Post Thyroidectomy Suture Granuloma: A Cytological Diagnosis
Anita P. Javalgi1, Surekha U. Arakeri2
1 Assistant Professor, Shri B M Patil Medical College, Bijapur, India.
2 Professor, Shri B M Patil Medical College, Bijapur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anita P. Javalgi, Department of Pathology, Bldeu’s Shri BM Patil Medical College, Sholapur Road, Bijapur, India.
Phone: 09739619068
E-mail: javalgianita@gmail.com
There are known post thyroidectomized complications, a suture granuloma being less frequent, with its late complication mimicking recurrent thyroid cancer.
A suture granuloma is a benign, granulomatous inflammatory reaction that occurs due to the use of non absorbable suture. It constitutes one of the late complications which altogether make up less than 2% of its incidence.
A suture granuloma is similar to a foreign body reaction and it usually develops slowly as a painless, palpable asymptomatic mass over the years. It mimics a cancer recurrence or a lymph node metastasis.
Here, we are reporting a case of a post thyroidectomy suture granuloma in a 46 years old lady who presented with a painless swelling in the lateral neck, with a past history of thyroidectomy 5 years back.
Suture granuloma, Post thyroidectomy, Cytological diagnosis
INTRODUCTION
A thyroidectomy is a very common surgical procedure which is performed world wide, even if the risks of lethal post operative complications prevented its evolution and diffusion until the beginning of the 20th century [1]. The major complications of a thyroidectomy are hypocalcaemia, recurrent laryngeal nerve injuries and post operative bleeding and its less frequent complications are surgical site infections, stitch sinuses, graulomas, keloids, wounds and chylous fistulas [2,3].
A suture granuloma is a benign granulomatous inflammatory lesion that may occur after a surgical intervention in which a non absorbable suture like silk, catgut had been used [4, 5].
Here, we are presenting a 46 years old lady who presented with a painless lateral neck swelling 5 years after a thyroidectomy, which was diagnosed as a suture granuloma on cytological studies.
CASE REPORT
A 45 yrs old female was referred to the cytology section for a swelling in the neck. The patient reported that she had detected a neck lump accidentally during a self examination one and a half months back. There was no history of pain or discomfort. Her past medical history revealed a total thyroidectomy which was done 5 years ago and she had no complaints since then, till the past 2 months back, when she had noticed this swelling. A local examination revealed a well defined, mobile, soft painless mass which measured 1.5x2cm, in front of neck, on the right side, just lateral to the hyoid bone. The swelling did not move on deglutition. All the routine haematological investigations were within normal limits. Sonography showed a hypoechoic lesion which measured 1.5x1.5cm. The case was referred for a fine needle aspiration study. There was no history of fever or any history which was suggestive of tuberculosis.
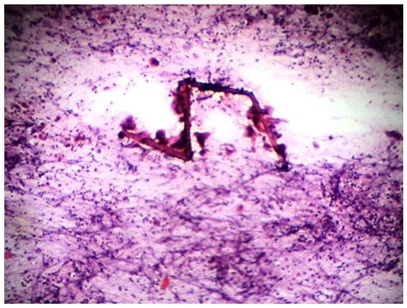
The cytological features showed a highly cellular smear which was comprised of inflammatory cells, predominantly neutrophils, aggregates of modified macrophages, foamy histiocytes, multinucleated Arakeriforeign body giant cells and few lymphocytes [Table/Fig-1 & 2]. Some of the giant cells consisted of fragments of suture material. The background showed necrotic debris, fibrinous material and fragments of suture material, which were surrounded by multinucleated giant cells [Table/Fig-3].
100 X H&E stain
Suture material surrounded by many multinucleated foreign body giant cells, background showing numerous mixed inflammatory cell infiltrate.
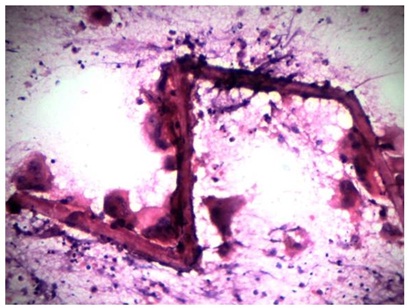
400 X H&E stain
High power view showing numerous multinucleated giant cells engulfing the suture material.
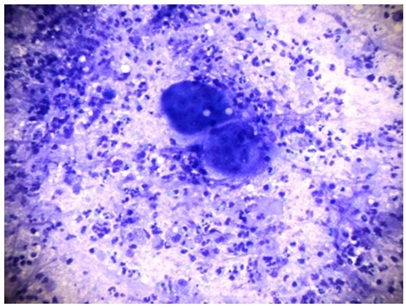
100X Geimsa stain
Numerous mixed inflammatory cells and multinucleared giant cells.
Special stains like PAS revealed no fungal filaments and the ZN staining for acid fast bacilli was negative. Hence, the features were those of a suture granuloma.
DISCUSSION
No surgical operation can be done without a risk of complications under any kind of anaesthesia. Nonetheless, the major complications of thyroid surgery like compressive haematomas, recurrent laryngeal nerve injuries and hypoparathyroidism, are still fearful complications [1].
The incidence of the complications like hypocalcaemia and recurrent laryngeal nerve injury varies from 0-14% and there is a less than 2% incidence of the minor complications like bleeding, seroma, infections and granulomatous lesions [1].
A suture granuloma is a rare complication of thyroid surgeries and it is known to occur after the use of non absorbable suture material deep within the skin [3]. The most common non absorbable suture material which is used is silk, which is a braided material which is formed from the protein fibres which are produced by the silk worm larvae. This silk suture is gradually degraded in the tissue over 2 years [4]. As compared to catgut, silk is cheap, it can be easily sterilized and it produces lesser tissue reactions and a stronger wound healing [4]. However, an inflammation along the suture line is sometimes noticeable immediately after the surgery, which causes suppuration and a sinus formation, but a delayed inflammatory reaction of the suture is rare [6, 7].
A suture granuloma can occur anywhere in the body after a variety of operations [5]. Eldridge et al., reported that the time lag between the operation and the formation of a suture granuloma varies upto 2 years, but there are other reports which have stated that the time interval varies from several months to years [5]. In the present (our) case, the time interval was 5 years.
The pathogenesis of a suture granuloma involves 2 steps; first, there is an initial reaction of the tissue which reflects the amount of injury which is inflicted by the passage of the needle and secondly, after the initial reaction subsides, the suture material causes a specific inflammatory reaction [8].
Eldridge et al., described severe complications which were caused by adverse reactions to sutures following thyroid surgeries. They reviewed their experience with 526 thyroid surgeries and found that 8% of the patients had severe neck infection postoperation, which was attributed to a silk suture reaction [9]. In a study which was done by Gritzmann et al., [2] and Rettenbacher et al., [3] they described a hypoechoic lesion with an echogenic central focus, in the neck swelling of a post thyroidectomy patient , that proved to be a foreign body granuloma which occurred from a suture and this had to be confirmed by doing a fine needle aspiration study.
The clinical presentation may vary from a classic inflammatory reaction with erythema, swelling, pain and finally, rejection of the suture material, to a chronic inflammatory reaction with a granuloma formation that may present as a solid, painless mass [4]. The traditional management of a suspected recurrence is fine needle aspiration for the cytological analysis and management of the therapy, based on the diagnosis [3]. A suture granuloma is clinically important because it mimics a cancer recurrence [4, 5].
CONCLUSION
A chronic granulomatous inflammation can occur as a palpable mass or masses in the operation bed of otherwise asymptomatic patients who had undergone thyroidectomies. Often, these patients are referred to undergo sonography and a fine needle biopsy study with a provisional differential diagnosis, with the highest possibility of a tumour recurrence. Hence, a cytological study remains the diagnostic tool for diagnosing a suture granuloma and if a successful diagnosis of a suture granuloma is made, removal of the suture can eradicate the inflammatory reaction and the further complications.
[1]. Lombardi CP, Raffaelli M, De Crea C, Tranini E, Oraganao L, Sollazzi L, Complications in thyroid surgeryMinerva Chir 2007 62:395-408. [Google Scholar]
[2]. Khanzada TW, Sammad A, Memon W, Kumar Basant, Post thyroidectomy complications: the Hyderbad experienceJ Ayub Med Coll. Abbottabad 2010 22(1):65-67. [Google Scholar]
[3]. Langer JE, Luster E, Horii S, Mandel SJ, Boloch ZW, chronic granulomatous lesions after thyroidectomy: imaging findingsAJR 2005 185:1350-54. [Google Scholar]
[4]. Kaprana A, foentanlabis NE, Karatzanis A, Velegrakis AG, Suture granuloma presenting as a lateral neck massOtorhinolarnyngologica – head and neck surgery 2012 48:36-40. [Google Scholar]
[5]. Chung YE, Kim EK, Kim MJ, Yun M, Hong SW, Suture granuloma mimicking recurrent thyroid carcinoma on ultrasonographyYonsei Med J 2006 47(5):748-51. [Google Scholar]
[6]. Katsunuma T, Likura Y, Delayed allergic reaction to silk sutures ;a case reportArerugi 1995 44:630-32. [Google Scholar]
[7]. Rossitch E Jr, Bullard DE, Oakes WJ, Delayed foreign body reaction to silk sutures in paediatric neurosurgical patientsChilds Nerv Syst 1987 3:375-78. [Google Scholar]
[8]. Postlethwait RW, Willigan DA, Ulin AW, Human tissue reaction to suturesAnn Surg 1975 181:144-50. [Google Scholar]
[9]. Eldridge PR, Wheeler MH, Stitch granulomata after thyroid surgeryBr J Surg 1987 74:62 [Google Scholar]