The blindness caused by glaucoma is expected to reach alarming proportions. It is the second most common cause of world’s blindness and majority of them reside in Asia [1, 2]. India accounts for 12.9% of the Primary Open Angle Glaucoma (POAG) cases and 12.7% of the Primary Angle Closure Glaucoma (PACG) cases in the world [3].
There were studies which account for the different subtypes of glaucoma and showed the varying predominance of glaucoma types in different regions of India in urban [4] and rural populations [5–7]. There is only little data on the distribution of these glaucoma subtypes according to the religion of the patients, as India has complex patterns of migration and this contributes to the marked ethnic diversity between the different regions and religions.
So, to further contribute in this regard, we conducted a study in the Moradabad district of Uttar Pradesh (U.P), India to find out the distribution pattern of the glaucoma subtypes, mainly in the Muslim and the Hindu populations, as the Muslim population was 49.13% in Moradabad as against 18.49% in U.P, India. The Hindu population accounts for 53.85% of the glaucoma cases in Moradabad, which is much lower than that in the state of Uttar Pradesh (80.62%) [8].
MATERIALS AND METHODS
A retrospective analysis was done of 1500 patients data, aged >25 years, who were diagnosed as having glaucoma in one or both the eyes in the Ophthalmic Outpatient Department of the Teerthanker SectionMahaveer Medical College, Moradabad, U.P, India, from January 2007 to August 2012. The hospital draws patients primarily from two major religions (Islam and Hinduism). The analysis was done on all the patients who were diagnosed as having primary and secondary glaucoma, as well as on glaucoma suspects. The data which was based on their demographic profile, any associated systemic illness and the family history, was obtained from the previous medical records.
Exclusion criteria
Incomplete data
Congenital and Developmental glaucoma
Patients lost to follow up
A previous glaucoma surgery
All the ophthalmologic procedures were performed by an experienced ophthalmologist and the diagnosis was established with the consensus of a senior ophthalmologist.
The work up of the history and the ophthalmic examination included:
The Best Corrected Visual Acuity (BCVA)
The IOP which was obtained by using a Goldman applanation tonometer. The average of 3 readings was taken as the final reading best corrected visual acuity
Slit lamp examination best corrected visual acuity
Gonioscopy, with the use of a Goldman two-mirror lens, was done in all the patients. The occludability was assessed by using a dim ambient and a slit lamp illumination, with the patient looking straight ahead. The anterior chamber angle was classified by using Shaffer’s grading [9]. Grade 2 or less was considered as occludable, and grade 3 or more was considered as open. The eyes with occludable angles and no glaucoma were labelled as latent ACG.
An optic disc examination was done with a+90 dioptres (D) lens at 16 × magnification without a pupillary dilatation. The Vertical Cup-to-Disc Ratio (VCDR) was used as the index for the structural glaucomatous change. If the stereo view was not satisfactory due to the opacity of the lens or due to the restrictions of the pupil size, the pupil was dilated by using 0.5% tropicamide and 0.5% phenylephrine hydrochloride, and the optic disc was examined with an indirect ophthalmoscope by using a+20 D lens. The fundus changes which were suggestive of glaucoma included focal notching of the disc, deepening of the cup, thinning of the neuroretinal rim, a laminar dot sign, overpass cupping, saucerization of the cup, asymmetrical cupping in the two eyes and Retinal Nerve Fibre Layer (RNFL) defects.
A field examination was done by using automated perimetry (the Humphrey Field Analyzer 30-2 program) if the fundus findings were suggestive of glaucoma. The unreliable fields [10] with the typical glaucomatous visual field damage (i.e. nasal step, or paracentral, Seidel’s or arcuatescotoma, or deep diffuse depression) were repeated twice [11].
A glaucomatous visual field defect was considered to be present if the following were found:
A Glaucoma Hemifield Test (GHT) result which was outside the normal limits, and
A cluster of three or more nonedge, contiguous points, which were not crossing the horizontal meridian, with a probability of 5% of the age-matched normals on the pattern deviation plot, on two separate occasions.
Some components of the examination could not be carried out on the patients who refused such an examination, those with cataracts, or those with corneal opacities.
PAOG was defined as a condition in a subset of patients with open angles, a raised IOP which was associated with either a glaucomatous cupping of the optic nerve head or visual field changes which were suggestive of glaucoma [12]. The patients who were less than 35 years of age, with a clinical picture which was similar to that of POAG, were labelled as having Juvenile Open Angle Glaucoma (JOAG) [12].
PACG was said to exist when a person had, in the same eye or in both eyes (a) a pressure of >21 mm Hg and (b) an anterior chamber angle which was two-thirds obstructed. The angle closure was considered to be either appositional or synechial. The chronic appositional angle closure was diagnosed in the presence of a raised intraocular pressure and with closed angles on gonioscopy, in the absence of peripheral anterior synechiae (PAS). The presence of glaucomatous field defects or optic disc changes was not considered as mandatory for the diagnosis of angle closure glaucoma [12], [13]. The latent ACG was comprised of asymptomatic patients with occludable angles [12]. The ocular hypertensives were defined as a subset of patients with open angles and a raised IOP but neither with an optic nerve head nor visual field changes [12].
The normal tension glaucoma patients were classified as having open angles, and progressive optic nerve head changes or a visual 500field loss which was suggestive of glaucoma in the absence of an elevated IOP [12]. The glaucoma suspects included (a) a subset of patients with open angles, an IOP of less than 22 mmHg and absence of field changes but with optic nerve head changes; and (b) patients with a strong family history of glaucoma in the absence of optic nerve head changes or a high IOP [12].
RESULTS
This study was done in September 2012 at TMMC and RC. It included a retrospective analysis of the glaucoma patients who came to the eye OPD from January 2007 to August 2012.
The total number of the ophthalmic patients who were seen in the OPD during this period was 73,864. 43579 (58.9%) were Hindus, 28068 (38.0%) were Muslims, and the rest [2217 (3.0%)] were others. Out of these, a total of 1500 (2.03%) glaucoma patients were identified. The mean age was 52.7 years with an S.D. of 12.1.
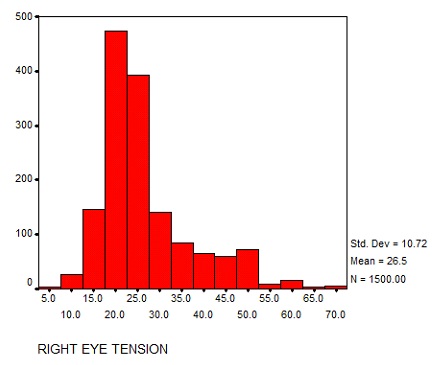
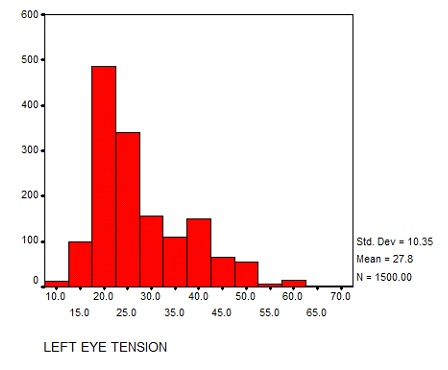
46.4% patients were males, while 53.6% patients were females. 37.4% were Hindus, while 58.8% were Muslims. 3.8% fell in the others category. The IOP was recorded by suing the Goldman applanation tonometer. The mean IOP recorded in RE was 26.5 mm Hg with S.D of 10.72 [Table/Fig-1] and in LE it was 27.8 mm Hg with S.D. of 10.35 [Table/Fig-2]. By matching the IOP with the slit lamp examination findings and the field defects, the patients were categorized into various glaucoma subtypes.
Bar chart showing IOP recorded in RE (mm Hg).
Bar chart showing IOP recorded in LE (mm Hg).
Primary Open angle glaucoma was diagnosed in the maximum number of patients (33%), followed by Primary angle closure glaucoma (32.7%)[Table/Fig-3]. The gender distribution of glaucoma showed that POAG was the most common type of glaucoma in males (16.8%) and that PACG was the commonest type in females (18.8%) [Table/Fig-4].
Showing distribution of various glaucoma subtypes.
| Subtype | RE | LE |
|---|
| Juvenile open angle glaucoma | 37 (2.5%) | 40 (2.7%) |
| Primary open angle glaucoma | 490 (32.7%) | 495 (33.0%) |
| Primary angle closure glaucoma | 489 (32.6%) | 490 (32.7%) |
| Normal tension glaucoma | 110 (7.3%) | 95 (6.3%) |
| Secondary glaucoma | 38 (2.5%) | 36 (2.4%) |
| Ocular hypertension | 166 (11.1%) | 142 (9.5%) |
| POAG suspect | 133 (8.9%) | 164 (10.9%) |
| Non glaucomatous | 37 (2.5%) | 38 (2.5%) |
Gender distribution of glaucoma.
| Diagnosis | Male | Female |
|---|
| Juvenile open angle glaucoma | 23(1.5%) | 17(1.1%) |
| Primary open angle glaucoma | 252(16.8%) | 243(16.2%) |
| Primary angle closure glaucoma | 208(13.9%) | 282 (18.8%) |
| Normal tension glaucoma | 45(3.0%) | 50(3.3%) |
| Secondary glaucoma | 42(2.8%) | 32(2.1%) |
| Ocular hypertension | 70(4.7%) | 72(4.8%) |
| POAG suspect | 56(3.7%) | 108(7.2%) |
| Total | 696(46.4%) | 804(53.4%) |
A further analysis was done to find out the pattern of glaucoma which was present in the patients of different religions. They mainly included Hindus and Muslims. POAG (40.8%) was found to be leading form of glaucoma among the Hindu patients [Table/Fig-5] while PACG was the most common type of glaucoma (40.1%) among the Muslim patients [Table/Fig-6].
Glaucoma in Hindu patients.
| Diagnosis | Number of glaucoma patients (out of 1500) | Percentage within the religion |
|---|
| Juvenile open angle glaucoma | 15 (1.0%) | 2.7% |
| Primary open angle glaucoma | 229 (15.3%) | 40.8% |
| Primary angle closure glaucoma | 116 (7.7%) | 20.7% |
| Normal tension glaucoma | 41(2.7%) | 7.3% |
| Secondary glaucoma | 33(2.2%) | 5.9% |
| Ocular hypertension | 75(5.0%) | 13.4% |
| POAG supect | 52(3.4%) | 9.3% |
| Total | 561(37.4%) | |
Glaucoma in Muslim patients.
| Diagnosis | Number of glaucoma patients (out of 1500) | Percentage within the religion |
|---|
| Juvenile open angle glaucoma | 23(1.5%) | 2.6% |
| Primary open angle glaucoma | 244(16.3%) | 27.7% |
| Primary angle closure glaucoma | 353(23.5%) | 40.1% |
| Normal tension glaucoma | 54(3.6%) | 6.1% |
| Secondary glaucoma | 41(2.7%) | 4.6% |
| Ocular hypertension | 67(4.5%) | 7.6% |
| POAG supect | 100(6.7%) | 11.3% |
| Total | 882(58.8%) | |
DISCUSSION
We studied the retrospective data of 1500 glaucoma patients who came to our OPD between Jan 2007 and August 2012 at TMMC and RC, Moradabad, U.P, India. The hospital attracts patients from both urban and rural areas. The mean age of presentation was 52.7 years. The mean age of presentation of glaucoma varies from 30 to 60 years, as was seen in various studies [13], [14]. The prevalence of POAG (33.0%) was almost equal to that of PACG (32.7%). A considerable number of patients also belonged to the POAG suspect (11%) category. A tertiary care hospital based study reported an incidence of PACG in nearly half of the all adult primary glaucoma patients [15]. Glaucoma was found to be more common in females, as they constituted 53.6% of the total study patients. But we found a higher number of males (16.8%) with POAG as compared to females (16.2%). Although the difference was not much, a higher incidence of POAG in male patients was reported in a north Indian study [12].
The PACG cases were present in high numbers among the females (18.8%). However, no significant difference in the prevalence of PACG among the two sexes was reported in a Vellore eye study [13]. An Andhra Pradesh eye study reported a higher prevalence of PACG in females of the lower socioeconomic strata [4]. The prevalence of glaucoma varies, depending on the demographic, ethnic, racial and the socioeconomic factors [16], [17]. A Barbados eye study concluded that there was a higher prevalence of POAG in the black population [18]. The number of cases was more among the older age groups (≥70).
An Addis Ababa study reported a variation in the prevalence of glaucoma among the ethnic groups in Ethiopia, with exfoliation being more common in the Gurage population and chronic angle-closure glaucoma being more frequent in the Amhara population [19]. In India also, there is an extensive variation among the subpopulations, depending upon the religion, culture and the demographic pattern.
In our study, we tried to find the pattern of the prevalence of glaucoma in a tertiary care hospital setting, in a western Uttar Pradesh District i.e. Moradabad. This is important, as the area is dominantly inhabited by Muslim population [8]. The prevalence of glaucoma was found to be higher among Muslim patients, 882 (58.8%) as compared to 561(37.4%) Hindu patients. This was despite the fact that overall Hindu patients (58.9%) were more as compared to Muslim patients (38.0%).
POAG was found to be most common type of glaucoma (40.8%) among the Hindu patients, followed by PACG(20.7%). Whereas PACG was reportedly highly prevalent among the Muslim patients (40.1%) as compared to PAOG (27.7%). The difference which we found, might be due to some cultural practices which are more common in the Muslim population, like consanguineous marriages [20].
An important aspect of our study was that, probably this was the first study in northern India, which had tried to highlight the prevalence of glaucoma and its subtypes, based on religious factors. We emphasize that a better health planning is needed in the further management of glaucoma in this region.
The drawback of this study was that this was not a population based study and that the number of cases were less. We need a population based study in future, with a larger number of patients in this region, to establish the points which arose in this study.