Marfan Syndrome (MFS) is an autosomal disease of the connective tissue which is characterized by skeletal anomalies and arachnodactyly [1]. Classic MFS occurs due to a mutation in the FBN1 gene, which codifies for the matrix protein fibrillin [1], although it is documented that 25% of the sporadic cases lead to de novo mutations in zones which are distant, several base pairs from this gene sequence [2].
Therefore, an early diagnosis of the pathology is essential, in order to establish a pharmacological therapy which is aimed at proSectiontecting the aortic wall and, in case of a grave mitral deficiency or a severe aneurismatic dilation of the ascending aorta, to plan a surgical correction [5–7]. The skeletal anomalies are the easiest signs to see [8–10] but oral manifestations, such as dental caries and periodontal diseases, although they are common in the general population, also have an increased incidence in patients with the Marfan Syndrome [11]. Thus, the aim of this work was to evaluate the oral phenotype in a group of paediatric aged patients with a clinical diagnosis of MFS and to analyze the association between these oral signs and other systemic alterations such as the cardiological and the orthopaedic characteristics.
MATERIALS AND METHODS
Subjects
On the basis of the inclusion criteria [Table/Fig-1] which were reviewed in 2010 in the Ghent Consensus [12], 32 paediatric subjects (18 males and 14 females; mean age: 10.47 years) with a clinical diagnosis of MFS were selected from our regional Marfan monitoring unit of the Tor Vergata University Hospital (Rome, Italy), in the period from May 2008 to September 2012. This study was conducted in accordance with the local ethics committee guidelines and written informed consents were obtained from each patient or his/her relatives.
Systemic score (revised Ghent nosology for the Marfan syndrome)
| Systemic Score |
|---|
| Characteristic | Score |
|---|
| Wrist and thumb sign | 3 |
| Wrist or thumb sign | 1 |
| Bulging chest | 2 |
| Hollow chest or thoracic asymmetry | 1 |
| Deformity of the rear foot | 2 |
| Flat foot | 1 |
| Spontaneous pneumothorax | 2 |
| Dural ectasia | 2 |
| Protrusion of the acetabulum | 2 |
| Reduction in the ratio between the length of the upper skeletal segment/lower skeletal segment and increased ratio between the length of the upper limb/lower limb and non grave scoliosis. | 1 |
| Scoliosis or thoracolumbar kyphosis | 1 |
| Reduced elbow extension | 1 |
| Cutaneous striae | 1 |
| Myopia > 3 diopters | 1 |
| Prolapse of the mitral valve (of all types) | 1 |
| Cranio-facial aspects (3/5) from: dolicocephaly, malar hypoplasia, retrognathia, enophthalmos and reduction of the palpebral rima | 1 |
Clinical Evaluation of the Oral Phenotype
The patients were subjected to cardio-surgical, paediatric, ophthalmological, genetic, orthopaedic and paediatric dentistry examinations. Moreover, all the patients were subjected to a radiological screening with Panoramic and Cephalometric X-Rays. The following clinical and radiographic parameters which are associated with MFS were evaluated:
Dolichocephaly (increased antero-posterior length of the head as compared to the width,a cephalic index of less than 76%) [13].
Retrognathia (posteriorly positioned lower jaw, which is set back from the plane of the face when viewed from the side but not from the front) [13].
Cross-bite (a malocclusion in which the mandibular teeth are in a buccal version to the maxillary teeth) [14].
Ogival palate (a condition where the palate is high and arched) [14].
Temporomandibular joint (TMJ) disorders (an articular click or a mandibular hyper-mobility) [14].
Malar hypoplasia (underdevelopment of the frontal process of the maxilla) [13].
Presence of dental caries.
Oral breathing,
STATISTCIAL ANALYSIS
Correlations between the oral and the cardiological and the orthopaedic observations were analyzed by using the chi square test for the nominal variables. A p-value of <0.05 was considered as statistically significant. The statistical analysis was performed by using the Statview software from the SAS Institute.
RESULTS
Clinical Characteristics
The percentage of the patients who had a first degree family member who was affected by MFS was 59.37% and 53.12% had a significant dilation of the ascending aorta, with a mean Z-score of 4.77. The percentage of the patients with a prolapse of one or both of the mitral valve leaflets was 71.87% and this alteration was significantly associated with the presence of the ascending aorta (p<0.05).
Orofacial Manifestations
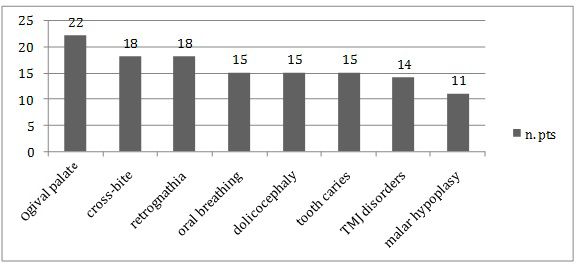
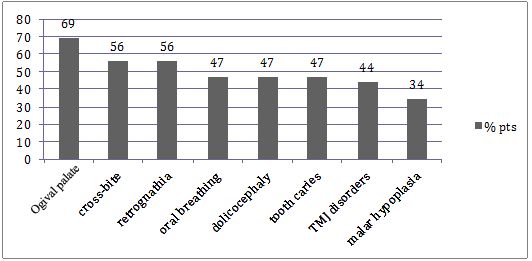
Number of oral manifestations associated in the observation sample is shown in [Table/Fig-2a]. On doing objective, cranial and dental X-ray examinations, 47% of the paediatric patients were found to present with dolicocephaly, 56% with retrognathia, 56% with cross-bite (mono- or bilateral), and 69% had evidence of an ogival palate. Moreover, 44% of them had temporomandibular joint disorders, 34% had malar hypoplasia and 47% had an experience of caries (dmft/DMFT >1) or they presented with oral breathing [Table/Fig-2b]. An absence of craniofacial anomalies was observed in 9.37% of the patients, while 15.63% presented with one or 2 alterations, 9.37% had 3 alterations and 12.5% had 4 to 8 alterations.
Number of oral manifestations associated in the observation sample
Percentages of oral manifestations associated in the observation sample
Correlations Between the Oral, Cardiological and the Orthopaedic Observations
The statistical analysis which was performed by doing the chi square test for the nominal variables, showed a significant correlation between the patients with cross-bite and an Aortic Z-score of >3 (p<0.01) [Table/Fig-3]. Moreover, the correlation between the patients with cross bite, an ogival palate and myopia of >3 diopters with an Aortic Z-score, was also significant (P<0.01). Similarly, a significant correlation was found with retrognathia, malar hypoplasia, cross bite, oral respiration and an Aortic Z-score (P<0.05) [Table/Fig-3].
Significant correlations between oral signs and cardiological and orthopedic characteristics
| Oral Characteristic | Other Characteristic of the Syndrome | P – Value |
|---|
| Cross-bite | Z – score > 3 | < 0.01 |
| Cross bite + ogival palate | Z – score > 3 + myopia>3 diopters | < 0.01 |
| Cross bite + oral respiration + malar hypoplasia + retrognathia | Hyperlaxity of ligaments | < 0.05 |
| Cross bite or oral respiration or malar hypoplasia or retrognathia | Scoliosis | < 0.05 |
The association of retrognathia, malar hypoplasia, cross bite and oral respiration with hyperlaxity of the ligaments was also statistically significant (P<0.05). The association of any of these defects with scoliosis was also significant (P<0.05) [Table/Fig-3].
DISCUSSION
Although oro-facial defects such as dental caries and periodontal diseases have an increased incidence in patients with the Marfan Syndrome [11], there is a lack of information on the association of these defects with other systemic alterations. Thus, in this study, we evaluated the oro-facial defects in a group of paediatric patients with a clinical diagnosis of MFS and analyzed their association with other systemic defects, such as cardiological and orthopaedic alterations.
Our data showed a significant correlation between the aortic dilation (Aortic Z-score value) and multiple oral defects which included retrognathia, malar hypoplasia, cross bite, oral respiration and an ogival palate. Moreover, a significant correlation between the aortic dilation and certain defects which presented simultaneously (cross bite, ogival palate and myopia of > 3 diopters), was also found. An association of retrognathia, malar hypoplasia, cross bite and oral respiration with hyperlaxity of the ligaments and scoliosis was also observed.
Paediatric population still suffers today from a diagnostic delay of the MFS syndrome because the symptoms may not be evident, especially during growth. Our data suggest that dentists should be more involved in a multidisciplinary approach, to provide an early diagnosis of MFS at the paediatric ages. This idea is supported by many experimental observations. A mono- or a bi-lateral cross-bite is a malocclusion which is regarded as a primary or a secondary condition which is associated with bad habits and which affects 8 to 23% of the paediatric population [15,16]. In our cohort of paediatric patients, cross-bite was present in 56% of the cases, which suggested that this characteristic was 2.5 to 7 times more frequent in the MFS patients. A maxillary contraction and an ogival palate are also important factors from an orthodontic point of view, as they may determine a posterior cross-bite and a dental crowding. A dolichofacial aspect and a Class II skeletal malocclusion are often observed in patients with MFS [17]. Westling and colleagues [18] studied 76 patients with the MFS syndrome and detected a collapse of the dental arches with crowding and augmented over-jets in 70% of them. The high occurrence of ogival palates in MFS patients has not yet been explained, although their association with either a restriction or an increased resistance in the nasal airways (NARs) has been hypothesized. In fact, elevated NARs can cause an obstructive apnoea in the sleep of Marfan patients [19]. The consequent compensatory oral respiration which is caused by a nasal obstruction may alter the physiological posture of the head, thus influencing the facial development.
As for an incidence of caries and periodontal disease, De Coster and colleagues [20] reported that, in a cohort of 23 patients with MFS with a mean age of 26.17 years, a majority of them presented a higher risk of caries which was correlated with an elevated difficulty of the treatment due to the presence of hypoplasia of the enamel, radical malformations and shape anomalies in the pulp chamber. In the same study, they highlighted that periodontal diseases were more frequent and severe in these patients. However, in our group of patients, we reported a 47% prevalence of dental caries, which is in line with the data of the general paediatric population in Italy. Moreover, no clinically or radiologically visible signs of periodontal disease were found. Thus, our findings suggest that the data which has been reported in the literature on a higher prevalence of caries and periodontal disease in MFS patients, is probably related to the adult rather than the paediatric age group.
CONCLUSIONS
In conclusion, our data suggest that some oro-facial defects are associated with other systemic alterations in children who are affected by MFS. The present findings suggest that an evaluation of the oro-facial characteristics, when they are accompanied by systemic symptoms which are assessed by other specialists (i.e. myopia exceeding 3 diopters, hyperlaxity of the ligaments and scoliosis), may provide a useful criterion to the paediatric dentists to refer the patient for a cardiological evaluation with the aim of making an earlier MFS diagnosis.