An Idiopathic Membranous IVC Obstruction: Presenting as a Variant of the BCS
Amirtha Ganesh B.1, Ravi Cherian Mathew2, Ananathakrishnan N.3
1 Associate Professor, Department of Cardiology, Mahatma Gandhi Medical College and Research Institute, Pillaiyarkuppam, Puducherry-607402, India.
2 Post Graduate, Department of Cardiology, Mahatma Gandhi Medical College and Research Institute, Pillaiyarkuppam, Puducherry-607402, India.
3 Professor, Department of Surgery, Mahatma Gandhi Medical College and Research Institute, Pillaiyarkuppam, Puducherry-607402, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amirtha Ganesh B., Department of Cardiology Mahatma Gandhi Medical College and Research Institute, Pillaiyarkuppam, Puducherry-607402, India.
Phone: 9443461648
E-mail: amirtha2001@rediffmail.com
An Inferior Venacaval (IVC) lumen obstruction, whether it is partial or complete, is not a common phenomenon and it may be caused by the thrombosis or compression which may result from neoplastic or non neoplastic masses. There are cases which are idiopathic and which are typically referred to as membranous obstructions of the IVC. Here, we are presenting a 40 years old male with multiple tortuous veins over the abdomen, with non healing ulcers in the leg for 12 years, without ascites, who underwent a successful percutaneous transluminal balloon dilatation of the IVC membrane which was located above the hepatic veins, which resulted in a successful palliation of his symptoms.
Membranous IVC, Budd-chiari
INTRODUCTION
An Idiopathic Obstruction of the Inferior Vena Cava (IOIVC) is common in some parts of the world than in others. A series of such cases was described by the authors in Japanese institutions [1,2], where IOIVC was a more common cause of the Budd-Chiari Syndrome (BCS) than the more classical intrahepatic venous obstruction. Such lesions have found to be frequent in Chandigarh [3,4] though no data are available from other parts of India. The IOIVC is also relatively common in the black population of south Africa [5–7]. Simson [7] described a case series of 101 cases from Pretoria, with more occurrence among black patients. In the Indian [3,4,8] population, the lesions are generally situated within the hepatic portion of the IVC, below or at the diaphragmatic level. Many have associated the obstruction of one or both of the main hepatic veins, a finding which permits separation of the lesions of the IOIVC into eight different categories. The commonest form appears as a thin membrane which runs below an obliterated left hepatic vein, but above a patent right hepatic vein.
CASE REPORT
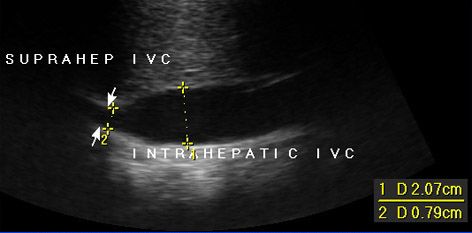
A 40 years old male smoker, who consumed alcohol twice a week, presented with multiple dilated tortuous veins [Table/Fig-1] over the abdomen, extensively over the central and the lateral abdomen and the back, which extended downwards into both the inguinal regions, which were associated with non healing ulcers on the right leg for the past 12 years. The flow in the dilated tortuous veins appeared to be below upward. He had NYHA class II dyspnoea. Upper GI endoscopy revealed gastric and oesophageal varices with gastric ulcers. An abdominal ultrasonography [Table/Fig-2] revealed narrowing of the suprahepatic inferior venacal lumen. No definite membrane could be visualized. A Computed Tomography (CT) of the abdomen which was done elsewhere, was not informative and it was suggestive of a long segment IVC occlusion, whose extent was not mentioned. An IVC angiogram showed a complete, blunt obstruction of the IVC, below the IVC-Right Atrial (RA) junction.
USG shows narrowing of the suprahepatic inferior vencal lumen
Dialated tortous veins seen over the abdomen pre-procedure (left) and post-procedure (right)

To know the extent of the obstruction, a simultaneous injection was given by keeping a pigtail in the IVC-RA junction from the upper limb, which revealed complete obstruction of the inferior vena cava by a membrane at 2-3 cm below the IVC right atrium junction. A Percutaneous Translumen Angioplasty (PTA) of the inferior – venacaval web was done. After crossing the membrane by using the stiff end of a 0.035 inch terumo guide wire, serial dilatation was done with peripheral balloons of different sizes and a final dilatations were done with a Jomiva balloon which was sized 26x40 mm [Table/Fig-3]. No significant residual stenosis was seen after the procedure and the collaterals were reduced significantly. But the oesophageal varices persisted. A repeat angiogram which was done after one month, revealed a good flow with no residual stenosis.
IVC angiogram shows complete obstruction of IVC below the IVC-RA junction (arrow), post dialatation revealed good flow with no residueal stenosis (right side)

DISCUSSION
Most of the reports on the membranous obstructions of the IVC, have originated from Japan, India, and south Africa [9], where this disease has a high incidence. Pathologically, this abnormality has been described as a web or a membrane which obstructs the IVC. Simpson [7] has described three types of membrane obstructions. In type I, the IVC is obstructed by a thin membrane, at the level of the entrance to the right atrium. In type 2, the segment of the IVC is absent and in type 3, there is complete obstruction of the IVC, which is secondary to the thrombosis. Clinically, these patients present in the third and fourth decades of life, with symptoms of portal hypertension. Yang and colleagues [9] reported good results with percutaneous transluminal balloon membranotomy. Dutta and colleagues [10] reported that hepatic vein thrombosis is a frequent complication of stent placement in IVC and patient need to be on long term antiplatelet therapy. After balloon dilatation if there is no significant residual stenosis then there is no need for stent placement. Srinivas and colleagues [11] reported that an endovascular management (balloon dilatation ± stenting) for membranous obstruction was safe, with good long-term patency rates. Sinha N and et al., [12] reported an incidental occurrence of IVC obstruction with Severe Rheumatic Mitral Stenosis for which they did single-staged balloon dilatation of the membranous obstruction. Bansal and et al., [13] using a Brockenbrough septal puncture needle relieved a membranous obstruction of IVC followed by deployment of a wall stent after series of balloon dilation which yield good results. In our case, the patient had portal hypertension, as evidenced by the grade III varices without ascites. Ultrasonography revealed that the hepatic veins were dilated but that the flow patterns were normal. There was no evidence of a hepatic venous obstruction. The portal venous flow was normal, with no obstruction.
CONCLUSION
The rarity in this case is its unusual presentation. Though we could not invasively measure the portal pressure, there was an evidence of portal hypertension – as was evidenced by the grade III oesophageal varices. But the patient did not have ascites and this was quite atypical and rare. Though the flow was completely restored after PTA, the oesophageal varices did not decrease even after one month, which could not be explained satisfactorily. Balloon dilatation with or without stent placement is a viable option for treating membranous obstructions of the IVC, which has shown good long term results.
[1]. Nakamura T, Nakamura S, Aikawa T, Suzuki O, Onodera A, Karoji N, Obstruction of the Inferior Vena Cava in the hepatic portion and hepatic veins. Report of eight cases and review of the Japanese literatureAngiology 1968 19:479-98. [Google Scholar]
[2]. Kimura C, Matsuda S, Koie H, Hirooka M, Membranous obstruction of the hepatic portion of the inferior vena cava: clinical study of nine casesSurg 1972 72:551-59. [Google Scholar]
[3]. Datta DV, Saha S, Singh SAK, Gupta BB, Aikat BK, Chugh KS, Chronic Budd- Chiari syndrome due to obstruction of the intrahepatic portion of the inferior vena cavaGut 1972 13:372-78. [Google Scholar]
[4]. Datta DV, Saha S, Singh SAK, Gupta BB, Aikat BK, Chugh KS, Chhuttani PN, Clincial spectrum of Budd- Chiari syndrome in Chandigarh with particular reference to obstruction of intrahepatic portion of the inferior vena cavaIndian J Med Res 1972 60:385-402. [Google Scholar]
[5]. Rogers MA, Chesler E, Du Plessis L, Joffe N, Joubert E, Membranous obstruction of the hepatic segments of the inferior vena cavaBr J Surg 1967 54:221-25. [Google Scholar]
[6]. Hodkinson HJ, Giraud RMA, Ou Tim L, Segal F, Cirrhosis of the liver associated with inferior vena cava and hepatocellular carcinoma in South AfricaGasteroenterol 1982 8:171-78. [Google Scholar]
[7]. Simson IW, Membranous obstruction of the inferior vena cava and hepatocellular carcinoma in South AfricaGastroenterol 1982 82:171-78. [Google Scholar]
[8]. Khurroo MS, Datta DV, Budd-Chiari syndrome following pregnancy. Report of 16 cases, with roentgenologic, hemodynamic and histologic studies of the hepatic outflow tractAm J Med 1980 68:113-21. [Google Scholar]
[9]. Yang XL, Cheng TO, Chen CR, Successful treatment by percutaneous balloon angioplasty of Budd-Chiari Syndrome caused by membranous obstruction of IVCJ Am Coll Cardiol 1996 28:1720-24. [Google Scholar]
[10]. Dutta U, Garg PK, Agarwal R, Dutta Gupta S, Prasad GA, Kaul U, Blocking of the hepatic vein outflow by neointima covering a wall stent across a membranous stenosis of the inferior vena cavaCardiovasc Intervent Radiol 1999 Nov-Dec 22(6):521-23. [Google Scholar]
[11]. Srinivas BC, Dattatreya PV, Srinivasa KH, Prabhavathi Manjunathan CN, Inferior vena cava obstruction: long term results of endovascular managementIndian Heart J 2012 Mar-Apr 64(2):162-69. [Google Scholar]
[12]. Sinha N, Kapoor A, Kumar S, Moorthy N, Singh V, Phadke RV, Sequential single-stage percutaneous balloon dilatation of an inferior vena cava obstruction with rheumatic mitral stenosisJ Heart Valve Dis 2011 Mar 20(2):237-39. [Google Scholar]
[13]. Bansal NO, Deshpande SS, Novel use of Brocken brough needle in relieving membranous obstruction of the inferior vena cavaHeart 2005 May 91(5):e38 [Google Scholar]