A Secondary Carcinomatous Lesion Masquerading as A Primary Osteosarcoma - A Case Report
Thamilselvi Ramachandran1, P. M. Subramanium2, K. Prakasam3
1 Professor, Department of Pathology,
2 Professor, Department of Pathology,
3 Professor, Department of Orthopedics, Vinayaka Mission’s Kirubanada Variyar Medical College & Hospital, India.
NAME, ADRES, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Thamilselvi Ramachandran, Professor, Department of Pathology, 32/2, Ashok Nagar II Street, Narajothipatty, Salem-4, India.
Phone: 09842744313
E-mail: drselvipatho@yahoo.com
Penile carcinomas account for 10% of all the malignancies in men with a predominant regional lymph node involvement, but a distant metastasis of such a carcinoma via the haematogenous route is rare (2.3%), with the common sites being the kidneys, adrenal glands, retroperitoneal lymph nodes, lungs, brain and the dorsal spine.
The pattern of the metastatic spread from carcinomas of the penis has been well described in the literature, with the inguinal and the iliac nodes being the commonest sites. The distant metastases are uncommon and delayed, even in advanced disease. Although metastases to the liver and lungs have been reported, the osseous metastases are exceptionally rare. We are presenting a case of carcinoma of the penis which metastasized to the tibia.
Penile carcinoma, Osteosarcoma & Squamous cell carcinoma
CASE REPORT
A 45 years male presented with a right knee swelling and pain of 3 months duration. On examination , a fungating, red, indurated penile growth with palpable right inguinal nodes were found. An X-ray of the right knee [Table/Fig-1] showed an osteolytic lesion [Table/Fig-2] with a soft tissue extension and a provisional diagnosis of an osteosarcoma was given. The chest X- Ray was normal. Ultrasonography of the abdomen did not reveal any lymph node enlargement.
X-Ray right knee – osteolytic lesion with soft tissue extension

Clinical Examination - fungating, red, indurated penile growth

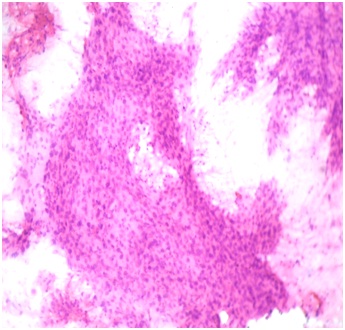
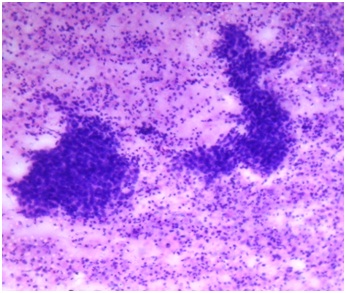
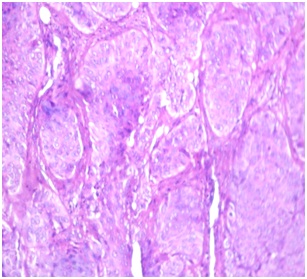
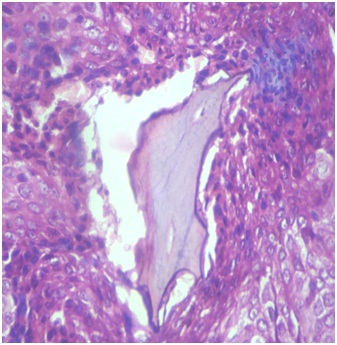
Computerized Tomography (CT) scan of the abdomen and pelvis did not show any metastatic deposits. FNAC of the right inguinal lymph node [Table/Fig-3] revealed secondary squmaous cell carcinomatous deposits and an imprint smear [Table/Fig-4] of the glans penis was positive for malignant cells. Later, wedge biopsies from the penile growth [Table/Fig-5] and a bone biopsy [Table/Fig-6] were done and they were sent for a histopathological examination.
FNAC of Inguinal Lymph node - Clusters of Malignant cells (H&E, 10X)
Imprint smear of Penile discharge– Clusters of Malignant cells (H&E,10X)
Histopathology of Penile growth – Non keratinising Squamous cell carcinoma (H&E, 40X).
Bone biopsy showed osteoid and Malignant squamous cells (H&E, 40X)
Macroscopic Appearance: Multiple, grey white, soft tissue bits from the penile growth and bony fragments from the tibia were received and each measured 2x1x1cm.
Microscopic appearance: The penile growth biopsy showed a moderately differentiated squamous cell carcinoma and the bone biopsy revealed a metastatic squmaous cell carcinoma.
DISCUSSION
Penile carcinoma is mainly a localized disease (39%), with carcinoma-in-situ making up 37% of the total penile carcinoma cases and regional disease making up 13% of the cases .The incidence of penile carcinoma is higher in the developing countries as compared to that in the developed countries. The incidence of cancer of the penis (5.9%) is also similar (7.84%) in Rajasthan, India [1] and (3.59%) in Mumbai [2]. It tends to occur in the elderly and most commonly on the glans penis (48%), then on the prepuce (25%), then both on the glans and the prepuce (9%), on the coronal sulcus (6%) and on the shaft (<2%). Ninety-five percent of these malignancies are squamous cell carcinomas.
The metastasis of carcinoma of the penis occurs predominantly through the lymphatic channels by a lymphatic embolization [3] and the ilio-inguinal nodes are the first to be involved, followed by the para-aortic lymph nodes [4]. The size and the site of the lesion or the grade of the tumour do not significantly affect the metastatic potential. However, the involvement of greater portions of the penis by the tumour has been found to increase the risk of metastatic disease [4]. The clinically detectable distant metastases are rare, with a reported incidence of 1-10% [3,4,5] and the distant metastases which occur via the haematogenous route are still rare (2.3%). However, the mean life span of those with distant metastases is 7.4 months’.
Metastasis to the kidneys, adrenal glands, the retroperitoneal lymph nodes, lungs, brain and the dorsal spine’” have been reported in the literature, but not to the long bones. Riveros and Gorostiaga 1 reported a metastasis to the iliac bone in one patient, and to the skin of the neck in another case. Another report of osseous metastases from a penile carcinoma to the ischial bone, was published by Gun’ko and Fomin [5]. According to us, this is the first case of carcinoma of the penis which metastasized to the tibia, which is being reported. Buck’s fascia acts as a natural barrier and the penetration of Buck’s fascia allows the involvement of the corporal bodies and a rapid dissemination. It has a progressive course and no case of spontaneous remission has been reported. In the untreated cases, most commonly death occurs due to the erosion of a femoral vessel.
The survival in penile carcinoma correlates with the presence or absence of the nodal disease. The five-year survival rates for the patients with a node-negative disease range from 65-90%, with positive inguinal nodes, this rate decreases to 30-50% and with positive iliac nodes, it further decreases to less than 20%. However, in the presence of soft-tissue or bony metastases, the 5-years survival has not been reported.
CONCLUSION
Although the incidence of carcinoma of the penis is 10% and it metastasizes predominantly to the regional lymph nodes, the distant metastases are extremely rare. The present case highlights a unique clinical manifestation of penile cancer as a bony metastasis, which caused an osteolytic lesion in the tibia, which clinically and radiologically mimicked osteosarcoma. This case has been presented for its rarity.
[1]. Sharma RG, Ajmera R, Saxena O, Cancer profile in eastern RajasthanInd Jour Cancer Sept. 1994 31:160-73. [Google Scholar]
[2]. Jussawala DJ, Yeole BB, Natekar MV, Sunny L, Cancer incidence and mortality in Greater BombayIndian Cancer Society. Mumbai 1995 :13 [Google Scholar]
[3]. Riveros M, Gorostiaga R, Cancer of the penisArch. Surg 1962 85:377-82. [Google Scholar]
[4]. Staubitz WJ, Melbourne HL, Oberkircher OJ, Carcinoma of the penisCancer 1955 8:371-78. [Google Scholar]
[5]. Gun’ko R I, Fomin S D, Metastasis of penile cancerto ischial boneMed. Radioi. (Mosk) 1989 34:75 [Google Scholar]