The Knowledge, Attitude and the Perception of Prescribers on the Rational Use of Antibiotics and the Need for an Antibiotic Policy–A Cross Sectional Survey in a Tertiary Care Hospital
Ambili Remesh1, A.M Gayathri2, Rohit Singh3, K.G. Retnavally4
1 Associate Professor, Department of Pharmacology & Therapeutics, Dr. Somervell Memorial CSI Medical College, Karakonam,Trivandrum, Kerala, India.
2 Final M.B.B.S Student, Department of Pharmacology & Therapeutics, Dr. Somervell Memorial CSI Medical College, Karakonam,Trivandrum, Kerala, India.
3 Assistant Professor, Department of Pharmacology & Therapeutics, Somervell Memorial CSI Medical College, Karakonam,Trivandrum, Kerala, India.
4 Professor & Head, Department of Pharmacology & Therapeutics, Dr. Somervell Memorial CSI Medical College, Karakonam,Trivandrum, Kerala, India.
NAME, ADDRES, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ambili Remesh, Associate Professor, Department of Pharmacology & Therapeutics, Dr. Somervell Memorial CSI Medical College, Karakonam,Trivandrum, Kerala, India.
Phone: 9497011358 E-Mail: ambiliremesh@yahoo.com
Background: Antibiotics are prescribed frequently and there is always an overuse with a risk of resistance and increasing costs. Rational drug prescribing is essential for minimizing the health care costs and for reducing the resistance. The implementation of a strict antibiotic policy by all the health care institutes is being made mandatory nowadays. An improving awareness among the prescribers which can be created through educational interventions, can promote the rational use of antibiotics. Hence, we considered it worthwhile to study the knowledge, attitude and the perception of the practitioners towards a rational antibiotic use.
Materials and Methods: All the registered practitioners who were working in the hospital setting and were willing to give written informed consents, were enrolled in the study. All the participants who were enrolled in the study during a one month period, had to fill up a predesigned, structured and validated questionnaire which was used to assess the knowledge, attitude and the perception among physicians towards the rational use of antibiotics.
Results: About 65% of the participants who provided complete information in the questionnaire, were included in analysis. Among them, more than 50 % agreed on the existence of an essential drug list, on the knowledge about new antibiotics and on prescribing antibiotics rationally and on the interpretation of the culture and the sensitivity results. A majority strongly agreed that they ensured that their patients completed the course, that they provided counselling and that they took special interest in the proper use of antibiotics. There was a consensus on the overuse, issues of resistance, and on the input from fellow colleagues.
Conclusion: The participants in our study had knowledge about the rational use of antibiotics, an attitude to prescribe drugs as per the essential drug list and a perception that antibiotics were being overused and that rational drug prescribing had an important role in the antibiotic resistance.
Antibiotic policy, Rational drug use, Drug resistance
INTRODUCTION
Antibiotics are among the most frequently prescribed drugs worldwide [1,2]. They are used to treat both life threatening and trivial infections [3]. The overuse and/ or misuse of antibiotics can lead to significant consequences, like increased costs, bacterial resistance, therapeutic failures, drug toxicities and drug interactions [1]. There have been reports on high incidences of infectious diseases due to a high usage of antibiotics and bacterial resistance from the low and middle income countries [3]. Overcrowding, poor sanitation and a warm-humid climate in these countries, results in the rapid spread of resistant bacteria [3]. A global proportion crisis of infectious diseases is threatening the health and the life expectancy. In children and young adults, infectious diseases are the world’s biggest killers, causing more than 13 million deaths per year. Ninety percent of the deaths are due to six deadly infectious diseases, namely; pneumonia, tuberculosis, diarrhoea, malaria and measles [4,5]. The burden of infectious disease is highest in India [5].
The prevalence of the use of antimicrobial agents varies from Pharmacology Section24 to 67% in India [5, 6], and about 64% of the total antibiotics which are prescribed are either not indicated or are prescribed in incorrect dosages or are inappropriately prescribed [5,7]. They account for more than 50% of the drugs which are sold [7], which puts an excessive strain on the limited health care budget [5]. According to the results of various surveillance studies which were done, the percentage of irrational antibiotics which was reported was 40-60% [8]. Antibiotic resistance develops with the inappropriate use, which includes the wrong indication, mode of use, and the poor adherence of the prescribed drugs [5]. Many strategies have been proposed for the use of antibiotics, like a formulary replacement or restriction, health care provider education, feedback activities, approval requirement from an infectious disease specialist for the drug prescription [8] and a more rational use of antimicrobial agents all over the world [5].
The concept of rational drug use is new in the developing countries [9] and it refers to prescription of the right drug to the right patient, in the right dose, at right time intervals and for the right duration [10]. Some measures are required for the rational drug use, which include the development and revision of the national essential drug list, the national formulary development, the amending pharmacy act and the opening of drug information centres [11]. The rational drug therapy practice include members of the health care team and the patients’ knowledge regarding their medications and their use [9,12].
Various studies which were done in India and other developed countries have highlighted the importance of rational drug therapy, along with educational interventions and a strict antibiotic policy, but most of these studies have either taken into consideration, the rational use of antibiotics or an educational intervention. Hence, we considered it worthwhile to study the knowledge, attitude and the perception of the practitioners towards a rational antibiotic use.
AIMS AND OBJECTIVES
To study the knowledge, attitude and the perception among the practitioners towards a rational use of antibiotics.
MATERIALS AND METHODS
This prospective, cross sectional survey was carried out on registered practitioners in a hospital setting, after getting the approval of the Institutional Ethics Committee (IEC). All the registered practitioners who were working in the hospital setting and were willing to give written informed consents, were enrolled in the study. House surgeons, practitioners who were not working in hospital settings and those who were not willing to give written informed consents, were excluded from the study.
All the participants who were enrolled in this study had to fill up a structured validated questionnaire which was used to assess the knowledge and perception among physicians towards a rational use of antibiotics [13–15]. This research tool had three sections to assess the knowledge, attitude and the perception, which was based on the Likert scale. The knowledge section had eight questions; the first question consisted of the knowledge on the definition of rational drug use; the next seven questions had statements which were measured on a five-point scale, which varied from strongly agreeing to strongly disagreeing.
The attitude section had nine questions, of which five were statements which had to be ranked on a five-point scale and the other questions in this section included those on the preferred antibiotics and on the factors which influenced the prescriptions. The perception section had nine statements which had to be ranked on a five–point scale; the last question was further subdivided into four sections which were also assessed on the five-point scale and were based on the advice of fellow colleagues.
STATISTICAL ANALYSIS
Descriptive statistics was primarily used and the data that was collected was expressed as percentage. All the data were analyzed by using the Microsoft Excel software.
RESULTS
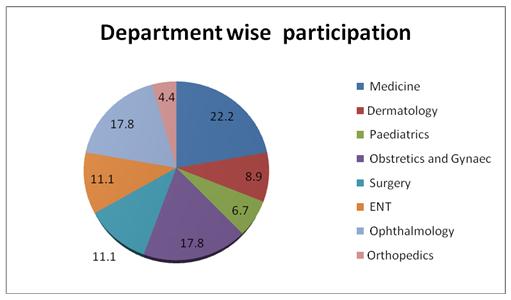
Of the total 70 questionnaires which were distributed, 45 provided complete responses and were included for the analysis. The participants included 39 practitioners and six post graduates. The response rate was about 65%. Among the participants, 26 were males and 19 were females. Their mean age was 43.9 (± 14.2) years. A department wise distribution of the participants is shown 676 in [Table/Fig-1]. A majority of the participants were from the Medicine Department (22%).
Department wise distribution of participants
KNOWLEDGE
All the participants were aware about rational drug use, as was evident by the definitions which were provided by them, but only 62% correctly answered the definition of rational drug use. The other aspects of the knowledge questionnaire are presented in [Table/Fig-2].
Percentage of participant that agreed on knowledge component of 5-point scale
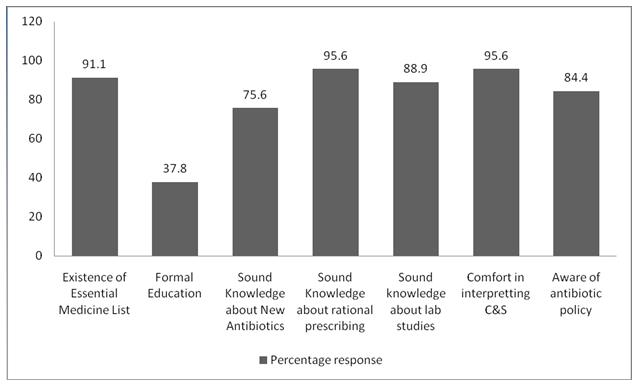
Ninety one percent of the participants agreed that they were aware of the existence of the essential drug list. 70% agreed and 5.6% strongly agreed that they had a sound knowledge about the new antibiotics and their usage, even though only 38% had a formal education on the newer antibiotics last year. About 2.2% disagreed and 2.2% answered neutrally, that they did not have/had a sound knowledge regarding prescription of the antibiotics rationally. 88.9% positively responded that they had a sound knowledge about the laboratory studies which were related to infections. 24.5 % strongly agreed and 71.1% agreed that they were comfortable in interpreting the culture and sensitivity results. About 84.4% were aware of the antibiotic policy which had to be followed in hospitals.
ATTITUDE
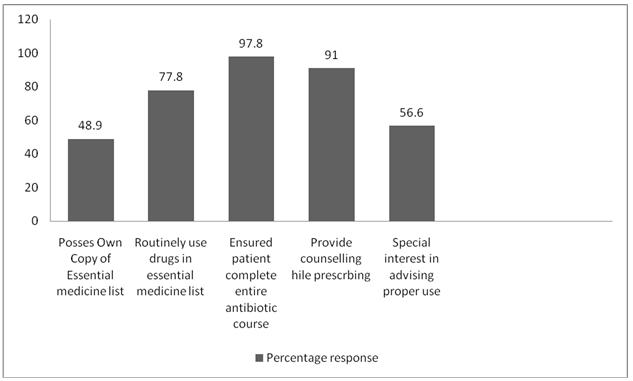
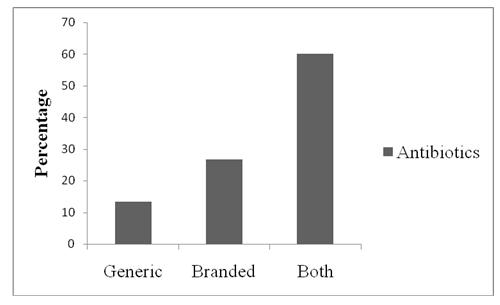
Of the nine questions which were asked to assess the attitude, five questions were measured on the five point scale [Table/Fig-3]. Forty-nine percent participants agreed that they had their own copy of the Essential Medicines List, but 20% of the participants were neutral on the use of drugs which were included in the essential medicine list, routinely in the prescription. 2.2% were not using it. About 97.8% ensured their patients had completed the entire course of the antibiotic therapy. 50% participants strongly agreed and 41% agreed that they had provided counselling while prescribing medications to their patients and 56.6% said that they had taken special interest in advising their patients about the proper use of antibiotics. Most of the participants answered that they had prescribed both branded as well as generic antibiotics [Table/Fig-4]. The beta lactam antibiotics were the most commonly prescribed antibiotics, and the prescriptions of the antibiotics were mostly influenced by the type of surgery and by the culture and the sensitivity reports [Table/Fig-5].
Percent of response on attitude component of 5-point \ scale
Percentage of antibiotic prescription
Response on Attitude component
| What are your preferred classes of antibiotics? | What are the influencing factors in your antibiotic decisions? | What kinds of intervention might influence the type of antibiotic you prescribe? |
| Penicillin, Cephalosporins Fluoro quinolones Amino glycosides Macrolides Topical - Chloramphenicol | Culture Report – Spectrum Nature & Severity of Infection Clinical Picture of infection System involvement Community/hospital acquired infection Co morbid condition Post operative infection Efficacy & safety Allergic history | Surgery Culture & Sensitivity Blood picture/count CME Journals MIMS Cost Analysis Present Antibiotic usage |
PERCEPTION
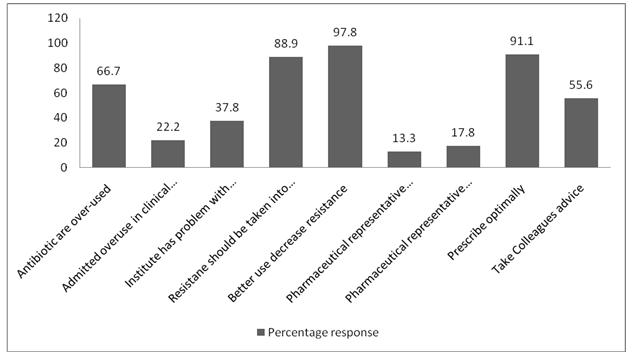
66.7% percent participants were of the opinion that antibiotics were generally overused, but most of the participants said that they had not over used antibiotics in the clinical practice (45%) and 32.8% were neutral in this matter. 88.9% considered the overall issues of 677resistance while they prescribed antibiotics for individual patients. About 47.8% strongly agreed and 50% agreed that a better use of antibiotics could help in decreasing the antibiotic resistance. Their interactions with pharmaceutical representatives had influenced their antibiotic prescriptions (13.3%). But 53% were neutral and 17.8% agreed on the influence of pharmaceutical representatives on others. About 37.8% of the participants opined that there was a problem of antibiotic resistance in the hospital. 91% thought that they had prescribed antibiotics optimally and only 55.6% had sought inputs from fellow colleague on the antibiotic choices [Table/Fig-6].
Percent of response on perception component of 5-point scale
Twenty-five participants who either strongly agreed/ agreed that they sought inputs from their fellow colleagues, also answered the further questions which were put to them for a clarification on the inputs from colleagues [Table/Fig-7]. Most of the participants agreed that the feed back from their fellow colleagues was useful, that they wanted more feedback and that there were patients’ inputs on the choice of antibiotics. A majority stated that a hospital antibiotic policy would be more helpful for achieving a rational antibiotic use.
Percent of response on perception component of 5-point scale on participants who took input from fellow colleague
| Statement | Strongly Agree% | Agree % | Neutral % | Disagree % | Strongly Disagree% |
|---|
| I feel the feedback given byfellow colleague(s) on antibiotic decisions is useful | 14.4 | 70 | 15.6 | 0 | 0 |
| I want more feedback from fellow colleague(s) on antibiotic choices | 26.7 | 31.1 | 41.2 | 1 | 0 |
| A hospital policy would be more helpful to achieve rational antibiotic use | 37.8 | 55.2 | 7 | 0 | 0 |
| There are patient influences on choice of antibiotics | 14.4 | 33.3 | 35.6 | 6.7 | 10 |
DISCUSSION
Our study was done to assess the knowledge, attitude and the perception among the practitioners towards a rational use of antibiotics. The results showed that most of the participants had agreeable knowledge about a rational use of antibiotics and an attitude to prescribe drugs as per the essential drug list, they had ensured a proper use of antibiotics by their patients, and they had a perception that antibiotics were being overused and that rational drug prescribing had an important role in reducing the antibiotic resistance.
The results of our study were similar to those of a study which was conducted in two hospitals in India, which had shown that there was extensive antibiotic prescribing and a high use of combinations of antibiotics; a need was felt to formulate and implement, based on the local prescribing and resistance data, with appropriate antibiotic prescribing guidelines [3]. The difference of that study from our study lay in the fact that the participants of our study believed that they were more rational in prescribing guidelines.
In a study which was done in Turkey to evaluate the rational antibiotic use and the impact of the implementation of a new restriction policy, showed a significant increase in the rational use of antibiotics after a restriction policy was made, with a decrease in the antibiotic use and an increase in the appropriate antibiotic use of antibiotics [8]. The restriction policy also lowered the costs of the antibiotics and their consumption in one hospital [1].
Another study which was done in Pakistan to evaluate the prescribers approach towards a rational drug practice, showed that the drug practice among the hospitalized patients was irrational, with high levels of medication errors. An accurate prescribing decision, an appropriate treatment, and a rational use of drugs are the major needs of the day, to ensure a safe medication practice [9].
A study which was done in Nepal to define the extent and the pattern of drug prescribing with an emphasis on those of antibiotics among the medical outpatients of a teaching hospital, showed that antibiotics were the most frequently prescribed therapeutic class. Although the selections of the antibiotics were rational, bacteriological confirmations prior to the institution of antibiotics, were not done in any case. The inclination towards the use of branded products and the overuse of antibiotics were revealed as the problems which required educational interventions and a strict antibiotic policy [10].
A cross-sectional study which was done to analyze and compare the antibiotic prescribing for inpatients, in two private sector tertiary care hospitals in India, showed extensive antibiotic prescribing and a high use of combinations of antibiotics. It showed a need to formulate and implement appropriate antibiotic prescribing guidelines, based on the local prescribing and resistance data [3].
In spite of numerous methods which were developed by healthcare institutions for an improvement in the antibiotic use, excessive and inappropriate antibiotic prescribing is still a major problem which is prevalent throughout the world. It has been reported that in the United States, approximately 60% of all the hospitalized patients receive an antimicrobial agent and that about 50% of its use is unnecessary or otherwise inappropriate [16,17]. The main consideration for the proper use of antibiotics is to select the optimal agent which has a proper dosage and a time duration, by minimizing the emergence of resistance and to provide affordable health care [8,18,19]. Other strategies for the rationalization of antibiotics include medical education, utilization of the hospital formulary, written justification forms, medical consultations and safe as well as cost effective prescribing patterns [1,5].
Another study demonstrated that beta lactams were one of the most frequently prescribed antibiotics, which are similar to the results of our study. Although the prescribing was rational, it was felt that an inclination towards branded products and an over use of antibiotics were prevalent. The need of an educational intervention, as well as a strict antibiotic policy was felt [10]. Developing and maintaining an electronic documentation of the patients’ medical records may serve as a valuable tool for auditing the prescriptions frequently and for implementing the antibiotic policy. Also, the implementation of a computerized reporting system in the hospital setup is suggested, so that it may hasten the detection of the early signals of potential ADRs. In addition, all the healthcare professionals should be given education and training in all the infection control activities which are being coordinated by the Hospital Infection Control Committee.
To conclude, the participants of our study had agreeable knowledge about the rational use of antibiotics and an attitude to prescribe drugs as per the essential drug list, they had ensured a proper use of antibiotics by their patients, and they had a perception that antibiotics were being overused and that antibiotic resistance had an important role in the rational drug prescriptions.
[1]. Ozkurt Z, Erol S, Kadanali A, Ertek M, Ozden K, Tasyaran MA, Change in antibiotic use, cost and consumption after an antibiotic restriction policy applied by infectious disease specialistJpn J Infect Dis 2005 58:338-43. [Google Scholar]
[2]. Fadare JO, Tamuno I, Antibiotic self-medication among university medical undergraduates in Northern NigeriaJournal of Public Health and Epidemiology 2011 3:217-20. [Google Scholar]
[3]. Sharma M, Eriksson B, Marrone G, Dhaneria SP, Lundborg CS, Antibiotic prescribing in two private sector hospitals; one teaching and one non-teaching: A cross-sectional study in Ujjain, IndiaBMC Infectious Disease 2012 12:155url.http://www.biomedcentral.com/1471-2334/12/155 [Google Scholar]
[4]. World Health Organization: WHO infectious disease report: leading cause of death. 2004; 1999 [Google Scholar]
[5]. Ahmad A, Parimalakrishanan Mohanta GP, Patel I, Manna PK, A study on utilization pattern of higher generation antibiotics among patients visiting community pharmacies in Chidambaram, Tamil Nadu at South IndiaInt J Pharm 2012 2:466-71. [Google Scholar]
[6]. Mohan J, Gopal KM, Meganathan M, Sasikala P, Gowdhaman N, Balamurugan K, A Study on Utilization Pattern of Antibiotics for the Complicated Urinary Tract Infections in a Tertiary Care CentreGlobal J Pharmacol 2011 5:1-3. [Google Scholar]
[7]. Kunin CM, Rational use of antibioticsWHO Drug Information 1990 4:4-7. [Google Scholar]
[8]. Tunger O, Karakaya Y, Cetin CB, Dinc G, Borand H, Rational antibiotic useJ Infect Developing Countries 2009 3:88-93. [Google Scholar]
[9]. Amin A, Khan MA, Azam SMF, Haroon U, Review of prescriber approach towards rational drug practice in hospitalised patientsJ Ayub Med Coll Abbottabad 2011 23:19-22. [Google Scholar]
[10]. Kumar J, Shaik MM, Kathi MC, Deka A, Gambhir SS, Prescrbing indicator and pattern of use of antibiotics among medical outpatients in a teaching hospital of Central NepalJournal of College of Medical Sciences.-Nepal 2010 6(2):7-13. [Google Scholar]
[11]. Alam K, Mishra P, Prabhu M, Shankar PR, Palaian S, Bhandari RB, Study on rational drug prescribing and dispensing in outpatients in a tertiary care teaching hospital of Western NepalKathman Uni Med J 2006 4:436-43. [Google Scholar]
[12]. Pharmacy communication. In: Hassan WE (editor)Hospital Pharmacy 1985 5thPhildelpiaLea and Febiger:154-59. [Google Scholar]
[13]. Adebayo ET, Hussain NA, Pattern of prescription drug use in Nigerian army hospitalsAnnals of African Medicine 2010 9:152-58. [Google Scholar]
[14]. Wood F, Simpson S, Butler CC, Socially responsible antibiotic choices in primary care: a qualitative study of GPs’ decisions to prescribe broad-spectrum and fluroquinolone antibioticsFam Pract 2007 24:427-34. [Google Scholar]
[15]. Srinivasan A, Song X, Richards A, Sinkowitz-Cochran R, Cardo D, Rand C, A survey of knowledge, attitudes, and beliefs of house staff physicians from various specialties concerning antimicrobial use and resistanceArch Intern Med 2004 164:1451-56. [Google Scholar]
[16]. Polk RE, Fishman NO, Antimicrobial stewardship. In: Mandell GL, Bennett JE, Dolin R, editorsMandell, Douglas, and Bennett’s Principle and Practice of Infectious diseases 2010 7thPhiladelphiaElsevier Churchill Livingstone:677-85. [Google Scholar]
[17]. Inan A, Daglý O, Akçay SS, Engin DÖ, Karagül E, Özyürek SÇ, Antibiotic use and cost in a teaching hospital in IstanbulJ Microbiol Infect Dis 2011 1:128-33. [Google Scholar]
[18]. Niederman MS, Principles of appropriate antibiotic useInt J Antimicrob Agents 2005 26(Suppl 3):S170-75. [Google Scholar]
[19]. Nathwani D, Davey P, Antibiotic prescribing-are these lessons for physicians?Q J Med 1999 92:287-92. [Google Scholar]