A Case Report on A Myomectomy which was Done During A Caesarean Section
Shyamsundar1, Ratnamal M. Desai2, Pavitra3
1 Assistant Professor, Department of OBG,
2 Professor & HOD, Department of OBG, S.D.M medical college Sattur, Dharwar,
3 Post Graduate Student, Department of OBG, S.D.M Medical College Sattur, Dharawar, Karnataka, India.
NAME, ADRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shyamsundar, Assistant Professor, Department of OBG, No. 37/1, Ushakiran, I Main, I Cross, Rajajinagar, Sattur, Dharwar, Karnataka - 580025, India.
Phone: +91 9035942479
E-mail: sundershyamdoc82@gmail.com
Uterine myomas are being observed in pregnancy more frequently now than in the past, because many women are delaying child bearing till their late thirties, which is the time for the greatest risk of the myoma growth. Traditionally, obstetricians are trained to avoid myomectomies during caesarean sections as severe haemorrhages can occur, which may often necessitate hysterectomies. Pedunculated fibroids which can be easily removed are an exception. Here, we are reporting one case of a myomectomy which was done during a caesarean section.
Leiomyoma, Myomectomy, Pregnancy
INTRODUCTION
Depending on the trimester, the prevalence of uterine leiomyomas in pregnancy varies between 2.7 -10.7 % [1–3]. Traditionally, obstetricians are trained to avoid elective myomectomies during caesarean sections as haemorrhages can occur, which may often necessitate hysterectomies. The blood loss is usually severe as the size and the blood supply of the myomas are increased in pregnancy, especially at term [4].The risk of a haemorrhage is reportedly less with pedunculated fibroids as compared to that with the non pedunculated ones [5]. In most of the cases, it is wise to defer a myomectomy until the uterus has completely involuted, preferably till 6 months. Here, we are reporting one case of a myomectomy which was done during a caesarean section.
CASE REPORT
Mrs. N.T who was aged 40 years, was admitted to the labour room on 4/5/2012 with a diagnosis of G3P1L0 with 36 weeks of gestation, with a cephalic presentation in early labour. She had one, previous, fresh stillbirth 2 years back because of severe birth asphyxia. A USG which was done on 6/6/11 showed a posterior fundal fibroid of size 4.5x4.6cms.
Mrs. N.T who was aged 40 years, was admitted to the labour room on 4/5/2012 with a diagnosis of G3P1L0 with 36 weeks of gestation, with a cephalic presentation in early labour. She had one, previous, fresh stillbirth 2 years back because of severe birth asphyxia. A USG which was done on 6/6/11 showed a posterior fundal fibroid of size 4.5x4.6cms.
On examination, her PR was 84 beats/min, her BP was 120/80mm of hg and mild pallor was present. On per abdominal examination, the uterus was found to be 36 weeks in size, acting and relaxing, with a cephalic presentation. LOA with FHR was 130/min. On per vaginal examination, the cervix was found to be 25% effaced, 1cm dilated, vertex -3 station and with the membranes intact and the pelvis adequate. Her haemoglobin was 8.6gm% and her blood group was AB positive. HIV, HBSAG and VDRL were all non reactive and GST was 106mg/dl. The USGs which were done in the 2nd trimester and the 3rd trimester were normal.
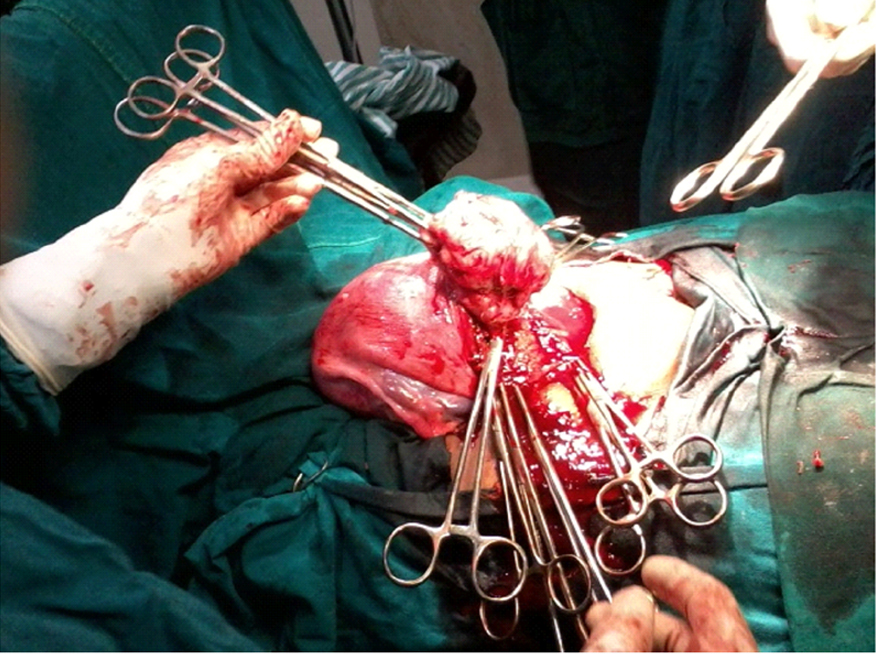
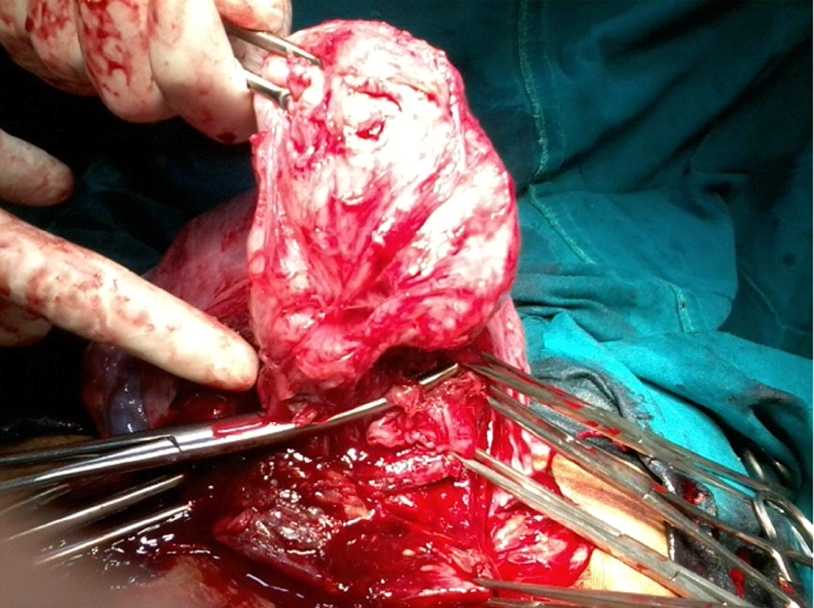
On 17/4/2012, she was taken for an elective Caesarean Section (CS) in view of her precious pregnancy. During the caesarean section, a submucous fibroid [Table/Fig-1] of size 6x7cms was noticed in the posterior wall of the uterus, at the incision site. After the extraction of a live female baby with a weight of 2kg, a decision was taken to perform a myomectomy and the myoma was enucleated [Table/Fig-2] with out much difficulty. A complete haemostasis was achieved.
Myoma in the posterior wall of uterus of size 6x7cms.
Enucleation of the myoma from the posterior wall of the uterus.
An oxytocin infusion was started after the delivery of the baby and it was continued for 12 hours. Broad spectrum antibiotics and analgesics were given in the post operative period. Her post operative period was uneventful and her post operative Hb was 8gm%. She did not require any blood transfusion. She was discharged on the 5th day and a USG which was done after 6 weeks, showed no fibroid.
DISCUSSION
Uterine myomas are being observed in pregnancy more frequently now than in the past, because many women are delaying child bearing till their late thirties, which is the time for the greatest risk of the myoma growth. Also, the use of ultrasonography has improved the diagnostic capability of detecting the small myomas and this has increased our knowledge on the myomas in pregnancy [6].
Ehigieba et al., reported 25 cases of caesarean myomectomies which were done in 12 women, which were without any complications [7]. They reported that anaemia was the most common form of morbidity. Kwawukume reported caesarean myomectomies which were done in 12 women. Enucleation of fibroids is technically easier in a gravid uterus, owing to the greater looseness of the capsule [8]. Li H et al., in a retrospective case control study which was done to assess the effectiveness of the safety, complications and the out comes of myomectomies which were done during CS, showed that it was an effective and a safe procedure with respect to the studied outcomes of the change in the haemoglobin levels, haemorrhage, blood transfusion, postoperative fever, duration of the operation and the length of the hospital stay [9].
Hassiakos D et al., reported that depending on the size and location of the myomas in pregnancy, the associated risks of the myomectomies with caesarean sections were similar to those of the isolated caesarean sections [10]. Kaymak O et al., in a retrospective case-control study which compared 40 patients who underwent myomectomies at the time of caesarean deliveries with the control group which consisted of 80 patients with myomas who had undergone caesarean deliveries alone, reported the incidences of haemorrhage to be 12.5% and 11.3 % in the two groups respectively. The difference was not significant [11]. Kadý Celal et al., also showed that myomectomies which were performed for fibroids in appropriate locations did not increase the post-operative bleeding or the maternal morbidity or mortality [12]. It was also reported that caesarean myomectomies would not significantly affect the future fertility and or the subsequent pregnancy outcome [13].
In this case, enucleation of the myoma was technically easy without an increase in amount of bleeding or the operative time. Also, the post-operative period was uneventful, which supported the fact that myomectomies which were done during caesarean sections were safe procedures.
[1]. Practice Committee of the American Society for Reproductive MedicineDefinitions of infertility and recurrent pregnancy lossFertil Steril 2008 89:1603 [Google Scholar]
[2]. Ansari AH, Kirkpatrick B, Recurrent pregnancy loss. An updateJ Reprod Med 1998 43:806 [Google Scholar]
[3]. Salat-Baroux J, [Recurrent spontaneous abortions]Reprod Nutr Dev 1988 28:1555 [Google Scholar]
[4]. Golan A, Langer R, Bukovsky I, Caspi E, Congenital anomalies of the müllerian systemFertil Steril 1989 51:747 [Google Scholar]
[5]. Daya S, Ward S, Burrows E, Progesterone profiles in luteal phase defect cycles and outcome of progesterone treatment in patients with recurrent spontaneous abortionAm J Obstet Gynecol 1988 158:225 [Google Scholar]
[6]. Davis JL, Ray-Mazumder S, Hobel CJ, Uterine leiomyomas in pregnancy: a prospective studyObstet Gynecol 1990 75:41-44. [Google Scholar]
[7]. Ehigiegba AE, Ande AB, Ojobo SI, Myomectomy during cesarean sectionInt J Gynaecol Obstet 2001 75:21-25. [Google Scholar]
[8]. Kwawukume EY, Myomectomy during cesarean sectionInt J Gynecol Obstet 2002 76:183-84. [Google Scholar]
[9]. Li H, Du J, Jin L, Shi Z, Liu M, Myomectomy during cesarean sectionObstetrical and Gynecological Survey 2009 64(6):363-64. [Google Scholar]
[10]. Hassiakos D, Christopoulos P, Vitoratos N, Xarchoulakou E, Vaggos G, Papadias K, Myomectomy during cesarean section: a safe procedure?Ann N Y Acad Sci 2006 Dec 1092:408-13. [Google Scholar]
[11]. Kaymak O, Ustunyurt E, Okyay RE, Kalyoncu S, Mollamahmutoglu L, Myomectomy during cesarean sectionInt J Gynaecol Obstet 2005 May 89(2):90-93. [Google Scholar]
[12]. Celal K, Hülya C, The evaluation of myomectomies performed during cesarean section in our clinicNiger Med J 2011 Jul 52(3):186-88. [Google Scholar]
[13]. Adesiyun AG, Ojabo A, Durosinlorun-Mohammed A, Fertility and obstetric outcome after caesarean myomectomyJ Obstet Gynaecol 2008 Oct 28(7):710-12. [Google Scholar]