A delayed Traumatic Diaphragmatic Hernia is a rare diagnosis. A 38 years old male presented to our emergency department with an acute bowel obstruction. He had a prior trauma laparotomy twenty year’s prior, which was reportedly negative. He required preoperative resuscitation for his severe hypokalaemic, hypochloraemic metabolic alkalosis, and acute renal failure. He underwent operative reduction of the incarcerated contents, and a primary permanent suture repair of the defect. The principles of the diagnosis of the delayed traumatic diaphragmatic hernia, and the operative repair of this entity have been reviewed.
Traumatic diaphragmatic hernia, Bowel obstruction, Delayed diagnosis, Occult injury
INTRODUCTION
Traumatic Diaphragmatic Hernias (TDHs) can result from both severe blunt, or penetrating traumas that traverse the diaphragm, and they are seen in 2-6% of the trauma cases [1]. They are a marker of serious injuries, and of blunt traumas that are associated with splenic ruptures, liver lacerations, pelvic fractures and thoracic aortic tears [2]. This is consistent with the severe forces in blunt trauma, that get distributed along the diaphragm, that cause an acute change in the intraabdominal pressure [3]. A majority of the TDHs are diagnosed and treated at the time of the injury; however, in approximately 10% of the cases, the injury is initially missed. In this rare case, a TDH was diagnosed one month or more after the injury and it was termed as a delayed TDH [4].
CASE REPORT
A 38 year old male presented to our emergency department with a 5 day history of nausea and vomiting. He could tolerate some liquids, but was vomiting after each solid meal. In addition, there were 48 hours of obstipation, constipation and oliguria. He had no past medical history, and had taken no medications. Twenty years prior, in another country, he had sustained a blunt trauma which was secondary to a bus accident, which had resulted in a reportedly negative trauma laparotomy and a left chest tube placement. The remainder of the history was negative.
His admission vitals were a temperature of 99.6 F, and he was haemodynamically stable. His physical examination revealed decreased breath sounds on the left side of the chest, and a nontender, nondistended abdomen with a healed midline scar.
His complete blood cell count was significant, as he had a white blood cell count of 12.6 K/μL, and a haematocrit of 54.6%. His biochemistry showed sodium 127 mEq/L, potassium - 3.3 mEq/L, chloride 73 mEq/L, bicarb 36 mEq/L, BUN 79 mg/dL, and creatinine 4.1 mg/dL. His amylase and lactic acid levels were both normal. The patient was aggressively resuscitated with normal saline for his acute renal failure and the hypokalaemic, hypochloraemic metabolic alkalosis. A nasogastric tube was placed on admission.
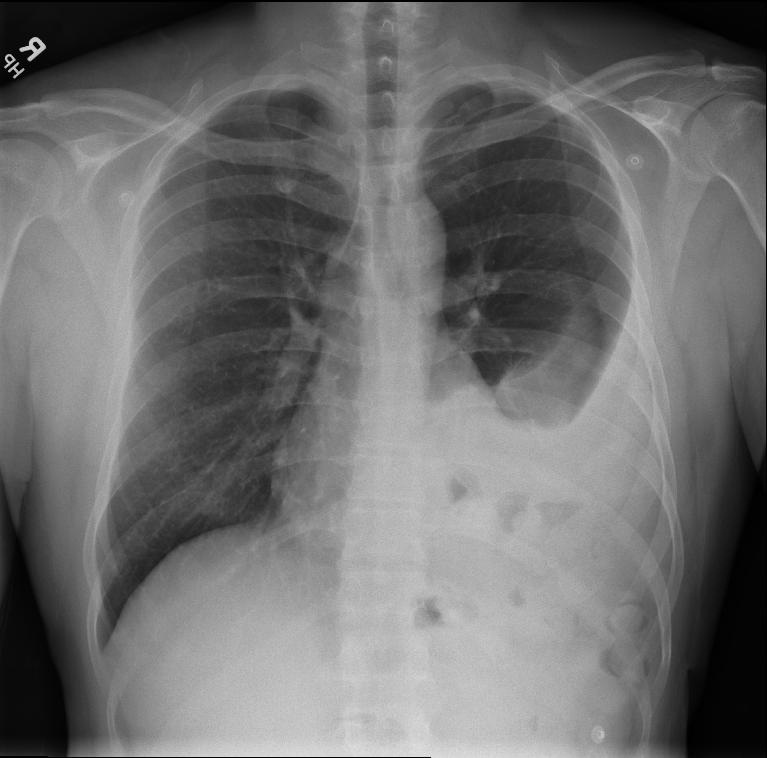
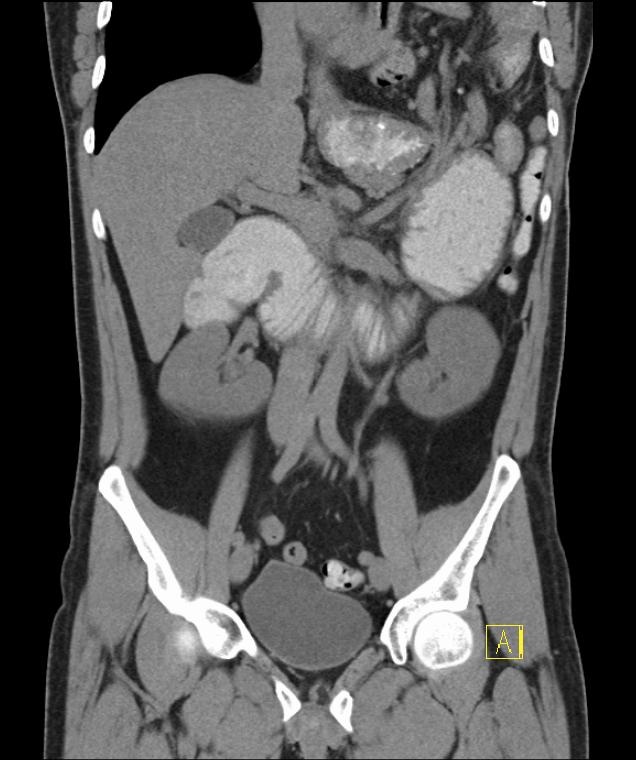
The initial chest X-ray had a large left pleural effusion [Table/Fig-1]. CT of the abdomen and pelvis found a large left diaphragmatic hernia with most of the transverse colon and nearly all of the jejunum and ileum herniating through the left diaphragm [Table/Fig-2]. The stomach and the duodenum were also markedly distended, with an abrupt transition point, where there was swirling of the mesentery.
Admission chest radiograph shows incarcerated bowel contents in the left lower chest. The gas present in the bowel loops helps to differentiate this from a large left pleural effusion
CT coronal view of the chest and abdomen with oral contrast shows the majority of the small bowel incarcerated in the left chest though the diaphragmatic defect
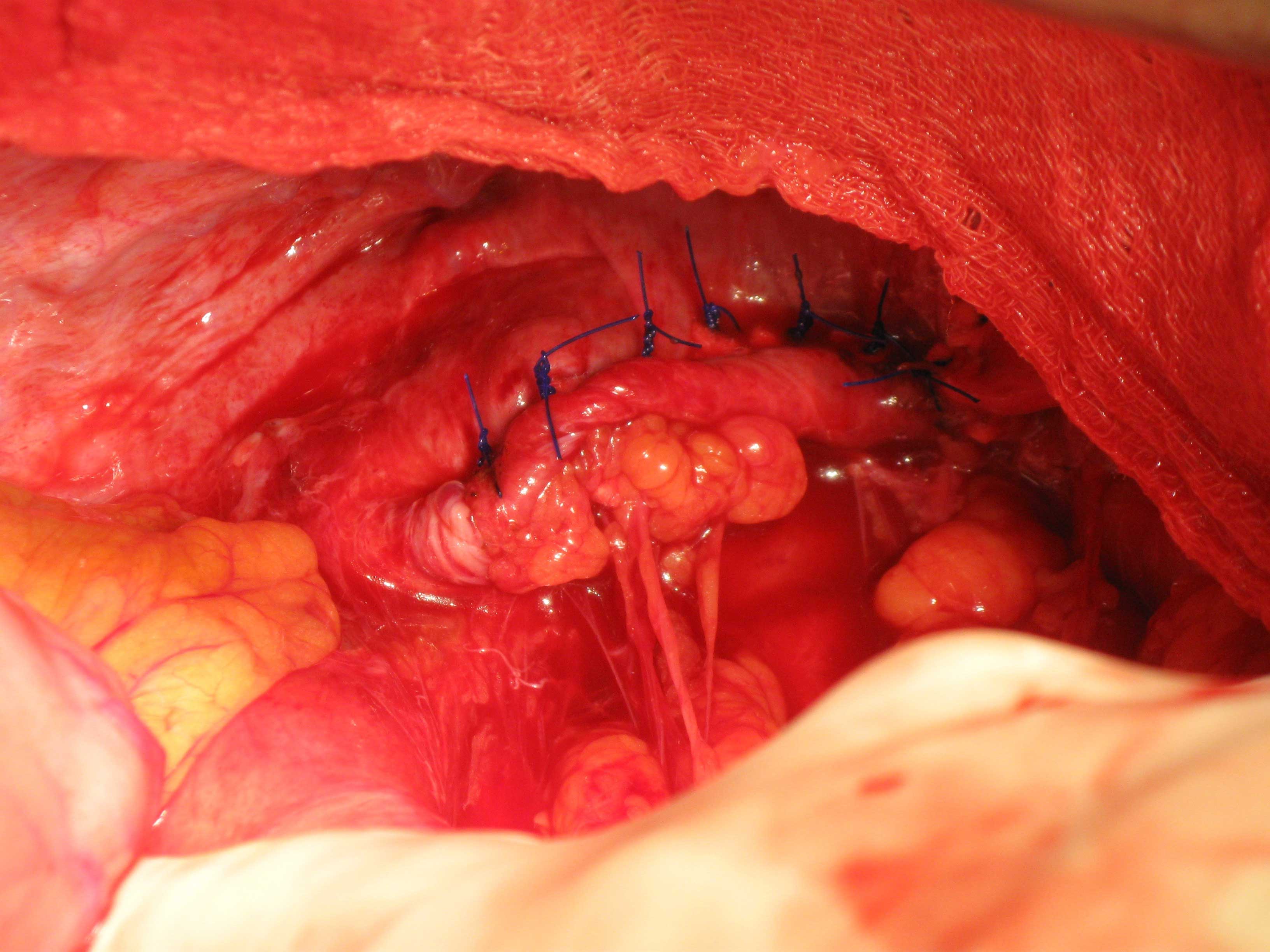
After 24 hours, with restoration of his intravascular volume, and normalization of his chemistries, he was brought to the operating room. Through an upper midline incision, the herniated contents were reduced, and a 4cm defect was identified in the central portion of the left hemidiaphragm, that was found to be chronic in nature. This was repaired by using interrupted 2-0 polypropylene sutures and pledgets [Table/Fig-3]. A left chest tube was placed at the conclusion of the procedure, which was removed on postoperative day #3, with no residual pneumothorax.
Intraoperative photograph of the left hemidiaphragm shows the 4 cm defect repaired with permanent suture and pledgets
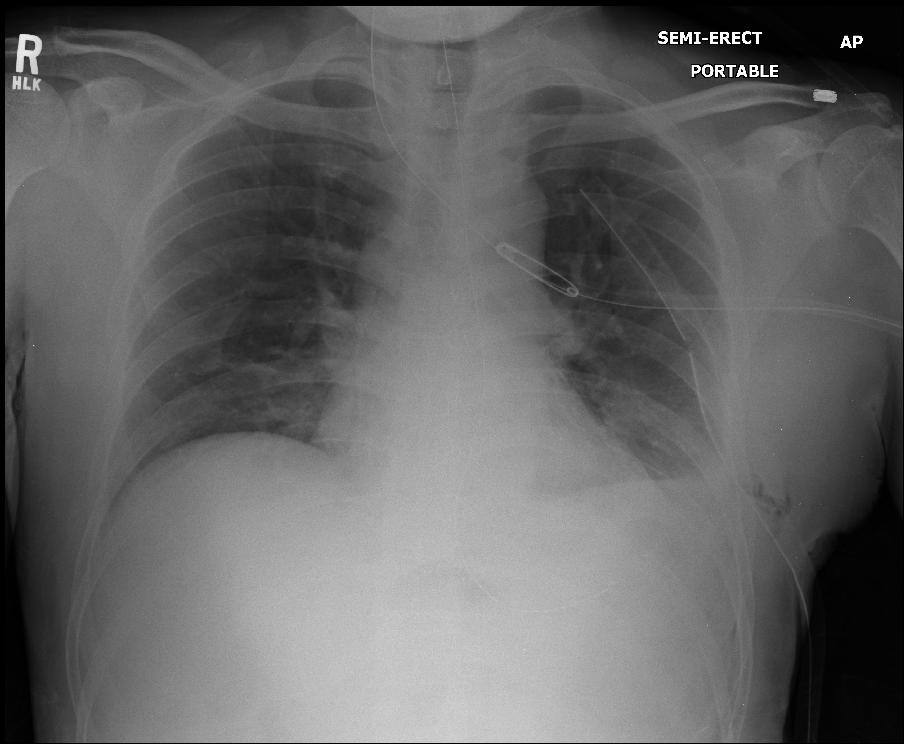
The patient made a full recovery, including the resolution of his acute renal failure [Table/Fig-4]. There were no postoperative complications, and an outpatient chest X-ray at 3 months postoperatively, showed the normal contour of the diaphragm and normal lung fields.
Immediate postoperative chest radiograph shows the chest tube appropriately placed with no pneumothorax. Note the small amount of subcutaneous emphysema present in the soft tissues of the left lateral chest wall
DISCUSSION
The diagnosis of a delayed TDH occurs when the patient becomes symptomatic, typically, after a delay of months to years. As the stomach and/or the colon herniate, the patient presents with acute dyspnoea, or as in our case, with gastrointestinal obstructive symptoms. Impressively, the diaphragmatic defect is typically asymptomatic before the acute presentation, and in some cases, for extended time intervals. While this is uncommon, a few cases of delayed TDH have presented decades later [5], with the longest interval being 50 years [6]. A majority of the cases of TDH are left sided [7,8].
A prompt diagnosis and an operative intervention form the cornerstone of the management, both for the TDHs and the delayed TDHs. This case illustrates that the diagnosis of TDH can be missed at the initial trauma presentation, even after an operative exploration, thus reinforcing the need to actively examine the diaphragm on all trauma laparotomies, to definitively rule out a TDH. In those cases that have an incarcerated bowel through the defect, the mortality rises to 80% when gangrene is present [9]. The radiologic workup consists of X-ray films, and computed tomographic scans of both the chest and the abdomen; in the more difficult cases, both will be required [10].
The principles of an operative repair include, reducing the incarcerated contents, removal of the hernia sac, drainage of the pleura and closure of the diaphragmatic defect. The diaphragmatic defects should be closed with permanent sutures, placed in an interrupted fashion, and reinforced with pledgets, so that they do not pull through the thin musculature of the diaphragm when they are tied in place. This is most commonly done via a laparotomy, although this has been approached via a thoracotomy, and also with laparoscopic and thoracoscopic techniques [5,11,12]. The postoperative complications include pneumothorax, atelectasis, recurrence of the diaphragmatic hernia, ileus, and intraabdominal adhesions.
The best method of a pleural drainage for preventing a pneumothorax remains a controversy, with the options including a tube thoracostomy drained to a pleuravac, or the intraoperative evacuation of air via a red rubber catheter. In this case, a tube thoracostomy was used, as the left lung had been chronically and significantly compressed due to the atelactatic changes, and was difficult to fully inflate intraoperatively. The author successfully used the catheter through the diaphragm technique to evacuate any remaining air, and removed at the conclusion of the repair on select cases when the lung has not been compressed, and the diaphragmatic defect smaller.
The clinicians need to be vigilant, to maintain a high index of suspicion for the diaphragmatic injuries, whether they are immediately posttraumatic, or even decades after the trauma. This case illustrates that an injury to the diaphragm can be missed, even at exploratory laparotomy, unless it is specifically sought out by palpating the diaphragms bilaterally at the time of any exploratory laparotomy for a trauma. While it is rare, a delayed TDH is an important cause of bowel obstruction, and it must be diagnosed early, so that an operative intervention can be done before gangrene of the bowel presents, with high mortality.
[1]. Nursal TZ, Ugurlu M, Kologlu M, Hamaloglu Tramautic diaphragmatic hernias: a report of 26 casesHernia 2001 5:25-29. [Google Scholar]
[2]. Meyers BF, McCabe CJ, Traumatic Diaphragmatic Hernia: Occult Marker of Serious InjuryAnnals of Surgery 1993 218:783-90. [Google Scholar]
[3]. Tang CT, Liu MY, Tang CT, Delayed presentation of a traumatic diaphragmatic herniaSigna Vitae 2011 6:53-55. [Google Scholar]
[4]. Shilpi G, Onkar S, Sumit S, Mathur RK, Delayed Presentation of Traumatic Diaphragmatic Hernia After 28 Years of Initial Trauma: Treated LaparoscopicallyThe Internet Journal of Surgery 2008 17(1) [Google Scholar]
[5]. Rashid F, Chakrabarty MM, Singh R, Iftikhar SY, A review on delayed presentation of diaphragmatic ruptureWorld Journal of Emergency Surgery 2009 4:32 [Google Scholar]
[6]. Singh S, Kalan MM, Moreyra CE, Buckman RF Jr, Diaphragmatic rupture presenting 50 years after the traumatic eventJournal of Trauma 2000 41:156-59. [Google Scholar]
[7]. Feliciano DV, Cruse PA, Mattox KL, Bitondo CG, Burch JM, Noon GP, Delayed diagnosis of injuries to the diaphragm after penetrating woundsJournal of Trauma 1988 28:1134-44. [Google Scholar]
[8]. Killeen KL, Mirvis SE, Shannmuganathan K, Helical CT of diaphragmatic rupture caused by blunt traumaAm J Roentgenol 1999 173:1611-16. [Google Scholar]
[9]. Hegarty MM, Bryer JV, Angorn IB, Baker LW, Delayed Presentation of Traumatic Diaphragmatic HerniaAnn Surg 1978 188:229-33. [Google Scholar]
[10]. Khreiss M, Karam J, Musallam KM, Al Harakeh AB, Nasr VG, Abi Saad GS, Distinctive Presentation of a Diaphragmatic Hernia 15 Years After A Traumatic InsultAnn Thoracic Surgery 2009 88:651-53. [Google Scholar]
[11]. Lomanto D, Poon PL, So JB, Sim EW, El Oakley R, Goh PM, Thoarcolaparoscopic repair of traumatic diaphragmatic hernia ruptureSurgical Endoscopy 2001 15:323 [Google Scholar]
[12]. Slim K, Bousquet J, Chipponi J, Laparoscopic repair of missed blunt diapragmatic rupture using a prosthesesSurgical Endoscopy 1998 12:1358-60. [Google Scholar]