40.1± 12.34 | 43.1± 13.01 | 48.8±14.56 |
| Gender (Men/Women) | 67/43 | 31/12 | 43/16 |
| Body Mass Index | 20.23±1.88 | 23.53±2.99 | 22.9±2.89 |
| IMA (ABSU) | 0.493±0.060 | 0.594±0.103* | 0.743±0.249* |
| TnI (ng/ml) | 0.0277±0.014 | 0.754±0.778** | 24.455±47.142** |
*Statistically significant (P<0.05)
**Statistically highly significant,(p<0.001)
n =numbers
As shown in [Table/Fig-1], the IMA levels were increased significantly (p<0.05) in the MI (0.743±0.249) and the UA (0.594±0.103) groups as compared to those in the controls (0.493±0.060).The mean values of serum TnI were significantly (P<0.001) higher in the MI (24.455±47.142) and the UA (0.754±0.778) groups as compared to those in the healthy controls (0.0277±0.014).
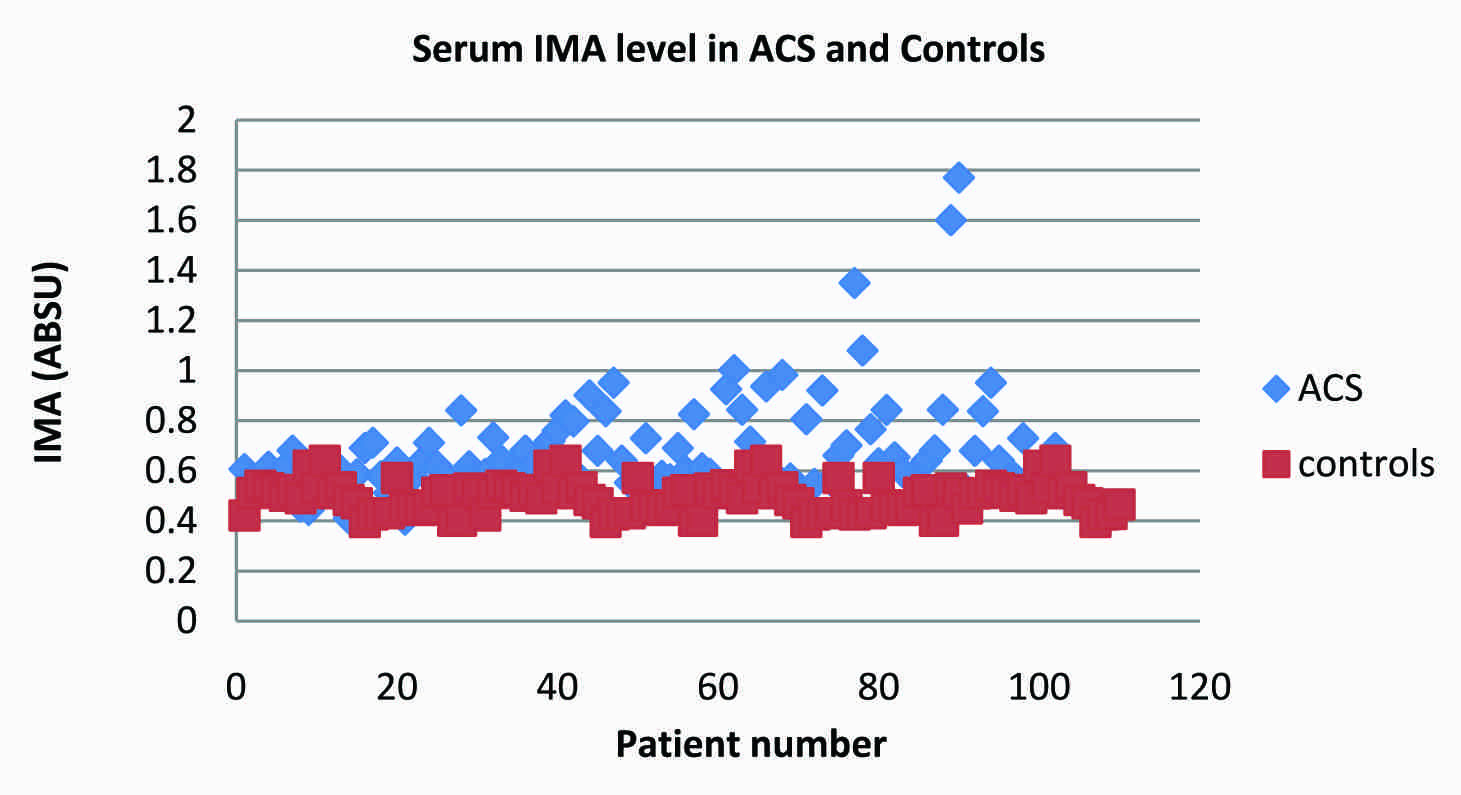
[Table/Fig-2] shows a scatter plot distribution of the results of the serum IMA in the control and the ACS groups. The optimum diagnostic cut off point which maximized the sensitivity and the specificity was determined to be 0.551 Absorption Units (ABSU), with a sensitivity of 88% and a specificity of 93%. The area under the curve for IMA was 0.90.
Scatter plot distribution of the results of serum IMA in controls and ACS groups
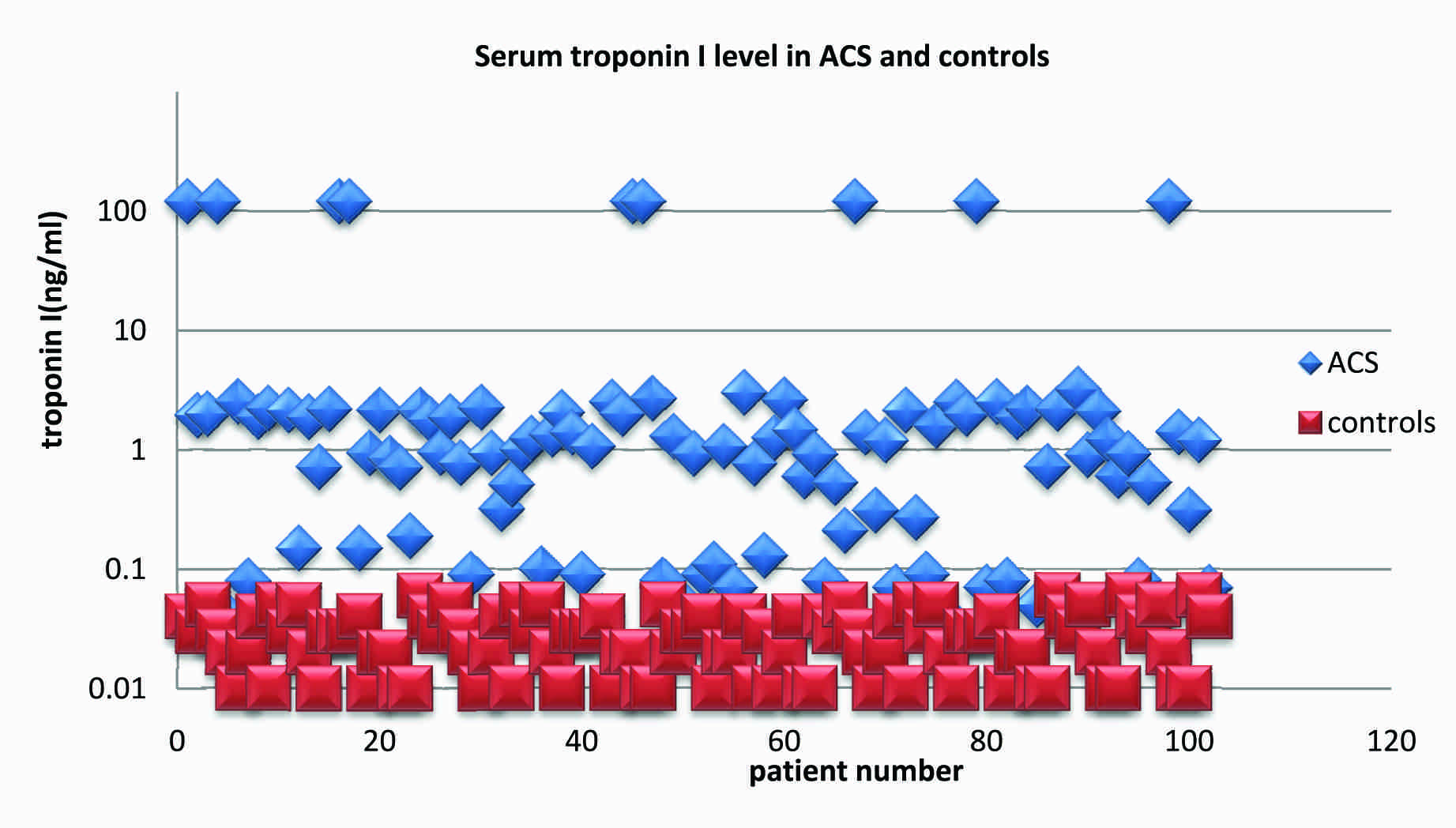
[Table/Fig-3] shows a scatter plot distribution of the results of serum TnI in the controls and the ACS groups. The optimum diagnostic cut off point which maximized the sensitivity and the specificity was determined to be 0.04ng/ml, with a sensitivity of 87% and a specificity of 75%.The area under curve for IMA was 0.638.
Scatter plot distribution of the results of serum troponin I in controls and ACS groups
The performanceof IMA and TnI alone and in combination for the diagnosis of ACS has been presented in [Table/Fig-4]. The sensitivity, specificity, positive predictive value and the negative predictive value were analyzed. The combined use of IMA and TnI significantly improved the sensitivity, specificity, positive predictive value and the negative predictive value to 96%, 93%, 93.33% and 96.26% respectively.
Clinical characteristics of diagnostic test for detection of ACS
| Variables | Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) |
|---|
| IMA | 88 | 93 | 92.78 | 89.56 |
| TnI | 87 | 75 | 77.11 | 88.29 |
| IMA and TnI | 96 | 93 | 93.33 | 96.26 |
DISCUSSION
The determination of biomarkers for myocardial injuries plays an important role in the diagnosis and the treatment of ACS. In the clinical practice, more attention has been paid to the determination of myocardial markers for the diagnosis of acute myocardial Ischaemia, stratification of the ACS risk and the differential diagnoses of reversible versus irreversible myocardial ischaemia and acute chest pain.
The quantitative or qualitative determination of cardiac TnI has been well accepted as a marker of the myocardial damage. However, most of the biomarkers of Acute Myocardial Infarction (AMI) are the products of myocardial necrosis and thus are detected typically at a later stage of the myocardial damage [10]. Therefore, rapidly detectable, highly sensitive markers would be desirable for myocardial ischaemia, to identify the patients with only ischaemia and those who are early in the course of an acute coronary syndrome without the evidence of any myocardial necrosis.
Prolonged ischaemia can lead to myocardial cell death and it is a pre-condition to an infarction. Therefore, the identification of myocardial ischaemia at the earliest stage is a must, for preventing the devastating consequences of the disease [4].
Ischaemia Modified Albumin has recently been evaluated as a new sensitive serum biomarker for cardiac ischaemia in contrast to the cardiac enzymes which are released when a cardiac necrosis occurs. During an acute ischaemic event, structural changes occur in the amino terminal of albumin, which rapidly reduces its capacity to bind to the transition metal ions and to generate a metabolic variant of the albumin, which is referred to as IMA [11–13] IMA has already been licensed by the US Food and Drug Administration for the diagnosis of suspected myocardial ischaemia [14]. Therefore, in our study, we examined the diagnostic performance of the IMA assay and the highly sensitive TnI assay for an early diagnosis of ACS at the time of the patients’ presentation to the Emergency Department.
The results of our study showed that the serum IMA level was significantly higher in the MI and the UA patients than in the healthy controls. The diagnostic appearance of serum IMA in ACS was maximum. The sensitivity and the specificity were 88% and 93% respectively. Our observations also supported the results of the studies of others [11,14,15] because ischaemic events could cause as much or more damage to serum albumin and the surrounding tissues as ischaemia itself. Different mechanisms have been postulated for the generation of IMA, early after cardiac ischaemia. Either ischaemia or a reperfusion may include hypoxia, acidosis, free radical damage, membrane energy-dependent sodium and calcium pump disruptions, and free iron and copper ion exposures [15,16]. Most of these conditions occur in vivo, within minutes after the onset of acute myocardial ischaemia.
It has also been hypothesized that in myocardial ischaemia, the release of fatty acids results in the binding of fatty acids to albumin, which leads to conformational changes in the albumin. This reduces the ability of albumin to bind to cobalt and hence, this accounts for the generation of IMA [17].
The blood levels of IMA patients rise promptly during myocardial ischaemia which is trigged by a primary reduction of the blood flow (supply ischaemia), as is seen in patients who undergo a percutaneous coronary intervention. They stay elevated for about 6 hours and return to the baseline line within 12 hours [18].
Shaoguing Juand et al., showed that the IMA concentration had increased significantly in the UA patients. In addition, IMA was negatively correlated with an abnormal Left Ventricular Ejection Fraction (LVEF), which could prove to be of clinical significance in the early diagnosis and the stratification of risk in patients with acute coronary syndromes [6].
The mean values of serum TnI were significantly higher in all the ACS patients as compared to those in the healthy controls. The diagnostic accuracy was highest with the TnI assay. The sensitivity and the specificity were 87% and 75%. Till Keller, et al., showed that with the use of the TnI assay on admission (with a cut off value of 0.04 ng/ml), the clinical sensitivity was 90.7% and the specificity was 90.2% [19]. The cardiac isoforms of troponins T and I have been used to evaluate the myocardial cell damage which is associated with UA and MI. Measurements of the cardiac specific contractile proteins, TnT or TnI were superior to the conventional measurements of other enzymes such as Creatine Kinase-MB and these were valid predictors of the adverse events in patients with ACS [20].
In the present study, the diagnostic performance of the IMA level in the ACS patients was greater as compared to that of the TnI assay. The sensitivity and the specificity of IMA were significantly greater than those of TnI. The combination of the IMA and the TnI results improved the sensitivity of the detection of ACS to 96%. Our results were in complete conformity to those of previous reports [10] which had revealed that a combination of the IMA, ECG and the TnI results had improved the sensitivity to 96% for the detection of ACS. Saif Anwaruddin et al., found that the combination of IMA, Myoglobin, CK-MB and TnI increased the sensitivity for detecting ischaemia to 97%, with a negative predictive value of 92% [21]. Bhagwan et al., reported a sensitivity of 88% and a specificity of 94% for the IMA assay, which were quite close to our results. They also reported an AUC under an ROC plot of 0.95 [7]. Therefore, there was the distinct advantage of measuring the combination of IMA and cardiac TroponinI on admission, in populations with non diagnostic electrocardiograms, to rule out a final diagnosis of AMI [22].
CONCLUSION
The core of this study lay in the fact that the measurements of the serum IMA levels could aid in a diagnosis of ACS in patients with ongoing ischaemic pain, who presented to the emergency department. IMA can be used as an independent point of care test or an additional parameter along with TnI, to boost the confidence of the clinicians in ruling out cardiac ischaemia. This combination seems to have clear potentials of time saving, an early intervention and a shortened stay in the emergency department.
*Statistically significant (P<0.05)
**Statistically highly significant,(p<0.001)
n =numbers