Oligodontia designates the congenital absence of six or more permanent teeth, excluding the third molars. Oligodontia of primary and permanent dentition is a rare observance. This case report describes the missing teeth in primary and permanent dentition of an 8 year old boy. Early diagnosis, and comprehensive treatment planning with good coordination and timing of the individual treatment phases are decisive for a successful treatment outcome.
INTRODUCTION
Tooth agenesis is a common developmental anomaly that appears in 2.2-10% of the general population (excluding agenesis of third molars). Congenital tooth agenesis can be either Hypodontia (agenesis of fewer than six teeth excluding third molars) or Oligodontia (agenesis of more than six teeth excluding third molars). Oligodontia is a rare condition that can occur in association with genetic syndromes, or as a non-syndromic isolated familial trait, or as a sporadic finding [1]. Although tooth agenesis is associated with more than 49 syndromes, several case reports describe nonsyndromic forms that are either sporadic or familial in nature, as reviewed by Gorlin et al., [2]. The prevalence of non-syndromic Oligodontia in Danish school children has been reported to be 0.16%, [3] a study conducted in Indore, India prevalence of Oligodontia was 0.36%. In addition to the loss of function and esthetic compromise, psychosocial development is an important concern in the oral rehabilitation of growing patients.
This case report presents a unique feature that oligodontia is present in both primary and permanent dentition and is not associated with any syndrome. This paper describes the teeth development of the child from 3 years, the course of treatment done during this period and the follow up evaluation.
CASE REPORT
A three year old male child of Indian origin reported to a private dental clinic with the chief complaint of missing primary teeth. Parents gave a positive history of consanguineous marriage with no associated prenatal, birth or medical condition. According to the mother, the child had difficulty in speaking and chewing because of absence of teeth. The child was examined by a paediatrician and growth assessment was done. The results showed that the child was apparently normal without any abnormal underlying systemic conditions. No significant abnormality revealed in extraoral examination. Intraoral examination revealed the presence of primary maxillary central incisors, maxillary primary first and second molars and mandibular primary first molars (Both Side). Salivary secretion was normal and the structure of teeth present was also normal. Panoramic radiograph revealed presence of Permanent maxillary central incisors, first permanent molars and mandibular permanent second molars [Table/Fig-1].
Orthopantomograph taken at 3 years old
As the child was not co-operative for the prosthetic management, he was called for periodical review once in 6 month was done and oral hygiene maintenance was reinforced. This also helped to desensitize the child to the dental environment. Parents were concerned about the unerruption of the teeth and its impact on his absence from school at six years of age. Intraoral examination revealed the presence of primary central incisors of maxilla, second primary molars in both mandible and maxilla, first permanent molars in both mandible and maxilla. The alveolus present was also very thin. Panoramic radiograph during this review [Table/Fig-2] revealed the formation of maxillary permanent incisors, mandibular first premolars including those of the ones in the maxillary left side and second premolars of the maxilla and right side of mandible. First premolars were seen bilaterally along with the tooth germ of the second molars in the right side. The teeth present in the oral cavity were of normal size, shape and color [Table/Fig-3]. After a thorough clinical and radiographic examination, the treatment option of a removable partial denture at this stage and later rehabilitation of teeth with osteointegrated implants was discussed with the parents. The child was familiarized with the materials to be used. Preliminary impressions were made using alginate (Zelgan, Dentsply, Indian). Special tray were fabricated using auto polymerizing acrylic resin (DPI-RR Cold acrylic resin, DPI, India), border molding was done using green stick compound (Pinnacle Tracing sticks, DPI, India). Then secondary impressions were made using zinc oxide eugenol impression paste (Impression paste, DPI, India). Record base were made jaw relation were registered. Teeth selection needs more attention as the commercially avaible would not satisfy the esthetic requirement in a pedo case. Teeth were trimmed to the approximate dimensions of the deciduous teeth and teeth setting were done. A removable partial denture was designed in such a way that it allows modification to be made as and the parents. The child was familiarized with the materials to be used. Preliminary impressions were made using alginate (Zelgan, Dentsply, Indian). Special tray were fabricated using auto polymerizing acrylic resin (DPI-RR Cold acrylic resin, DPI, India), border molding was done using green stick compound (Pinnacle Tracing sticks, DPI, India). Then secondary impressions were made using zinc oxide eugenol impression paste (Impression paste, DPI, India). Record base were made jaw relation were registered. Teeth selection needs more attention as the commercially avaible would not satisfy the esthetic requirement in a pedo case. Teeth were trimmed to the approximate dimensions of the deciduous teeth and teeth setting were done. A removable partial denture was designed in such a way that it allows modification to be made as and when necessary for the erupting tooth as well as providing reasonable aesthetic result, an acceptable masticatory function on complementing the lack of dentition and to be changed every 6month serving as interim prosthesis. Dentures were processed through compression molding using heat cure acrylic resin (DPI- heat cure acrylic resin, DPI, India) and inserted. The boy was taught the way to insert and remove the denture. He was instructed to speak and read loudly for some time in order to improve the phonation. The child was advised to have mashed potatoes, well cooked rice, biscuits and milk till he got accustomed to the denture.
Orthopantomograph taken at 6 years old

Intra oral photograph taken at 6 years old

Post insertion instructions on denture wear, functions of speech, mastication, hygiene and maintenance were given. The patient was recalled after 24 hrs of denture insertion for the post insertion checkup. Initially the patient was very depressed about the absence of teeth and reluctant in opening his mouth but after a week the patient was very comfortable with the denture [Table/Fig-4]. Periodic checkups were advised, approximately once in every three months to monitor the prognosis of the patient and modifications done as required.
Prosthesis with unerupted maxillary permanent right central incisor

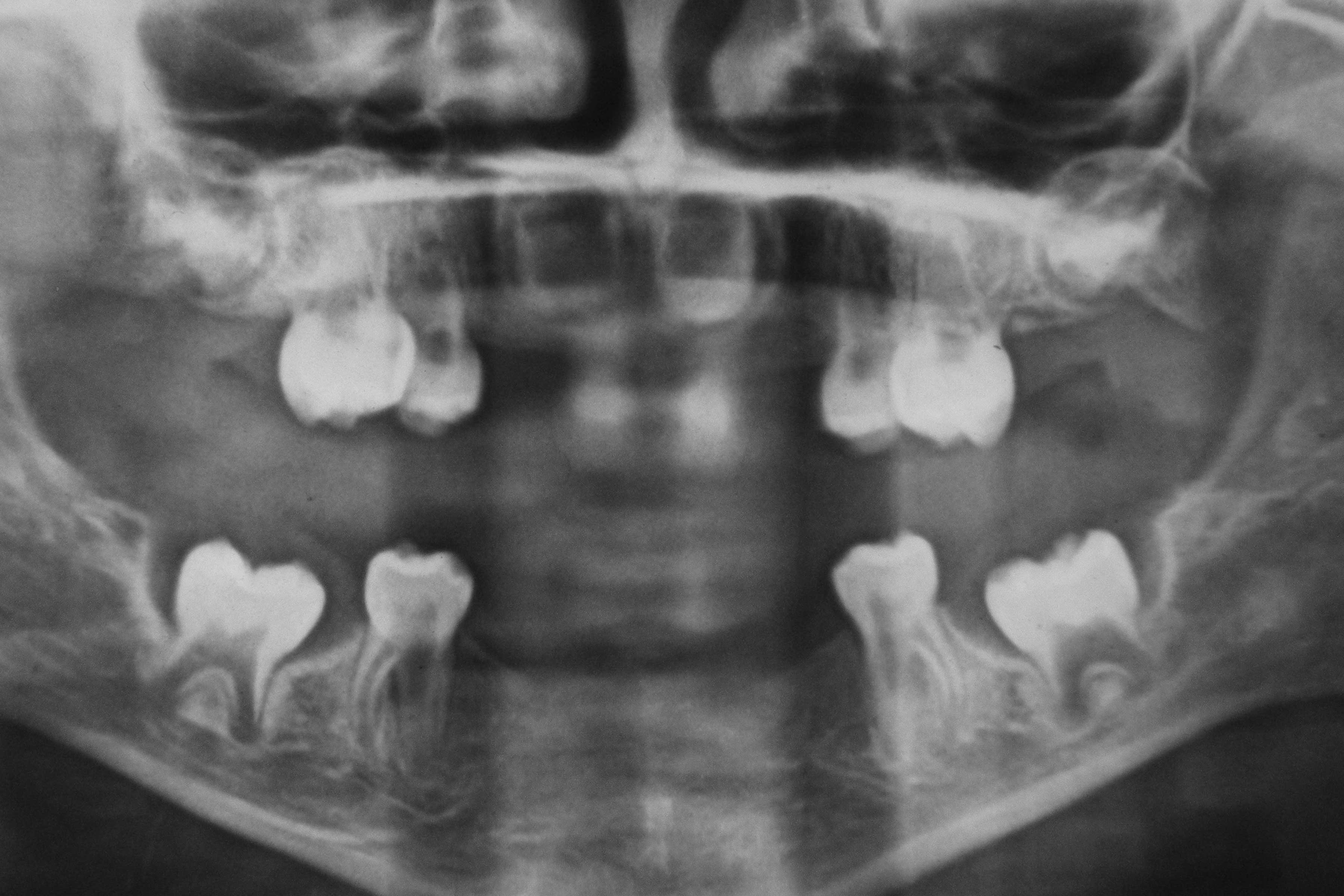
With the eruption of maxillary central incisors, at the age of 8, [Table/Fig-5] a new denture was constructed following the same procedure as done earlier [Table/Fig-6]. Panoramic radiograph at 6 years of age revealed the development of the maxillary permanent second molars [Table/Fig-7].
Intra oral photograph taken at 8 years old

Prosthesis with erupted maxillary permanent right central incisor

Orthopantomograph taken at 8 years old

At the present moment, we are following the eruption of still unerupted teeth, along with good hygienic measures and topical fluoride applications in every six months.
DISCUSSION
The case report presented in this paper is unique for the reason that oligodontia is exhibited both in primary and permanent dentition. Literature available is sparse with such type of cases. Oligodontia is a rare anomaly having an overall prevalence of 0.14% [4]. Oligodontia has a population prevalence of 0.3% in the permanent dentition and 0.5% to 0.9% in primary dentition [5]. Oligodontia may occur alone, as part of a syndrome, or in more serious systemic disturbances, for example in ectodermal dysplasia. If oligodontia is a part of a syndrome there are usually changes on the skin, nails, eyes, ears or skeleton [6]. On the contrary, the patient presented here does not have peg-shaped teeth, dry, scaly skin, straw-like hair, frontal bossing, wide spaced eyes or any problem with body-heat regulation. He appears to be a perfectly normal young child, with no known family history of missing teeth. The features in this patient also are not consistent with any specific forms of ectodermal dysplasia or syndrome [7]. Therefore this patient is diagnosed as having an isolated type of oligodontia. Isolated cases of Oligodontia have been reported without genetic mutations which have been inherited as an autosomal dominant trait with incomplete penetrance and variable expression. Mutations in MSX1 and PAX9 have been shown in families with nonsyndromic familial oligodontia [5,8]. Though oligodontia can be induced by environmental factors, the history of the child and the parents are not suggestive of any external influence. It is necessary to perform a gene analysis of the child to understand the mutation in a more definite manner.
In this case, there are ten missing primary teeth, which is a very rare occurrence. The radiographic evidence at the age of 3 shows only the presence of four permanent teeth. Venkataraghavan et al., [9] has reported absence of 18 missing primary teeth with the presence of developing permanent tooth buds with the defective formation of dentin, roots of permanent molars and incisors. A case of idiopathic oligodontia in primary dentition with permanent successors was reported by Shilpa et al., and Oshima et al., [10,11]. In the present case, there is absence of developing tooth germs of permanent lower incisors and permanent canines at seven years in the orthopanoromic radiograph. A similar finding has been observed by Bankole et al., [12] in a child of 9 years with non syndromic oligodontia the presence of primary canines and molars, permanent upper left canine and first molars. From a complete analysis of radiographs taken during the ages of 3 years, 6 years and 8 years, it is clear that there is delayed formation of tooth buds. As it has been reported earlier, the formation of premolars showed a varied formation and developing time, and the same can be observed in the present case. Therefore a long term follow up of this patient is required.
In the present case panoramic radiograph taken at the age of 8 showed the presence of permanent central incsiors, first premolars and the development of mandibular permanent second molar at an unusual site [Table/Fig-8]. This observation is in agreement with Rune who has stated that simultaneous with oligodontia are often different positional changes of the existing teeth, their morphology and size [13].
Profile photograph of the patient

A child with oligodontia should be under proper treatment planning, treatment and coordination of treatment and review appointing. Optimized conditions for the treatment of these patients include a fully integrated interdisciplinary team approach of pedodontist, orthodontist, oral maxilla-facial surgeon, and prosthodontist. The consequences of missing teeth include abnormal occlusions altered facial appearance which can cause psychological distress for some patients. For this reason, early diagnosis is important to prevent consequences of aesthetic and functional problems in the dentition. It is postulated that in cases where early prosthetic reconstruction is essential, the aim should be to provide the patient with temporary solutions which satisfy aesthetic and functional requirements and avoid unnecessary damage to tissue. A prosthodontic rehabilitation is fundamental in these situations, attempting to provide a functional and aesthetic solution that will allow the child as normal a life-style as possible, without damaging self-esteem or psychological development and ensuring that behaviour is unaffected. Therefore a removable partial denture which can be modified according to the eruption status of the teeth was provided to the child. The patient’s speech and masticatory function have improved greatly. However with the increased predictability of dental implants, the same treatment modalities have come under consideration for growing patients [14]. Patients with oligodontia may benefit from the use of dental implants in the mandibular anterior region, with restoration of function and improvement in psychosocial development, without waiting for the completion of growth to initiate treatment. Therefore placing of an implant supported denture is a treatment option in the near future for this child.
CONCLUSION
This case report exemplifies the rare occurrence of oligodontia in both primary and permanent dentition. The low prevalence of patients with oligodontia necessitates a certain degree of centralization of the more complicated cases and accumulation of knowledge and experience is to be obtained.
[1]. Kotsiomiti E, Kassa D, Kapari D, Oligodontia and associated characteristics: assessment in view of prosthodontic rehabilitationEur J Prosthodont Restor Dent 2007 Jun 15(2):55-60. [Google Scholar]
[2]. Gorlin RJ, Cohen MMJ, Levin LS, Syndromes of the head and neck 1990 3New YorkOxford University Press [Google Scholar]
[3]. Rolling S, Poulsen S, Oligodontia in Danish schoolchildrenActa Odontol Scand 2001 Apr 59(2):111-2. [Google Scholar]
[4]. Polder BJ, Van’t Hof MA, Van der Linden FP, Kuijpers-Jagtman AM, A meta-analysis of the prevalence of dental agenesis of permanent teethCommunity Dent Oral Epidemiol 2004 Jun 32(3):217-26. [Google Scholar]
[5]. Vastardis H, Karimbux N, Guthua SW, Seidman JG, Seidman CE, A human MSX1 homeodomain missense mutation causes selective tooth agenesisNat Genet 1996 Aug 13(4):417-21. [Google Scholar]
[6]. Schalk-van der Weide Y, Beemer FA, Faber JA, Bosman F, Symptomatology of patients with oligodontiaJ Oral Rehabil 1994 May 21(3):247-61. [Google Scholar]
[7]. Levin LS, Dental and oral abnormalities in selected ectodermal dysplasia syndromesBirth Defects Orig Artic Ser 1988 24(2):205-27. [Google Scholar]
[8]. Stockton DW, Das P, Goldenberg M, D’Souza RN, Patel PI, Mutation of PAX9 is associated with oligodontiaNat Genet [10.1038/71634] 2000 24(1):18-9. [Google Scholar]
[9]. Venkataraghavan K, Anantharaj A, Prasanna P, Sudhir R, Oligodontia in the primary dentition: report of a caseJ Dent Child (Chic) 2007 May-Aug 74(2):154-6. [Google Scholar]
[10]. Shilpa Thomas AM, Joshi JL, Idiopathic oligodontia in primary dentition: case report and review of literatureJ Clin Pediatr Dent 2007 Fall 32(1):65-7. [Google Scholar]
[11]. Ooshima T, Sugiyama K, Sobue S, Oligodontia in the primary dentition with permanent successors: report of caseASDC J Dent Child 1988 Jan-Feb 55(1):75-7. [Google Scholar]
[12]. Bankole OO, Iyun OI, Dosunmu OO, Non-syndromic oligodontia: a case reportWest Afr J Med 2010 Sep-Oct 29(5):356-8. [Google Scholar]
[13]. Rune B, Sarnas KV, Tooth size and tooth formation in children with advanced hypodontiaAngle Orthod 1974 Oct 44(4):316-21. [Google Scholar]
[14]. Giray B, Akca K, Iplikcioglu H, Akca E, Two-year follow-up of a patient with oligodontia treated with implant- and tooth-supported fixed partial dentures: a case reportInt J Oral Maxillofac Implants 2003 Nov-Dec 18(6):905-11. [Google Scholar]