Extragenital Aggressive Angiomyxoma of the Axilla and the Chest Wall
Bhavna Nayal1, Lakshmi Rao2, Anuradha C.K Rao3, Swati Sharma4, Rajgopal Shenoy5
1 Assistant Professor, Department of Pathology, KMC, Manipal University, Manipal, India.
2 Professor, Department of Pathology, KMC, Manipal University, Manipal, India.
3 Professor, Department of Pathology, KMC, Manipal University, Manipal, India.
4 Associate Professor, Department of Pathology, KMC, Manipal University, Manipal, India.
5 Professor, Department of Surgery, KMC, Manipal University, Manipal, India.
NAME, ADRES, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bhavna Nayal, Assistant Professor, Department of Pathology, Kasturba Medical College, Manipal, Manipal University, India.
Phone: +919900411064
E-mail: bhavnayal17@gmail.com
Aggressive angiomyxomas are uncommon mesenchymal tumours which most often arise in the perineal and the pelvic regions in women. Extragenital aggressive angiomyxonas are extremely rare. We are reporting a young male with an aggressive angiomyxoma which involved the axillary region and extended into the anterior chest wall, which demonstrated its characteristic histomorphological features. The diagnosis was confirmed by immunohistochemistry. A careful histological examination, along with immunohistochemistry, aids in diagnosing this lesion and differentiating it from tumours which have similar histologies.
Aggressive angiomyxoma, Extragenital, Chest wall, Axilla
INTRODUCTION
An aggressive angiomyxoma is a rare myxoid soft tissue neoplasm which originates from fibroblasts/myofibroblasts which are composed of variably sized blood vessels, which range from thin walled capillaries to thick hyalinized blood vessels with a predominant myxoid stroma. These tumours primarily affect the pelvis and the perineum [1]. Only two cases of aggressive angiomyxomas which arose from the soft tissues of other sites have been reported in the literature [2,3]. This tumour has a marked preponderance for females who are in the reproductive age group [1,2]. Aggressive angiomyxomas have been reported in males to affect the inguinoscrotal region and the perineum, but the reports are very few in number [1,4,5]. To the best of our knowledge, this is the first case of extragenital aggressive angiomyxoma which involved the axilla and the anterior chest wall, which occurred in a male patient.
CASE REPORT
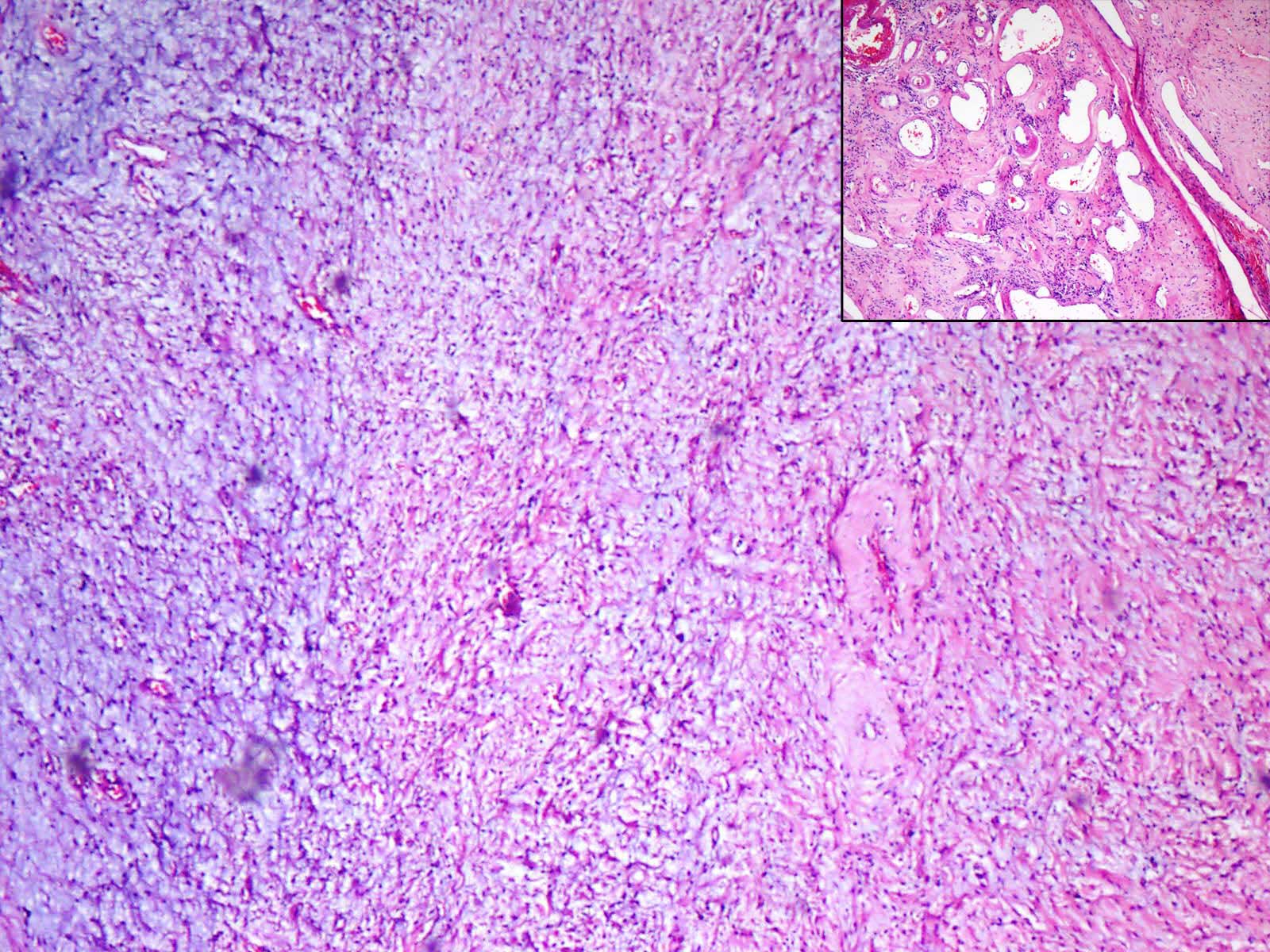
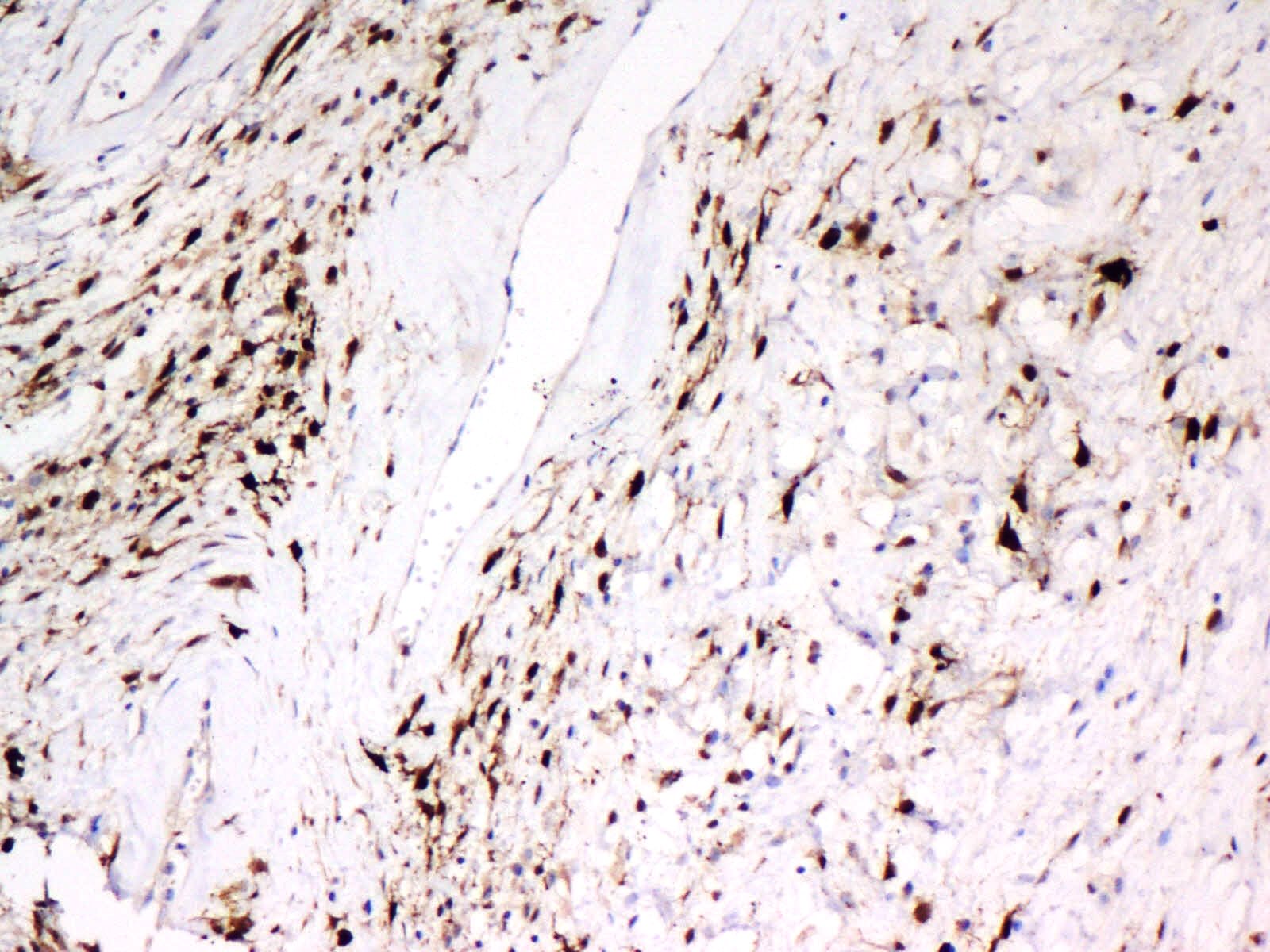
A 27-years-old male presented with a progressively enlarging mass in the left axillary region, which was there since 8 months. The initial size of the mass was 6x8 cm, which increased to 12x10cm and it extended into the anterior chest wall. There were no systemic complaints. On examination, the tumour mass was found to be firm and non tender and it involved the left axilla and the anterior chest wall. MRI revealed a relatively well defined mass with its anterior border overlapping the lateral border of the pectoralis major muscle, its posterior border extending beyond the mid axillary line, its superior border in the left axilla and its inferior border reaching up to the 5th rib, deep into the pectoralis major. No other lesions were detected in the abdomen or the pelvis. A clinical diagnosis of a schwannoma was given. The preoperative biopsy showed a hypocellular lesion with loosely dispersed spindle cells, with wavy buckled nuclei and hyalinized blood vessels. Based on the clinical suspicion and the histopathological features, a presumptive diagnosis of a schwannoma was rendered. A wide excision of the tumour was done and it was sent for a histopathological examination. The intraoperative findings revealed a soft, well circumscribed, lobulated mass which measured 12x7cm, which occupied the left axilla and the left side of the thorax. No adhesions to the adjacent muscle or the neurovascular bundle were detected grossly. The cut surface of the tumour showed a grey brown multinodular growth with gelatinous and myxoid areas [Table/Fig-1]. Histopathology revealed a myxohyaline vascular tumour which was composed of loose bundles of stellate to spindle cells with oval nuclei, which showed nuclear indentations. Few had prominent nuclei and a moderate eosinophilic cytoplasm which was characteristic of myofibroblasts. The surrounding collagenous stroma showed numerous thick walled blood vessels with vessel wall hyalinization. Few showed fibrin thrombi and few thin walled congested vessels. Extensive myxoid degeneration, oedema and eosinophilic, lymphoplasmacytic and mast cell infiltrates, along with extravasated RBCs, were also noted [Table/Fig-2]. The tumour showed infiltration into the adjacent skeletal muscle fibres. Immunohistochemistry revealed a diffuse smooth muscle actin [Table/Fig-3] and a focal S100 positivity. CD34 and the oestrogen receptor were negative. Based on the histopathological features and the immunohistochemistry, a diagnosis of an extragenital aggressive angiomyxoma was rendered. Six months post surgery, the patient remains asymptomatic, with no evidence of a recurrence.
A well circumscribed tumor. Inset: cut section shows grey brown multinodular growth with gelatinous and myxoid areas

Loose bundles of stellate to spindle cells in a myxoid stroma. Inset: collagenous stroma with numerous thick walled blood vessels and vessel wall hyalinization. (H&E, x200)
Spindle cells demonstrating smooth muscle actin immunoreactivity. (x400)
DISCUSSION
Angiomyxomas are rare tumours of mesenchymal origin. These lesions are classified as aggressive angiomyxomas, superficial angiomyxomas and angiomyofibroblastomas [2].
Aggressive Angiomyxoma (AAM) occurs predominantly in women, with a female to male ratio of approximately 6.6:1. These lesions are known to involve the soft tissue of the perineum and the pelvis in both males and females [1]. Two cases have been reported in regions other than these sites. The first was seen in an eight year old Japanese girl with AAM of the oral cavity [2]. The other case was a 48-years-old man with involvement of the supraclavicular fossa [3]. Both these cases showed no signs of recurrence or metastasis following the tumour excision. Our case was the first one which showed involvement the soft tissue of the axilla and the anterior chest wall.
Macroscopically, AAM is usually unencapsulated, bulky with a poor circumscription and with a glistening, gelatinous cut surface. However, encapsulated AAMs have also been reported [1,6, 7] .The present case was different, as the tumour was well circumscribed. The histopathological features include hypocellularity, hapahazardly arranged blood vessels of varying calibres, a myxoid stroma with collagen fibres and extravasated erythrocytes. AAMs tend to infiltrate the adjoining soft tissue [1]. Immunohistochemically, AAMs show positivity for vimentin, desmin and smooth muscle actin. The immunoreactivity of the Oestrogen (ER) and the Progesterone (PR) receptors have been described to be the most characteristic feature [1]. However, ER and PR negative AAMs have also been reported in the literature, particularly in male patients [5,8].
Aggressive angiomyxomas need to be differentiated microscopically from superficial angiomyxomas, fibroepithelial polyps, angiomyofibroblastomas, myxoid neurilemmomas, myxoid malignant fibrous histiocytomas, myxoid lipomatous tumours, myxoid leiomyomas and cellular angiofibromas. The clinicopathological features, along with the immunoreactivity, help in the diagnosis [1,3,5]. The presence of medium sized thick walled blood vessels, the deep location of the tumours and the absence of stromal neutrophils in this case, excluded the possibility of a syperficial angiomyxoma, a fibroepithelial polyp and an angiomyofibroblastoma. Since a majority of the tumour cells were S100 negative, a myxoid neurilemmoma was ruled out. A myxoid MFH shows the features of anaplasia, namely an increase in the mitosis or the presence of an abnormal mitosis or a nuclear atypia. These features were absent in the present case. The absence of significant proportions of smooth muscle or a lipomatosus component, excluded the possibility of myxoid lipomatous or smooth muscle tumours. Both cellular angiofibromas and aggressive angiomyxomas show medium to large sized hyalinized blood vessels with stromal mast cells; however, cellular angiofibromas are more cellular, more superficial in location with circumscribed margins and intralesional fat and they usually show positivity for CD34 [9].
The high mobility group A (HMGA2) gene rearrangements on chromosome 12q13-15 have been implicated in aggressive angiomyxomas. This transcription factor is present during the embryonic life and it is absent in the adult tissue. A strong HMGA [2] nuclear immunoreactivity aids in differentiating these tumours from other lesions, which include angiomyofibroblastomas and cellular angiofibromas [1].
The aggressive angiomyxomas are thought to be benign, locally infiltrative and non metastasizing [8]. However, two cases of metastases of AAMs which were reported, raised the possibility of the AAMs being classified as tumours of intermediate malignancies [1,10,11].
A complete surgical resection of the tumour is the first line of treatment. Owing to the infiltrating nature of AAMs, these are associated with a high recurrence. Hence, a postoperative follow up is necessary. Hormonal therapy with gonadotropin-releasing hormones has been used as an alternative treatment for the resolution of these tumours [1,5].
CONCLUSION
Aggressive angiomyxomas are rare slow growing tumours with a high recurrence rate and they occur almost exclusively in the pelvi-perineal region. The present case is unique in being located in the axilla and the anterior chest wall. A histopathological examination, combined with immunohistochemistry, help in distinguishing these lesions from the more commonly occurring similar entities, when they are located in sites other than the pelvis or the perineum.
[1]. Sutton BJ, Laudadio J, Aggressive angiomyxomaArch Pathol Lab Med 2012 136:217-221.PMID: 22288973 [Google Scholar]
[2]. Yamashita Y, Tokunaga O, Goto M, Aggressiveangiomyxoma of the oral floor: report of a caseJ Oral Maxillofac Surg 2004 Nov 62(11):1429-31.PMID: 15510368 [Google Scholar]
[3]. Pai CY, Nieh S, Lee JC, Lo CP, Lee HS, Aggressive angiomyxoma of supraclavicular fossa: a case reportHead Neck 2008 Jun 30(6):821-24.PMID: 18213718 [Google Scholar]
[4]. Tsang WY, Chan JK, Lee KC, Fisher C, Fletcher CD, Aggressive angiomyxoma. A report of four cases occurring in menAm J Surg Pathol 1992 Nov 16(1):1059-65.PMID: 1471726 [Google Scholar]
[5]. Kondo T, Aggressiveangiomyxoma in the inguinal region: a case reportJ Med Case Rep 2010 Dec 8 4:396PMID: 21143833 [Google Scholar]
[6]. Kaur A, Makhija PS, Vallikad E, Padmashree V, Indira HS, Multifocal aggressive angiomyxoma: a case reportJ Clin Pathol 2000 Oct 53(10):798-99.PMID: 11064679 [Google Scholar]
[7]. Adwan H, Patel B, Kamel D, Glazer G, A solitary encapsulated pelvic aggressive angiomyxomaAnn R Coll Surg Engl 2004 Nov 86(6):W1-W3.PMID: 16749950 [Google Scholar]
[8]. McCluggage WG, Patterson A, Maxwell P, Aggressive angiomyxoma of pelvic parts exhibits oestrogen and progesterone receptor positivityJ Clin Pathol 2000 Aug 53(8):603-5.PMID: 11002763 [Google Scholar]
[9]. Iwasa Y, Fletcher CD, Cellular angiofibroma: clinicopathologic and immunohistochemical analysis of 51 casesAm J Surg Pathol 2004 Nov 28(11):1426-35.PMID: 15489646 [Google Scholar]
[10]. Siassi RM, Papadopoulos T, Matzel KE, Metastasizing aggressive angiomyxomaN Engl J Med 1999 Dec 2 341(23):1772PMID: 10610453 [Google Scholar]
[11]. Blandamura S, Cruz J, Faure Vergara L, Machado Puerto I, Ninfo V, Aggressive angiomyxoma: a second case of metastasis with patient’s deathHum Pathol 2003 Oct 34(10):1072-74.PMID: 14608546 [Google Scholar]