Carcinosarcoma of the Gallbladder: A Case Report and Review of the Literature
Menka Khanna1, Ashish Khanna2, Mridu Manjari3
1 Associate Professor, Pathology, Sri Guru Ram Das Institute of Medical Sciences.
2 Associate Professor, Microbiology, Sri Guru Ram Das Institute of Medical Sciences.
3 Professor and Head Pathology Department, Sri Guru Ram Das Institute of Medical Sciences.
NAME, ADRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ashish Khanna, 538, Basant Avenue, Amritsar 143001, Punjab, India.
Phone: 9465128936 , 0183-2562919
E-mail: ashish_538@yahoo.co.in
A carcinosarcoma is a rare type of gallbladder malignancy, the diagnosis of which requires the presence of both malignant epithelial and mesenchymal components. The prognosis of this disease is extremely poor because it normally presents at advanced stages.We are reporting a case of carcinosarcoma of the gallbladder in a 45 year-old woman who was treated by cholecystectomy, as the tumour was confined to the gall bladder only.
Gall bladder, Carcinosarcoma
INTRODUCTION
Carcino Sarcoma of Gall Bladder (CSGB) is an extremely rare neoplasm and it is characterized by the presence of both carcinomatous and sarcomatous components. The occurrence of the tumour in many different organs which include the uterus, lung, oesophagus, kidney and pancreas is well known [1]. However, the gallbladder is a rare site, with only 34 cases being reported in the English literature till date [2]. A vast majority of the gallbladder (GB) cancers are adenocarcinomas, with carcinosarcomas accounting for fewer than 1% of the tumours [3]. The invasive nature and the aggressive biology of CSGB adequately explains the limited number of resectable cases.
CASE REPORT
A 45-year-old woman presented with a 10 days history of severe
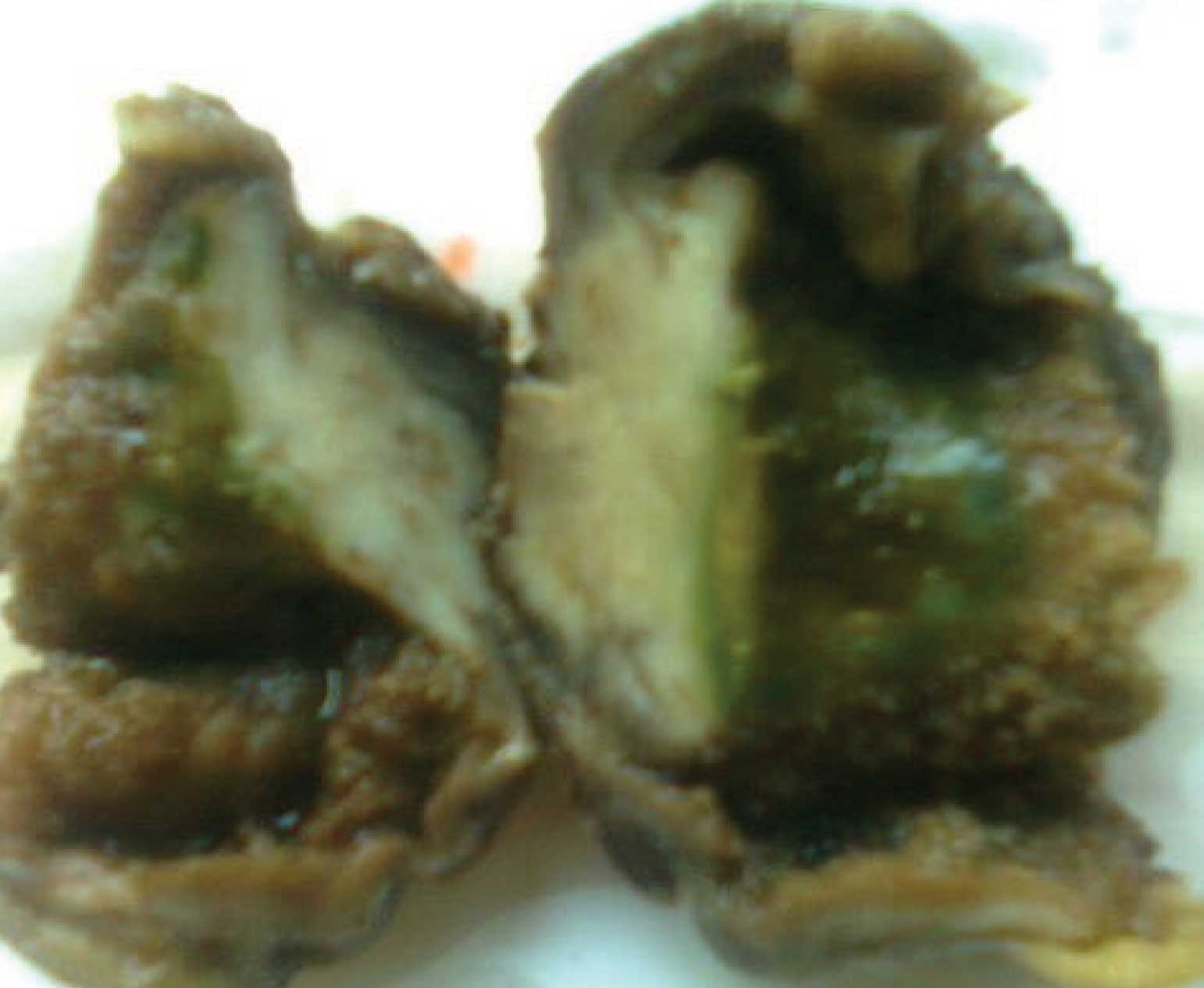
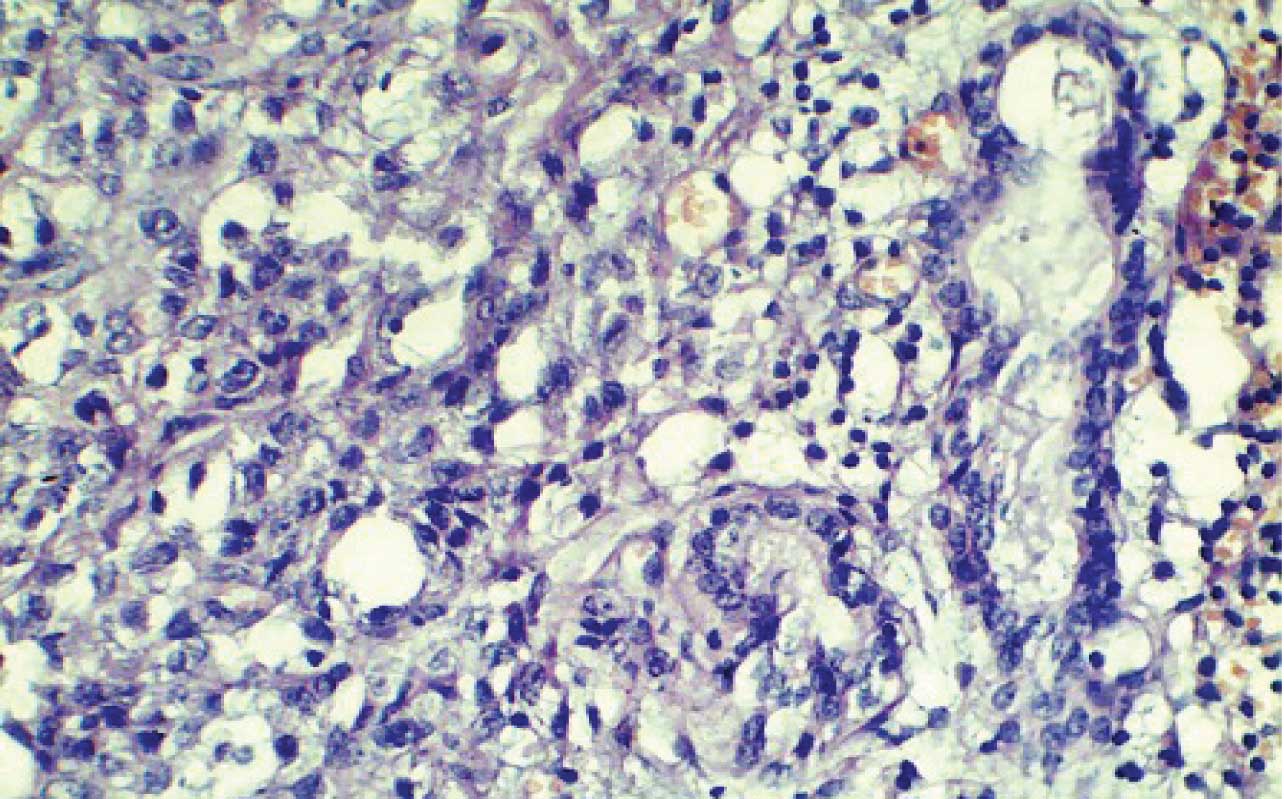
pain in the right hypochondrium.There was no history of fever, vomiting, anorexia or weight loss. There was also no history of gastro-intestinal bleeding or the features of a gastric outlet obstruction. The liver was non-palpable and there was no free fluid in the abdomen. Her per rectal examination was normal. Her laboratory examinations showed haemoglobin of 9.5g/dl, a normal leukocyte count, and normal liver function tests. Her ultrasonographic examination showed a small hypoechoic mass in the posterior wall of the gall bladder. Her computed tomographic scan showed a mild, irregular thickening of the gall bladder wall, in the region of the fundus and the posterior wall, along with a small and an ill defined hypodense mass in the wall.There was no evidence of distant metastases, ascites, or lymph node enlargements in the porta, pericholedochal, retro-portal or the coeliac areas. A preoperative diagnosis of a gallbladder malignancy was made. A laparotomy and a simple cholecystectomy, with a wedge resection of the underlying liver tissue and the pericholedochal lymph nodes were performed and the specimens were sent for histopathology. On gross examination, the gallbladder was found to measured 6x4cm and the external surface was slightly congested and smooth, with the liver tissue being attached on one side. The cut section showed an ulcerated lesion in the mucosa, which measured 2.5cm x1.5cm in the region of the fundus and the body. The ulcer had a thickened and an indurated base with raised edges. The cut Manjarisection, through the ulcer, showed a firm, solid and a grayish white mass which underlay it , which appeared to be infiltrating the entire thickness of the gall bladder wall, with no outer extension [Table/Fig-1]. Microscopically, the sections from the mass showed a tumour which was composed predominantly of sarcomatoid areas with focal carcinomatous components. The sarcomatoid areas showed fascicles of spindle-shaped cells which exhibited a nuclear pleomorphism with a focal carcinomatous element in the form of few scattered glands [Table/Fig-2].
Greyish white mass underling the ulcer and infiltrating the gall bladder wall
Focal carcinomatous component as few scattered glands lying amidst spindle cell sarcomatous areas (H&E,X400)
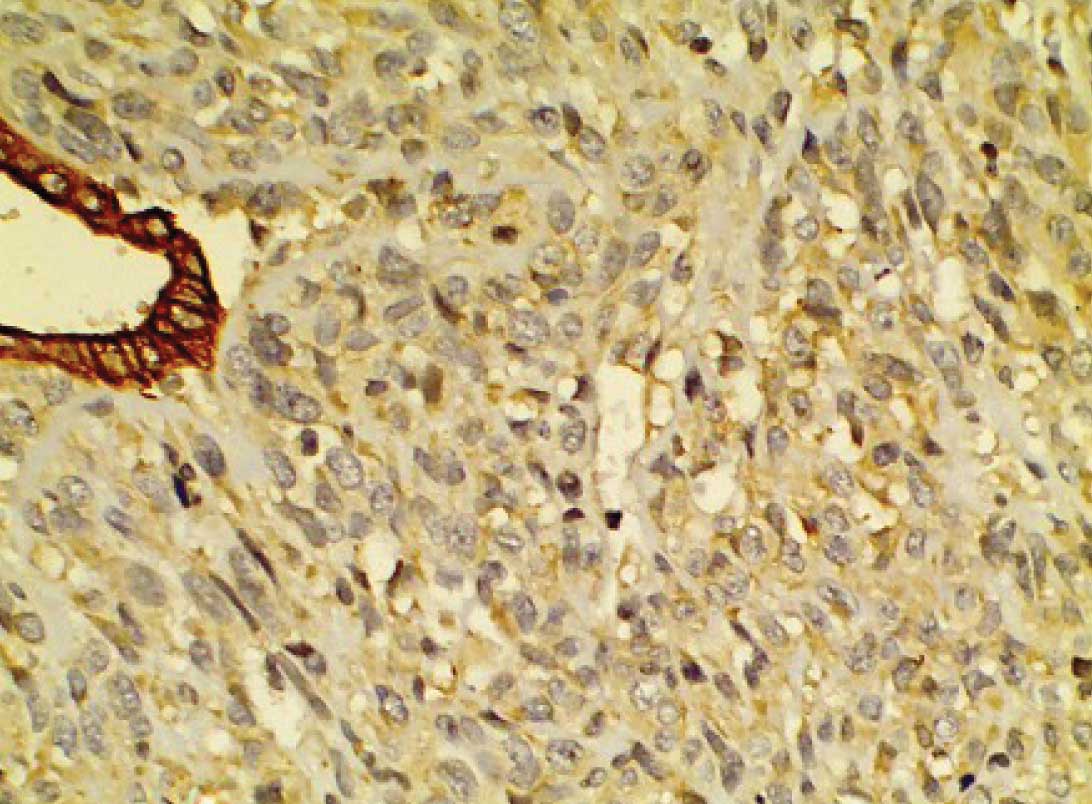
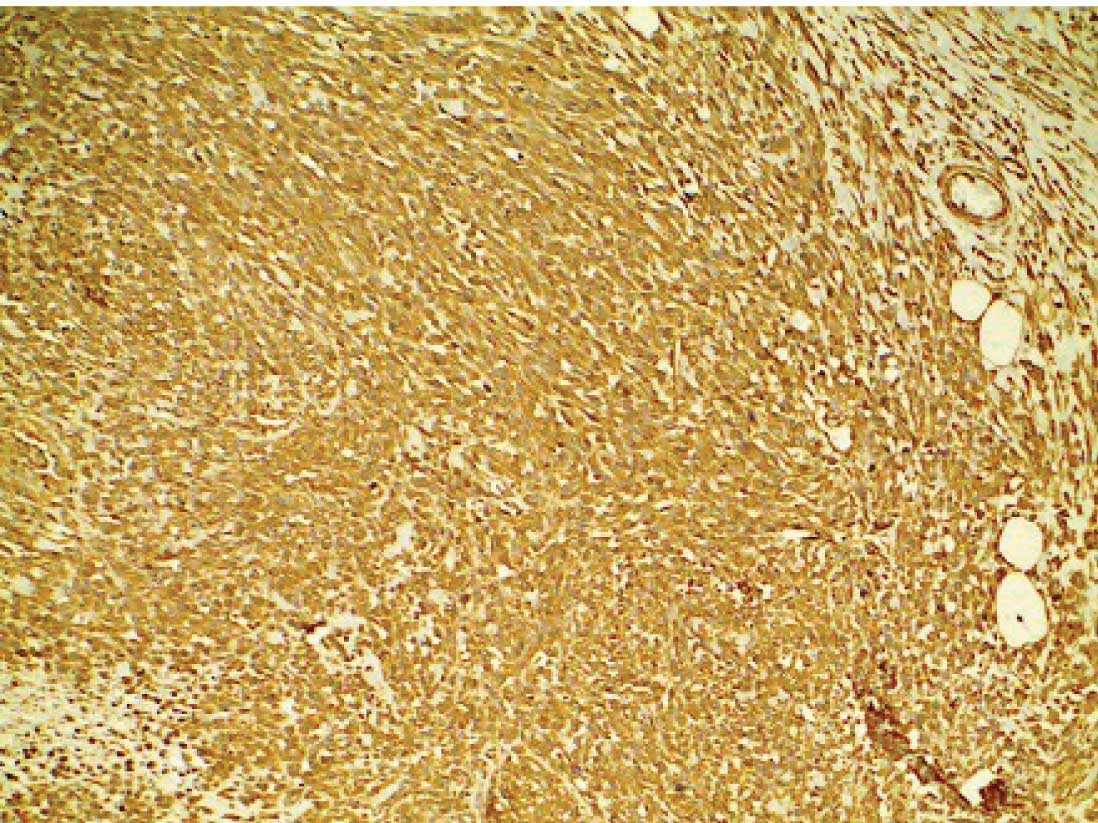
Heterologous sarcomatous elements were not seen. The tumour was found to infiltrate across the muscularis propria, but the serosa, liver and the resected lymph nodes were free of its infiltration. On immunohistochemistry, the sarcomatoid areas were found to be strongly positive for vimentin and to be negative for cytokeratin.The carcinomatous areas were positive for cytokeratin and negative for vimentin [Table/Fig-3 and 4]. The postoperative recovery was uneventful. The patient was asymptomatic for six months after the treatment.
Strong cytokeratin positivity in malignant glands forming the epithelial component (Cytokeratin×400).
Strong vimentin positivity in the sarcoma component (Vimentin, ×400).
DISCUSSION
Carcinosarcoma of the gallbladder is a rare tumour, with only 34 cases being reported in the English literature [2]. It is characterized by a malignant trasformation of both the epithelial and the mesenchymal components of the same tissue. Its diagnosis requires the presence and the intermingling of both the histological components [4]. Born et al., reported one case of carcinosarcoma of the gallbladder among 99 cases of primary gallbladder malignancies who were admitted to St Luke’s Hospital in New York City, over an 18-year period from 1964 to 1981 [5].
Several theories have been proposed to explain the admixture of the epithelial and the mesenchymal tissues in these neoplasms: (1) a mesenchymal reaction, (2) a true sarcoma (including the collision neoplasm hypothesis), (3) a malignant proliferation of epithelial origin (including the stromal induction/metaplasia model), (4) an embryonic cell rest origin, and (5) the totipotential stem cell hypothesis. The sarcomatous change of a carcinoma can be induced by radiotherapy, alterations to the p53 gene, and production of the bone morphogenetic protein by cancer cells. On the other hand, it has been speculated that these neoplasms arise from totipotential stem cells, the rest cells of the myoblasts that retain the capability of a transformation, the primitive undifferentiated mullerian stroma, or from paramesonephric tissue [4].
In a majority of the cases, a well to poorly differentiated adenocarcinoma comprises the carcinomatous element. There is occasionally a component of a squamous cell carcinoma or a squamous metaplasia. The sarcoma like portion consists of undifferentiated stellate and spindle-shaped cells which are variably admixed with foci which resemble an osteosarcoma, a chondrosarcoma or a rhabdomyosarcoma [6].
In our case, the tumour was mainly composed of spindle cell sarcomatous areas. An extensive sampling and a diligent search was done to find any carcinomatous areas and thus to rule out its pure mesenchymal origin.The focal carcinomatous area was composed of an adenocarcinoma which was positive for cytokeratin and negative for vimentin,whereas the spindle cell sarcoma component was negative for cytokeratin and positive for vimentin.
An accurate preoperative diagnosis of CSGB is very difficult because imaging studies cannot differentiate it from carcinoma of the gall bladder. An abdominal angiography often shows neovascularity and staining of, whereas Computed Tomography (CT) shows an enhanced solid mass lesion. The differential diagnosis includes gall bladder carcinoma when there is calcification, calcified gall stones, or a porcelain gall bladder, and a carcinosarcoma of the gall bladder is suspected when a calcification is observed within the tumour on CT examination. However, more detailed imaging data are needed to improve the diagnosis of CSGB. It is not associated with specific radiological findings or serum data, which include tumour markers [6].
Zhang et al, in their study, reported that tumours which were smaller than 5 cm had a longer survival and that therefore, the tumour size should be considered as a major component in the future staging system for CSGB, although genetic variations, an earlier detection of CSGB (stage I or stage II) and a more extensive surgery could also contribute to a better prognosis. They also indicated that the presence of gallstones, epithelial and mesenchymal component types, age and sex were of little prognostic value [7]. The best treatment option for CSGB is surgical excision. Cholecystectomy alone is sufficient for the cancer cells which are confined to the lamina propria, whereas the more advanced states require the resection of a 3 to 5 cm wedge of the liver tissue at the gallbladder bed, combined with a Lymph Node (LN) dissection in the absence of an evidence of a distant metastasis. The 5-year survival rate after a curative resection for CSGB is 88.9%, when the invasion is restricted to the muscularis propria.CSGB may recur as a liver metastasis, a peritoneal dissemination, or as a LN metastasis.The therapeutic interventions have not been well defined and no optimal postoperative adjuvant therapy such as chemotherapy and radiotherapy has been established, because of the rarity of CSGB and its poor prognosis [8].
An extensive sampling and a careful search for various carcinomatous and sarcomatous elements are mandatory for making an accurate diagnosis, to decide the appropriate clinical management and to try and improve the prognosis.
[1]. Oberoi R, Jena A, Tangri R, Saharia A, Carcinosarcoma of the gallbladder with chondroid differentiation: MRI findingsIndian Journal of Radiology and Imaging 2006 16(4):491-93. [Google Scholar]
[2]. Uzun MA, Koksal N, Gunerhan Y, Celik A, Gunes P, Carcinosarcoma of the gallbladder: report of a caseSurg Today 2009 39(2):168-71. [Google Scholar]
[3]. Huguet KL, Hughes CB, Hewitt WR, Gallbladder carcinosarcoma: a case report and literature reviewJ Gastrointest Surg 2005 9:818-21. [Google Scholar]
[4]. Okabayashi T, Sun Z-L, Montgomery RA, Hanazaki K, Surgical outcome of arcinosarcoma of the gall bladder: A ReviewWorld J Gastroenterol 2009 15(39):4877-82. [Google Scholar]
[5]. Al-Sheneber IF, Jaber T, Huttner I, Arseneau J, Loutfi A, Carcinosarcoma of the gallbladder: a case report and review of literatureThe Saudi Journal of Gastroenterology 2002 2(1):22-24. [Google Scholar]
[6]. Kim MJ, Yu E, Ro JY, Sarcomatoid Carcinoma of the Gallbladder with a rhabdoid tumor componentArch Pathol Lab Med 2003 127:e406-8. [Google Scholar]
[7]. Zhang L, Chen Z, Fukuma M, Prognostic Significance of Race and Tumor Size in Carcinosarcoma of Gallbladder: a Meta-Analysis of 68 CasesInt J Clin Exp Pathol 2008 1:75-83. [Google Scholar]
[8]. Park SB, Kim YH, Rho HL, Primary carcinosarcoma of the gallbladderKorean Surg Soc 2012 82:54-58. [Google Scholar]