The patterned traceries of the fine ridges on the fingers, palms and soles must have aroused interest long ago, though when it was that men first noticed them, can never be known. There exist records that indicate an acquaintance with these traceries, or dermatoglyphics, prior to the period of the scientific study [1].
Dermatoglyphics is a collective term for all the integumentary features (skin patterning of the fingers, toes, palms and soles) and it applies to the division of the anatomy which embraces their study. In this pattern, the configurations include the finger print, palm print and the toe print. Several decades of finger print studies have helped people to understand more on this subject. The palm prints include much more information than the finger prints [1].
The study of dermatoglyphics plays an important role in the diagnosis of chromosomal disorders. Dermatoglyphics has revealed its significance in Down’s syndrome, Turner’s syndrome and in the Trisomy 18 syndrome. Breast cancer is the commonest neoplastic disease in women in the western world, with a lifetime risk of 11-12% in the general population [2].
A search of the literature has revealed that a family history of breast cancer might be associated with a specific fingerprint pattern. A fingerprint determination is genetic but it has been reported to be affected by the environmental factors in the first trimester of pregnancy. After birth, the patterns remain more or less constant and hence, they may serve in studying the genetic patterns in any individual. The studies of the prints thus represent a noninvasive anatomical marker of the breast cancer risk. The fingerprints could be used for screening or to guide the future research in this direction.
MATERIALS AND METHODS
This cross-sectional study was conducted in the Department of Anatomy, Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan, India. Hundred cases of breast cancer were taken up for dermatoglyphic studies from the day care centre of the Bhagwan Mahaveer Cancer Hospital and Research Centre, Jaipur, Acharya Tulsi Regional Cancer Centre, Bikaner and Ravindranath Tagore Medical College and Hospital ,Udaipur, India. Both the cases and the controls were females. These female patients used to attend the chemotherapy clinics. Their age group ranged from 20-75 years. The socio-economic strata and the qualification of the subjects varied from the primary standard to the secondary standard.
Written consents were taken from both the cancer patients and the controls. These observations were compared with those of the normal healthy control group of the hundred female subjects who had not suffered from any malignancy till date. An effort was made to find the correlation between cancer and the epidermal ridge patterns of the palm. The dermatoglyphic prints were taken by the ink method, as was described by Cummins and Midlo [1]. Hand prints were collected from the students of Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan, India, who were between the age group of 20-21 years, which formed the control hand prints and the prints of middle aged and elderly females who resided in Jaipur, Rajasthan, India were also taken [Table/Fig-1]. This study was conducted on established cases of breast cancer as well as on normal controls from the Rajasthani population. The diagnoses of these patients were established by doing histopathological biopsies. These patients were divided into two groups:
Finger prints and palm prints of a control taken during study.
Group I: Carcinoma breast patients who had no history of any other genetic disorder or hereditary diseases.
Group II: Those who had no family history of either breast cancer or any other inheritable disease.
The materials which were required were: Camel quick drying duplicating ink, a rubber roller, an inking slab (a thick glass sheet which was fixed on a wooden support), an A4 size white sheet, a pressure pad which was made of rubber foam, cotton puffs, a scale, a pencil and a pen. The fingerprints were taken on an A 4 size paper by the rolling finger technique [Table/Fig-2].
Rolling palm Technique of taking finger prints.
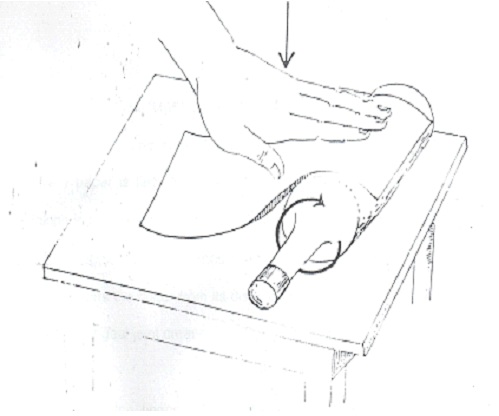
First, the hands were washed with soap and water and the greasy material was cleared off with the help of ether [Table/Fig-1]. A small dab of printer’s ink was squeezed out on the inking slab and it was spread into a thin film with the help of a roller for the direct inking of the fingers. The palm was smeared uniformly with the inked roller to cover the whole area of the palm which had to be printed for the examination.
In the next step, the paper was set over the round bottle and the palm and the moderately open fingers were successively rolled over by applying some pressure on them, while permitting the bottle and the paper to move forward, so that the finger prints of the whole of the palm and the plain were obtained. The rolled finger prints are taken by rotating the fingers both during the inking and printing, so as to obtain a complete impression of the finger tip [Table/Fig-1].
The precautions which were followed while taking the finger and palm prints:
The finger was pressed edge down against the paper margin and 610it was rolled to the opposite edge in a manner which was similar to that which was done during inking, to minimize a certain awkward manipulation. The thumb was placed with the ulnar edge down and it was rolled towards the body. The other digits are placed with their radial edges down and they were rolled away from the body. In taking imprints of the palm, special attention is required: the zone of flexion creases at the wrist and at the ulnar margin and the flexion creases where the fingers join the palm and at the central hollow of the palm. Unless these are inked and printed, the palmer prints will lack the critical features.
The following parameters were observed and compared between the two groups:
The fingertip ridge pattern [Table/Fig-3]
The ridge counts in the individual fingers of both the hands
The Total Finger Ridge Count of both the hands (TFRC)
The Absolute Finger Ridge Count (AFRC)
A loop with a count of eleven ridges.Ridges are counted along the indicated line which Point of Triradius (outer terminus) and point of core (inner terminus).

The finger tip ridge pattern was compared between the cancer patients and the controls by using the Z-test. For the Z-test, whenever the calculated Z value was below 1.96, the difference in the proportions was considered as non-significant.
RESULTS
The mean age of the cancer patients was 45.6+11.0 years while for the controls, it was 33.3+14.96 years. A significant (P<0.001) increased percentage of the arch pattern (39.8% left hand and 36.0% right hand) was seen in the cancer patients as compared to that in the controls (16.2% left hand and 11.4% right hand ) [Table/Fig-4] and [Table/Fig-5]. A significantly higher percentage of the cases (26%) as compared to the controls (3.7%) showed arches (P<0.001), while the radial loops (Lr) which were associated with them were significantly less (P<0.001).
Comparison of Tip Ridge Pattern of All fingers (Left) between cancer cases and controls.
| Status | Number | Ulnar Loop (Lu) | Whorl (W) | Arch (A) | Radial Loop (Lr) |
|---|
| Case | 500 | 16 | 101 | 199 | 184 |
| % | 3.2 | 20.2 | 39.8 | 36.8 |
| Control | 500 | 13 | 154 | 81 | 252 |
| % | 2.6 | 30.8 | 16.2 | 50.4 |
| Z value | 0.57 | 3.85 | 8.31 | 8.20 |
| P-value | NS | < 0.001 | < 0.001 | < 0.001 |
Comparison of Tip Ridge Pattern of All fingers (Right) between cancer cases and controls.
| Status | Number | Ulnar Loop (Lu) | Whorl (W) | Arch (A) | Radial Loop (Lr) |
|---|
| Case | 500 | 25 | 106 | 180 | 189 |
| % | 5.0 | 21.2 | 36.0 | 37.8 |
| Control | 500 | 1 | 139 | 57 | 296 |
| % | 0.2 | 27.8 | 11.4 | 59.2 |
| Z value | 4.77 | 2.43 | 9.15 | 6.77 |
| P-value | < 0.001 | < 0.05 | < 0.001 | < 0.001 |
The arches in the left index finger were seen in a significantly higher percentage of the cancer cases as compared to those in the controls (P<0.001). A significantly lower percentage of the ulnar loops (2%) in the right index finger were seen in the cancer patients as compared to that in the controls. A significantly large number of arches were seen in the cancer patients as compared to the controls (p<0.001) in the Ieft and right middle fingers. A significantly large number of arches were seen in the right and left ring fingers (p<0.001) A large number of arches were seen in the left little finger. The arch pattern was more common in the cancer patients (39.8% vs. 16.2%), while the radial loop (36.8% vs. 50.4%) and the whorl (20.2% vs. 30.8%) were less common in the cancer patients as compared to those in the controls. The arch pattern was more common in the cancer patients (36.0% vs. 11.4%), while the radial loop (37.8% vs. 59.2%) and the whorls (21.2% vs. 27.8%) were less common in the cancer patients as compared to those in the controls. The ulnar loop which showed a comparable pattern on the left hand, showed a different pattern on the right hand. The ulnar loop was more common in the cancer cases as compared to the controls [Table/Fig-4] and [Table/Fig-5]. The lower values of TFRC (below 50) were associated with the cancer patients, whereas the higher values (>126) were associated with the controls. This suggested that the lower values of TFRC, particularly those which were below 50, could be associated with a risk of developing cancer [Table/Fig-6]. The lower values of AFRC (below 100) were associated with the patients, whereas the higher values (>201) were associated with the controls [Table/Fig-7]. This suggested that the lower values of TFRC and AFRC, particularly those which were below 100, could be associated with the risk of developing cancer.
Distribution of subjects according to their status and TFRC.
| Status | ≤50 | 51-125 | ≥126 | Total |
|---|
| Cases | 23 | 30 | 47 | 100 |
| Controls | 1 | 26 | 73 | 100 |
| Total | 24 | 33 | 58 | 200 |
Distribution of subjects according to their status and AFRC.
| Status | ≤100 | 101-200 | ≥ 201 | Table Total |
|---|
| Cases | 32 | 42 | 26 | 100 |
| Controls | 12 | 49 | 39 | 100 |
| Table Total | 44 | 91 | 65 | 200 |
| Chi-square = X2 =12.22; degrees of Freedom=df=2; P<0.002 |
DISCUSSION
Breast cancer is the most common malignancy among women in the world. According to the latest report of the NCRP (National Cancer Registry Program), around 25% of the total cancer cases are reported to be that of breast cancer [4]. The present study reported a relatively high increase in the arches in the cancer patients as compared to that in the controls (36.0% vs. 11.4%). Bukovic et al., conducted a dermatoglyphic study on ovarian cancer patients. A high percentage of arches (right-10% and left-11%) was seen in the cancer patients as compared to the controls (4% and 5%). Sukhre and Mahajan found a significantly increase in the number of arches in carcinoma breast patients as compared to that in the controls, on both the hands. Inamdar et al., reported an increase in the frequency of the arch pattern on the left hand of Carcinoma cervix patients (8.4% vs. 3.8%).Oladipo et al., reported an increase in the frequency of the arch pattern on left hands of the females who had malignant mammary neoplasms (20% vs. 7%). Thus, our findings were in conformity with the findings of Bukovic et al., [5], Sukhre and Mahajan [6], Inamdar et al., [7] and Oladipo et al., [8]. Charlton et al., [9] reported an association between the ABO blood groups and the fingerprints of 275 cancer patients and 251 controls, which were tabulated on the basis of the sex and the blood group. There were 14 instances of 6 or more arches among the 304 cancer patients and there were 8 among the 339 controls.
Seltzer et al., reported the low frequency of the arches in the carcinoma breast patients as compared to that in the controls (cases-5.6% vs. control 10.0%). Abbasi et al., reported a decrease in the frequency of the arches. Sridevi et al., reported a significant decrease in the arch pattern on the digits II, III and IV. On comparing all the ten digits, a significant decrease in the arch pattern was reported (p=0.05) from the right hands of the carcinoma breast patients. The findings of the present study did not coincide with the findings of Seltzer et al., [10], Abbasi et al., [11] and Sridevi et al., [12], where there was decrease in the frequency of the arches. The present study revealed that a TFRC<50 was associated with a risk of breast cancer. Fuller (1973) reported a low TFRC (123.49±44.35), but the difference was not significant. Huang and MP [13] reported no significant differences in the TFRC and the AFRC between the cancer patients and the controls. Inamdar et al., reported a significant increase in the frequency of TFRC in the cancer patients as compared to the controls. Chintamani et al., reported a low mean total finger ridge count in the carcinoma breast patients as compared to the controls. Sridevi et al., reported a high TFRC in the cancer patients as compared to the controls. Those with an AFRC of < 100 were associated with cancer patients and those with an AFRC of > 201 were associated with the controls. Our results were in conformity with the findings of Fuller [14], Chintamani et al., [15] and Oladipo et al., [8]. Our results were not in agreement with those of Inamdar et al., [7], Sridevi et al., [12] and Huang and MP [13].
For centuries, the features of the hands have fascinated scholars, sages, theologians, doctors and laymen alike. The modern study of the hand has been far removed from the popular image of the soothsaying hand reader uttering mysterious incantations in an arcane language. Rather, after decades of scientific research, the hand has come to be recognized as a powerful tool in the diagnosis of psychological, medical and genetic conditions. The study and the comparison of all the variables of both the hands of the carcinoma breast patients and the controls enabled us to create a scoring system. This scoring system is based on the use of two fingertip patterns-the arch and the radial loop. An increase in the number of arches (more than or equal to 2) on both the hands is designated as score 1, whereas, when the number is less than or equal to 2 on any of the hands, the score is 0. Similarly, the number of the radial loop, if it is zero on any hand, it is designated as score 1 and if the number is more than one, the score is 1. The number of whorls, if it is zero, it is designated as score 1 and if the number is more than 1, the score is 0. A TFRC number of less than 50 is designated as score 1 and if it is more than 50, the score is 0. An AFRC number of less than 100 is designated as score 1 and if it is more than 100, the score is 0 [Table/Fig-8].
Definition of score to assess risk variables
| Variable | Number | Score |
|---|
| R-Arch / L-Arch | ≤ 2 | 1 |
| < 2 | 0 |
| R-Lr / L-Lr | 0 | 1 |
| ≤ 1 | 0 |
| R-W/L-W | 0 | 1 |
| ≤ 1 | 0 |
| TFRC | ≥ 50 | 1 |
| > 50 | 0 |
| AFRC | ≤ 100 | 1 |
| >100 | 0 |
CONCLUSION
To conclude, the fingerprint determination is genetic. It is also affected by the environment in the first trimester of pregnancy. After birth, the patterns remain more or less constant and hence, they may serve in studying the genetic patterns in any individual. The fingerprints could thus be used for screening or to guide the future research in this direction and one day, the screening for breast cancer could be well at our fingertips.