Castleman`s Disease (CD) is a rare lymphoproliferative disorder and a mesenteric location is unusual. The unicentric variety is more difficult to diagnose clinically and it requires a histopathological confirmation. The excision biopsy itself will help both in the diagnosis and in planning the treatment. Here, we are presenting a case of unicentric mesenteric Castleman`s disease which we suspected to be lymphoma.
Castlemans disease, Unicentric, Mesenteric
INTRODUCTION
Castleman’s Disease (CD) is a benign, rare, lymphoproliferative disorder which was first described by Dr. Benjamin Castleman in 1956. It is also known as angiofollicular lymph node hyperplasia, angiofollicular lymphoid hyperplasia, gaint lymph node hyperplasia, lymphoid hamartoma, benign lymphoma or follicular lymphoreticuloma. This disease usually occurs in the mediastinum, lung, neck, axilla, pelvis and the retroperitonem. But a mesenteric CD is rare. The diagnosis is difficult but the management depends on whether it is of the multicentric or the unicentric (localized) type.
The mesenteric Castleman’s disease has to be differentiated from other benign or malignant mesenchymal lesions of the mesentery like stromal tumours, leiomyomas, leiomyosarcomas and fibromas. It is also associated with a number of malignancies, which include Kaposi’s sarcoma, non-Hodgkin’s lymphoma, Hodgkin’s lymphoma, and the POEMS syndrome. We are reporting a case of mesenteric CD in a middle aged man.
CASE REPORT
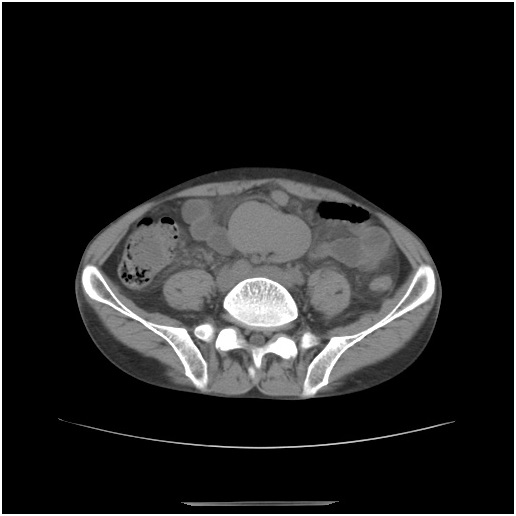
A middle aged man was admitted with pain in the abdomen which was there since 2 months. On physical examination, a tender, oval shaped, palpable mass was found in the left infraumbilical region, which measured about 4cm. On admission, the investigations showed microcytic hypochromic anaemia (Hb%-6.2 G% and PCV- 19.3%), proteinuria with elevated renal parameters (urea- 84 mg/dl and creatinine -5.1mg/dl) and chest X-ray with no radiological abnormalities. An abdominal ultrasound which was done, revealed a hypo echoic mass lesion in the left infraumbilical region. On further investigation with CT of the abdomen and the pelvis, a well-defined, soft tissue mass was seen in the mesentery, with internal foci of calcification and multiple enlarged mesenteric lymph nodes. The radiologist gave an impression of lymphoma [Table/Fig-1] and suggested fine needle aspiration cytology (FNAC)/biopsy for its confirmation.
Ct Scan Showing Well Defined Soft Tissue Mass in the Mesetery with Internal Foci of Calcification
CT guided FNAC showed the features of Non-Hodgkin’s lymphoma. However, the pathologist suggested a histopathological study of the mass for a confirmative opinion.
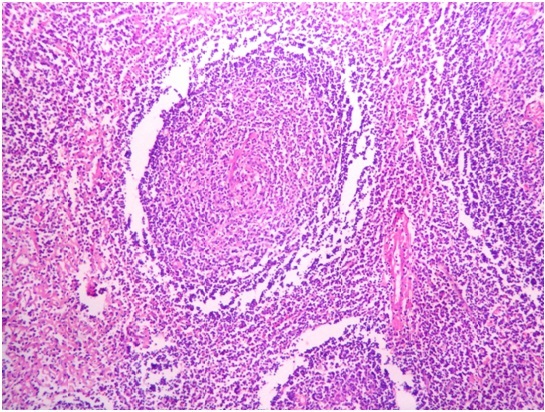
A minilaparotomy was done, which showed that there was a hard dark brown coloured mass in the mesentery which measured 5.5x5x 2 cm [Table/Fig-2]. The Histopathological Examination (HPE) study showed lymph nodes with thick capsules and a partially effaced architecture. The impression was of Castleman’s disease (CD), (giant lymph node hyperplasia)- mixed type (hyaline-vascular and plasma cell type) [Table/Fig-3].

The Hassall Corpuscle Like Atrophic Follicle Centre Contains A Radiating Vessel Simulating A Lollipop Sign
The patient had an uneventful postoperative course and is on regular follow up.
DISCUSSION
CD was first described by Dr. Benjamin Castleman in the year 1956, when he studied a group of patients with large thymoma like masses in the anterior mediastinum [1]. Although the involvement of CD is commonly seen in the mediastinum, neck, axilla, the shoulder region, the pelvis, pancreas, nasopharynx and the retroperitoneum, mesenteric CD is rare. This disease is more common in adults but it can be seen in children also [2].
The aetiology of CD is not properly known and is characterized by a lymphoid hyperplasia which mimicks lymphoma. It involves the hyper proliferation of certain B cells which produce cytokines. Castleman’s disease can be classified as a) unicentric or multicentric, based on the clinical and the radiological findings, b) as of the hyaline vascular or plasmacytic or mixed cellularity variety, based on the histopathology and c) as HIV negative or HIV positive based on the HIV status of the patient. Pathologically, CD can be of a hyaline 574vascular variant, a plasma cell variant and of mixed types [3].
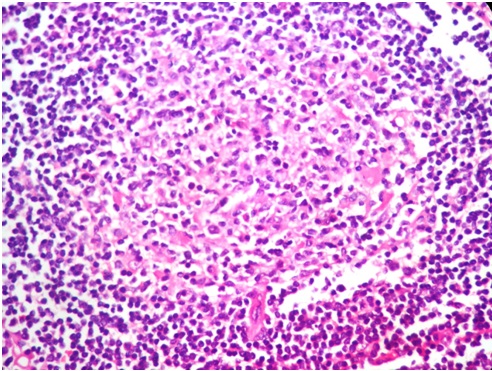
The hyaline vascular type exhibits a prominent proliferation of the small hyalinized follicles, with a marked interfollicular vascular proliferation [Table/Fig-4]. The plasma cell type (10-20%) has hyper plastic germinal centres and sheets of plasma cells in the interfollicular region, with the proliferation of the blood vessels and the persistent sinuses, while a small per cent has a mixed histologic appearance with the features of both the hyaline vascular and the plasma cell subtypes.
Microscopic Features of Castleman’s Disease Showing Increased Vessels are Associated with Hyalinization
Radiologically, the findings of CD are not specific and the radiological studies without histopathological reports will not give a definite diagnosis. CT scans can show a well defined soft tissue density, and the hyaline vascular type is more contrast enhanced than the plasma cell type.
Unicentric CD is characterized by the growth of lymph nodes at a single site with few (associated with the pressure symptoms) or no symptoms. Excision of the lymph nodes is the gold standard treatment, although there are no reported cases of recurrence [4]. There was a case of unicentric mesenteric CD which was of the hyaline vascular type, which presented with chronic non-iron deficient anaemia, which resolved after an effective treatment of the CD [5].
Unicentric Castleman’s Disease (UCD) is most often an isolated benign lymphoproliferative disorder of young adults, that is unassociated with the HHV-8 infection and that is generally curable with surgical resection. The largest published series included 81 cases; approximately 90 percent were of the hyaline vascular variant 3.UCD may be associated with an increased risk of lymphoma. Multicentric CD is always symptomatic as a result of the elevated Interleukin-6 production and is associated with asthenia (65%) weight loss (67%) and fever (69%) [6] and with the POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal proteinuria and skin changes ).
The first case of multicentric CD was reported in 1978 [7]. Multicentric CD is usually a plasma cell variant and it is a systemic disease with generalized peripheral lymphadenopathy, hepatosplenomegaly, frequent fever, and night sweats. The multicentric type is associated with AIDS and the human Herpes virus 8- related infections. Many patients have been reported to die of the progressive disease with multi-organ system failure. No standard treatment for multicentric CD has been advocated. But a combined treatment of surgery, chemotherapy and corticotherapy is being tried [8,9].
The symptoms of Hodgkin’s disease and lymphoma can mimick those of Castleman’s disease. In Hodgkin’s disease, the symptoms may include fever, night sweats, weight loss, and/or enlarged or swollen lymph nodes. The tumours occur most often in the chest, stomach, or the spleen. Hodgkin’s disease is usually progressive and it may spread to involve the lymph nodes which are located in other areas of the body. Malignant lymphomas generally occur in the chest and/or the stomach. The symptoms which are common to all forms of malignant lymphomas include fever, excessive sweating at night, weight loss, and/or an enlarged liver and/or spleen (hepatosplenomegaly). Both the conditions can be evaluated and differentiated by a histopathological confirmation.
[1]. Castleman B, Towne VW, Case records of the Massachuetts General Hospital. Case 40011N Engl J Med 1954 250:26-30. [Google Scholar]
[2]. Wei BP, Taylor R, Chan YF, Waters K, Alex G, Mesenteric Castleman’s disease in childhoodANZ J Surg 2004 74:502-04. [Google Scholar]
[3]. Keller AR, Hochholzer L, Castleman B, Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locationsCancer 1972 29:670-83. [Google Scholar]
[4]. Ushio T, Yoshimura K, Kojima A, A case of Castleman’s disease that recurred nine years after initial surgical removalNippon Kyobu Shikkan Gakkai Zasshi 1994 32:1175-80. [Google Scholar]
[5]. Bejjani Jimmy, Lemieux Bernard, Gariepy Gilles, Younan Rami, Complete anemia reversal after surgical excision of mesenteric hyalinevascular unicentric Castleman’s disease – A case noteCan J Surg October. 2009 52(5):E197-198. [Google Scholar]
[6]. Sarrot-Reynauld F, Castleman’s diseaseOrphanet Encyclopaedia August. 2001 [Google Scholar]
[7]. Gaba AR, Stein RS, Sweet DL, Variakojis D, Multicentric giant lymph node hyperplasiaAm J Clin Pathol 1978 69:86-90. [Google Scholar]
[8]. Bowne WB, Lewis JJ, Filippa DA, Niesvizky R, Brooks AD, Burt ME, Cancer 1999 85:706-17. [Google Scholar]
[9]. Herrada J, Cabanillas F, Rice L, Manning J, Pugh W, The clinical behavior of localized and multicentric Castleman’s diseaseAnn Intern Med 1998 128:657-62. [Google Scholar]