Infertility is a medical problem that affects a vast proportion of the world’s young population (10-15%); there is no agreement on the single definition. Irrespective of the definition which is being used, the inability to bear children seruminously impacts the psychosocial and the emotional lives of the couples who face this condition [1]. Infertility is defined as the inability to conceive even after a year of unprotected intercourse, or the inability to carry a child to term. Infertility is a growing problem among women and men [2]. It is of two types, primary infertility; it is a term which is used for a couple who have never achieved a pregnancy. The term, secondary infertility is used for a couple who had previously succeeded in achieving at least one pregnancy, even if it had ended in abortion [1]. There are many causes for the infertility in women.
The fallopian tubes may be blocked, which can prevent the egg from being fertilized and delivered to the uterus. Sexually transmitted infections or scarring from a previous surgery can cause such damage. The ovulation can be affected by hormonal imbalances, thyroid disorders, or chronic diseases such as diabetes [3]. Hyperprolactinaemia, the presence of abnormally high levels of prolactin in the blood, is the most common endocrine disorder of the hypothalamic-pituitary axis. Clinical and experimental studies have suggested a close relationship between the hypothalamic-pituitary-thyroid axis and the hypothalamic-pituitary-ovarian axis [4]. Hypothyroidism and hyperprolactinaemia are found to be closely interrelated. Hypothyroidism may cause a failure in ovulating regularly in women of the reproductive age group. Some of the women with high prolactin levels have been diagnosed with hypothyroidism, which is characterized by high levels of serum TSH [5]. The present study was conducted to determine the levels of serum prolactin in the primary infertile females who were sent for a hormonal evaluation, after excluding the tubal factors and the male factor infertility and to find its comparison with the thyroid stimulating hormone. This study was conducted to evaluate the levels of the prolactin hormone and the thyroid stimulating hormone in primary infertility women.
MATERIAL AND METHODS
Material
This was an observational study. The cases included diagnosed cases of 30 primary infertile females who underwent hormonal investigations in a special lab. There were 30 normal controls. The study was conducted at the Biochemistry Department which functioned at Grant Medical College and Sir J.J. Group of Hospitals, Byculla, Mumbai, India, from May 2011 to August 2011.
Inclusion criteria
The inclusion criteria for the selection of the cases were a diagnosis of primary infertility, age between 20-40 years and duration of marriage of more than one year. The relevant clinical history was taken from all the patients and the details were recorded in writing.
Exclusion criteria
The exclusion criteria that were adopted during the case selection were tubal factors, any congenital anomaly of the urogenital tract, or any obvious organic lesion. The patients with a history of thyroid disease or a previous thyroid surgery or those who were currently on thyroid medication were excluded from this study.
Method
Five millilitres of fasting venous samples were collected in the morning of the second day of the menstrual cycle for the serum biochemical analysis. The serum was separated and stored for further analysis. The hormones were estimated by using chemiluminiscence kits of serum prolactin, and serum TSH. The assay reliability was determined by the use of commercially derived control sera of low and high concentrations.
STATISTICL ANALYSIS
The statistical analysis was done by using the graph pad prism version 4. The data were analyzed by using the unpaired “t” test. A p-value of <0.05 was considered to be statistically significant.
RESULTS
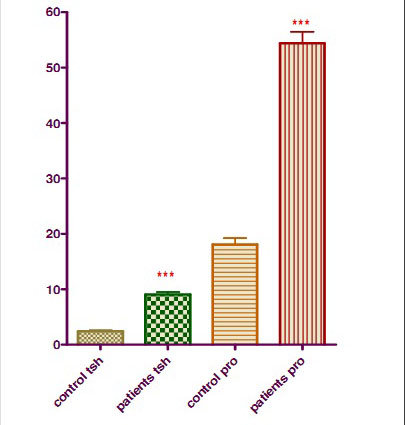
The serum Prolactin concentration was increased in the infertile group (54.38 ±11.34) as compared to that in the control group (18.14± 5.99) and it was found to be statistically highly significant (p<0.0001).
Similarly, the serum TSH in the infertile group was 9.05±2.64 and in the control group, it was 2.41±1.03, which was highly significant (p<0.0001) [Table/Fig-1].
Infertility and TSH, prolactin levels.
DISCUSSION
Hyperprolactinaemia is a common problem which is encountered in reproductive disorders [6]. The understanding that the prolactin hypersecretion not only caused galactorrhoea and amenorrhoea but also gonadal dysfunction and infertility, led to the need of prolactin estimations. Our study was carried out at the Biochemistry Department, Grant Medical College and Sir J.J. Group of Hospitals, Byculla, Mumbai, India. The serum Prolactin and TSH were measured by IMMULITE 1000 chemiluminescence immunoassays. The serum Prolactin concentration was increased in the primary infertile group (54.38 ±11.34) as compared to that in the control group (18.14± 5.99) and it was found to be statistically highly significant.
The serum TSH concentration was increased in the primary infertile group (9.05±2.64) as compared to that in the control group (2.41±1.03) and it was found to be statistically highly significant. (p<0.0001). Prolactin inhibits two hormones which are necessary for ovulation: the Follicle Stimulating Hormone (FSH) and the Gonadotropin Releasing Gormone (GnRH). When there are high levels of prolactin in the blood (a condition which is called hyperprolactinaemia), one will not ovulate and this will result in infertility. This anovulation can also cause irregular menstrual cycles [7]. Hyperprolactinaemia causes infertility because prolactin inhibits the GnRH secretion. When the GnRH secretion is low, the FSH and LH secretions are also low and so they do not stimulate the gamete production and the gonadal steroid synthesis [8–10].
Affia Tasneem stated that there was a higher prevalence of hyperprolactinaemia, together with a greater propensity for thyroid disorders in infertile subjects as compared to those in females with normal fertility [4]. This study stated that some of the women with high prolactin levels had been observed to have hypothyroidism which was characterized by high levels of serum TSH and low levels of T3 and T4. A subclinical hypothyroidism which was associated with hyperprolactinaemia was also reported in some cases. Clinical and experimental studies have suggested a close relationship between the Hypothalamic-Pituitary-Thyroid axis (HPT) and the Hypothalamic-Pituitary Ovarian axis (HPO) [11]. The specific thyroid hormone receptors at the ovarian level may regulate the reproductive function, as well as the influence of oestrogens at higher levels of the HPT axis seem to integrate the reciprocal relationship between these two major endocrine axes [11].
Lunenfeld et al., suspected that the patients with increased prolactin values were often hypothyroid [12]. Hyperprolactinaemia which results from a longstanding primary hypothyroidism has been implicated in ovulatory dysfunctions due to an inadequate corpus luteal progesterone secretion. Also, when the circulating prolactin levels are high, they lead to oligomenorrhoea or amenorrhoea [13]. Kumkum et al., stated that amenorrhoea occurs in hypothyroidism due to hyperprolactinaemia, which results from a defect in the positive feedback of oestrogen on LH, and because of the suppression of LH and FSH. It also mentioned that the prevalence of ovulatory dysfunction was one of the causes of female infertility. This study showed that a significant association between the abnormal menstrual patterns, as well as the anovulatory cycles, with hyperprolactinaemia in the infertile group 7.
K. Mohan and Mazher Sultana found that decreased levels of LH in the midcycle clearly indicated that there was a possibility of anovulation, which could result in infertility. According to this study, the elevated prolactin values in infertile women clearly showed that there was a mechanism which operated at the anterior pituitary level, which showed an abnormal distribution of FSH and LH, which could further explain the abnormal or delayed ovum maturation. This study showed lower concentrations of serum FSH and LH and higher concentrations of Prolactin in primary infertile women than in the control group [14].
Bohnet et al., and Matsuzaki et al., stated that hyperprolactinaemia was associated with a marked reduction in both the frequency and the amplitude of the LH pulses, which indirectly suggested that both the brain and the pituitary gland might be targets for prolactin. According to this study, the increase which was observed in prolactin may be the cause of the low oestrogen and progesterone concentrations in the infertile subjects, which showed that higher serum prolactin concentrations resulted in decreased serum LH and FSH levels in infertile women. This study also showed that there were lower concentrations of serum FSH and LH and higher concentrations of PRL in primary infertile women than in the control group [15–16].
According to Binita Goswami’s study, there is a significant association between the abnormal menstrual patterns, as well as the anovulatory cycles, with hyperprolactinaemia in infertile women. Amenorrhoea occurs in hypothyroidism due to hyperprolactinaemia which results from a defect in the positive feedback of oestrogen on LH, and because of LH and FSH suppression [17]. Hyperprolactinaemia adversely affects the fertility potential by impairing the pulsatile secretion of GnRH and hence interfering with the ovulation. This disorder has been implicated in menstrual and ovulatory dysfunctions like amenorrhoea, oligomenorrhoea, anovulation, an inadequate corpus luteal phase and galactorrhoea [17].
CONCLUSION
We found that there was an increase in the serum prolactin levels in infertile women as compared to those in the fertile ones in the control group. Similarly, we found a increase in the serum TSH levels in the infertile group as compared to those in the control group.
The incidence of hyperprolactinaemia in the primary infertile subjects in our study population was found to be significantly high. The relatively high occurrence of abnormal TSH levels in primary infertile women emphasized the importance of TSH screening in these women.