Vascular Leiomyoma of Foot
Suhith Gajanthodi1, Rakesh Rai2, Rajeev Kumar Chaudhry3
1 Assistant Professor, Department of General Surgery,
2 Associate Professor, Department of General Surgery,
3 Assistant Professor, Department of General Surgery.
NAME, ADRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Suhith Gajanthodi, Assistant Professor, Dept of General Surgery, Fr. Muller Medical College, Kankanady, Mangalore-575002
Phone: 0824 2221166, 9886875822, 0824 2238000 Email:suhith@rediffmail.com
Vascular leiomyomas of the foot are relatively rare benign soft tissue tumours which arise from the tunica media and present as painful or painless solitary subcutaneous nodules. We are reporting a rare case of vascular leiomyoma with a dystrophic calcification and a myxoid change.
Extremity Swelling, Calcification, Angioleiomyoma
INTRODUCTION
Angioleiomyoma or vascular leiomyoma, a benign, rare tumour of smooth muscle origin, generally arises from the tunica media of the small veins and arteries [1]. Although they are most frequently reported in the lower extremity and in middle-aged female patients, angioleiomyomas can be found throughout the body in male and female adults of all ages [1–6]. The diagnosis of a leiomyoma is frequently delayed due to its rare occurrence and due to the lack of awareness of the treating physicians [7]. This study has described a case of swelling over the foot. A surgical excision confirmed it to be a angiolieomyoma. This study has also reviewed the pathological aspects of this rare lesion.
CASE REPORT
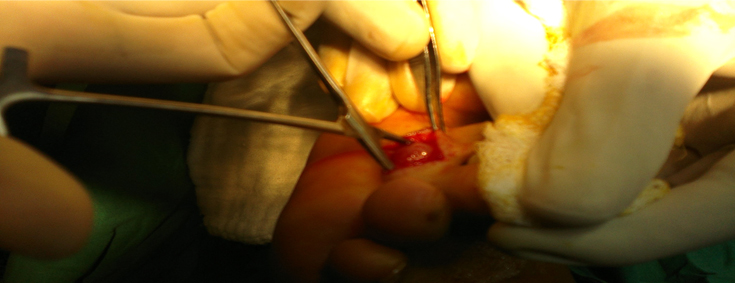
A 44 years old male presented with the chief complaint of a swelling in the plantar aspect of the left foot, which was there since 3 months. The swelling was painless and it produced discomfort only on walking and wearing footwear. On examination, a solitary oval swelling in the plantar aspect, just proximal to the 2nd web space, which measured 1.5*2 cm, which was nontender, minimally mobile, hard in consistency and in the subcutaneous plain, was noted [Table/Fig-1]. Differential diagnoses of lipoma, a dermoid cyst and a ganglion were considered and the patient underwent an excision biopsy of the lesion [Table/Fig-2].
Swelling just proximal to 2nd webspace.

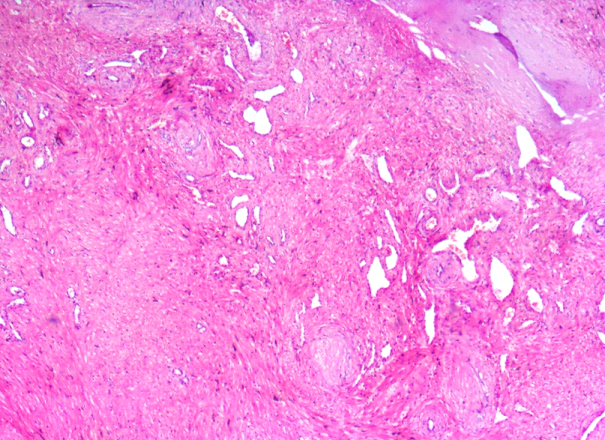
The histological examination revealed a tumour which was composed of numerous thick walled blood vessels, with ecstatic, partially patent and compressed lumens. The outer smooth muscle layer was found to swirl away from the vessels and to merge with the peripheral smooth muscle fibres. Focal areas of a myxoid change and a dystrophic calcification were also noted [Table/Fig-3]. This confirmed a diagnosis of a vascular leiomyoma or angioleiomyoma. The patient had a uneventful recovery and the clinical follow up of the patient revealed no local recurrences.
Intersecting and interfacing fascicles of smooth muscle.
DISCUSSION
A leiomyoma is a benign smooth muscle neoplasm that frequently occurs in the extra-skeletal sites which include the ovaries, uterus, bladder, lung and the gastrointestinal tract. Sometimes the skin and the subcutaneous soft tissues are involved, as in the vascular
leiomyomas which arise from the small blood vessels of the smooth muscle. The tumour rarely arises from the periosteal membrane or from bone [8].
A vascular leiomyoma usually occurs as a solitary subcutaneous lesion, with a predilection for the lower extremities of middle-aged women [2–6]. The most common anatomical site is the lower extremity, followed by the upper extremity, the head and the trunk [9]. Leiomyomas are divided according to their origins into 3 different types: piloleiomyomas, angioleiomyomas and genital leiomyomas. The piloleiomyomas are the most frequent types, which originating from the arrector pili muscles, whereas the angioleiomyomas arise from the vascular smooth muscles and the genital leiomyomas arise from the smooth muscles of the vulva, scrotum and the nipples [10]. Clinically, the most common complaint which is associated with a vascular leiomyoma is a painless swelling or a slightly tender tumour mass [11, 12]. Its growth is usually slow and it may have grown for years before a patient seeks medical evaluation. If the tumour is located in the feet, fitting on shoes may be a problem [1]. Pain, with or without tenderness, exists in approximately 60% of the patients [4]. Although a majority of these tumours are small, ranging from 0.5 to 2 cm in diameter, they frequently grow larger. The vascular leiomyomas arise commonly in the deep layers of the dermis, or in the subcutaneous tissues. The tumour is generally rounded and it forms a nodule that usually elevates the skin [5].
Four histological subtypes of angioleiomyomas 4 have been described, namely:
Capillary or solid angioleiomyomas which have a rich smooth muscle cell stratification which surround and hold a few thin vascular channels,
Venous angioleiomyomas which are characterized by more numerous and thicker vascular channels than are found in capillary angioleiomyomas,
Cavernous angioleiomyomas which have widened vascular channels which are surrounded by a thin layer of smooth muscle cells,
Combined capillary and venous angioleiomyomas [4].
Complications like secondary calcification, myxoid degeneration, hyalinization, and malignant transformation have been reported. The angioleiomyomas on the acral sites which show extensive calcification have been reported, and the term “acral calcified vascular leiomyoma of the skin” was proposed for this rare, clinicopathological variant of angioleiomyomas. The sites were in the acral regions such as the index finger, the sole and the heel [13,14]. The dystrophic calcification has been reported to occur due to a minor pressure, an injury, a previous inflammatory process, or de novo. Although the pathogenesis of the diffuse calcification in angioleiomyomas is obscure, the tumours in the acral areas may be susceptible to calcification due to minor, repetitive injuries [15]. Areas of a myxoid change and hyalinization are sometimes present [4]. Vascular leiomyomas must also be differentiated from fibromas, lipomas, glomus tumours, ganglions, neurilemmomas and leiomyosarcomas. However, because of the lack of specificity of clinical and sonographic findings for the differentiation of soft tissue masses, biopsy remains the reference standard if a clinical uncertainty exists [16]. The therapeutic approach depends on the size of the lesion and the severity of the symptoms. Surgical excision is the treatment of choice for the solitary leiomyomas. A drug treatment with nifedipine, gabapentin and antidepressants can be undertaken in the cases where the tumours are both numerous and painful [10].
CONCLUSION
Although angioleiomyoma is an infrequent soft tissue tumour, it has a typical nonspecific presentation. It has to be considered in the differential diagnosis of subcutaneous swellings, especially in the extremities. Excision of the lesion and the histopathology give a definitive diagnosis and a complete resolution of the symptoms in the patient.
[1]. Duhig JT, Path D, Ayer JP, Vascular Leiomyoma: A Study of 61 CasesArch Pathol 1959 68:424-30. [Google Scholar]
[2]. Myhre-Jensen O, A Consecutive 7-Year Series of 1331 Benign Soft Tissue Tumors: Clinicopathologic Date: Comparison with SarcomasActa Orthop Scand 1981 52:287-93. [Google Scholar]
[3]. Kinoshita T, Ishii K, Abe Y, Naganuma H, Angiomyoma Of The Lower Extremity : Mr FindingsSkeletal Radiol 1997 26:443-45. [Google Scholar]
[4]. Hachisuga T, Hashimoto H, Enjoji M, Angioleiomyoma: A Clinicopathologic Reappraisal of 562 CasesCancer 1984 54:126-30. [Google Scholar]
[5]. Stout AP, Solitary Cuteneous and Subcutaneous LeiomyomaAm J Cancer 1937 29:435-69. [Google Scholar]
[6]. Freedman AM, Meland NB, Angioleiomyomas Of The Extremities: Report Of A Case And Review Of The Mayo Clinic ExperiencePlast Reconstr Surg 1989 83:328-31. [Google Scholar]
[7]. Di Caprio Mr, Jokl P, Vascular Leiomyoma Presenting As Medial Joint Line Pain Of The KneeArthroscopy 2003 19(3):E24 [Google Scholar]
[8]. Turhan-Haktanir N, Haktanir A, Demir Y, Tokyol C, Acar M, Toe Leiomyoma. A Case Report With Radiological CorrelationActa Chir Belg 2006 106:92-95. [Google Scholar]
[9]. Ramesh P, Annapureddy SR, Khan F, Sutaria PD, Angioleiomyoma: a clinical, pathological and radiological reviewInternational Journal of Clinical Practice 2004 58(6):587-91. [Google Scholar]
[10]. Miranda LQ, Rehfeldt FV, Souto da Silva R, Case for diagnosisAn. Bras. Dermatol. Rio de Janeiro ar./Apr. 2012 87(2) [Google Scholar]
[11]. Callé SC, Eaton RG, Littler JW, Vascular leiomyomas in the handJ Hand Surg [Am] 1994 19:281-86. [Google Scholar]
[12]. Lawson GM, Salter DM, Hooper G, Angioleiomyomas of the hand. A report of 14 casesJ Hand Surg (Br) 1995 20:479-83. [Google Scholar]
[13]. Maheshwari AV, Temple HT, Murocacho CA, Calcified Angiomyomas Of The Foot: A Case ReportFoot Ankle Int 2008 29:449-55. [Google Scholar]
[14]. Kacerovska D, Michal M, Kreuzberg B, Mukensnabl P, Kazakov DV, Acral Calcified Vascular Leiomyoma Of The Skin: A Rare Clinicopathological Variant Of Cutaneous Vascular LeiomyomasJ Am Acad Dermatol 2008 59:1000-04. [Google Scholar]
[15]. Sakai E, Asai E, Yamamoto T, Acral Calcified AngioleiomyomaEur J Dermatol 2010 20(1):121-22. [Google Scholar]
[16]. Smith J, Wisniewski SJ, Lee RA, Sonographic And Clinical Features Of Angioleiomyoma Presenting As A Painful Achilles Tendon Mass Jum. 2006 25(10):1365-68. [Google Scholar]