Dedifferentiated liposarcoma is one of the variants of liposarcoma which has a more aggressive course. It constitutes less than 10% of all the liposarcomas and is often found in the retroperitoneum and the mediastinum.
We are reporting a rare case of a 60 years old female who presented with a huge, soft tissue mass in the left thigh with a past history of an operation which was done15 years back. The histopathological examination showed a well differentiated liposarcoma with a high grade fibrosarcomatous differentiation. Immunohistochemical studies confirmed the dedifferentiated liposarcoma with the high grade fibrosarcomatous differentiation. To the best of our knowledge, this is the 11th case in the literature with rare findings.
INTRODUCTION
Liposarcoma is one of the most common soft tissue sarcomas of the adult life, which ranges from 16-18% of all the soft tissue sarcomas [1]. According to the World Health Organization (WHO), liposarcomas are generally classified into five subtypes: well differentiated, myxoid, round cell, dedifferentiated and pleomorphic [1].
The term dedifferentiated liposarcoma was first used by Harry Evans [2] in 1979 to define the transition from a low grade to a high grade nonlipogenic morphology within a well differentiated liposarcoma. The concept of dedifferentiation had been previously introduced by David Dahlin in the context of the description of the tumour progression in chondrosarcoma [3]. In the 2002 WHO classification, it was specified that the nonlipogenic areas may not be necessarily high grade [3].
The well differentiated and the dedifferentiated liposarcomas commonly occur in the retroperitoneum, whereas the myxoid, round cell and the pleomorphic liposarcomas typically present in the extremities (thigh) [4]. Men are more frequently affected than women [3].
In this paper, we are reporting a huge dedifferentiated liposarcoma of the thigh with a high grade fibrosarcomatous differentiation and a local recurrence in a 60 year old female patient.
CASE REPORT
A 60 year old female patient presented to the surgical department of our hospital with the chief complaint of a huge swelling in the left thigh since 2 to 3 years. It was associated with pain and inability in taking up the routine daily activities. There was no history of trauma or any other illness. A past history of an operation at the same site 15 years back which was done by a local practitioner was obtained. (The records could not be traceable) She mentioned a gradual increase in the size of the mass since 2 to 3 years. The local examination revealed a huge mass which measured 30x20x18cms, in the medial aspect of the left thigh. The mass was multinodular and soft to feel, with the firm areas extending from the hip joint to the knee joint. The overlying skin was tense and the underlying bone appeared to be free from the mass. The haematological, biochemical and the serological parameters were within normal limits. The chest X-ray was within normal limits. Ultrasonography (USG) of the abdomen and the pelvis was unremarkable.
USG of the left thigh mass revealed a large, ill defined, soft tissue mass of a predominantly fatty architecture, which seemed most likely to be a liposarcoma. Spiral Computerized Tomography (CT) of the left thigh mass revealed a large, mixed signal intensity mass which was predominantly of a fat density, with irregular masses which measured 27x18x16cms, with focal cystic areas and calcifications, which compressed the muscles and without a femur involvement, which was suggestive of a neoplastic soft tissue mass –liposarcoma [Table/Fig-1].
Spiral CT image of left thigh mass showing large mixed signal intensity mass predominantly of fat density suggestive of neoplastic soft tissue mass

Fine Needle Aspiration Cytology (FNAC) of the mass was performed. The FNAC diagnosis was a malignant soft tissue tumour with a differential diagnosis of a liposarcoma or an intermediate grade myxofibrosarcoma. On the basis of all the above findings, a clinical diagnosis of liposarcoma was made and a wide excision of the left thigh mass was carried out with preservation of the muscles, vessels and the sciatic nerve. The resected specimen was sent for a histopathological examination. The postoperative period was uneventful.
Gross Examination: We received an excised specimen from the left thigh which consisted of a large, circumscribed, greyish yellow, soft tissue mass which measured 28x18x16cms and weighed 5.8kgs [Table/Fig-2]. The external surface was nodular and greyish yellow. The cut section showed a large greyish yellow mass with few mucoid areas, along with a variegated appearance [Table/Fig-3]. At places, it appeared to be fleshy with focal areas of calcification, haemorrhage and necrosis.
Gross appearance of excised left thigh mass showing large, circumscribed grey to yellow nodular tumor masses

Cut section showed large grey yellow mass with few mucoid areas along with variegated fleshy appearance and focal areas of calcification, hemorrhage and necrosis.

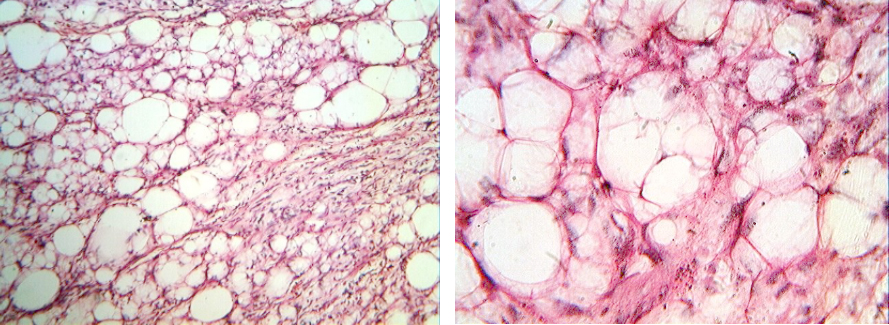
Light Microscopy: Multiple sections which were studied, showed a well differentiated liposarcoma which was arranged back to back with a spindle cell tumour [Table/Fig-4]. The lipogenic component was composed of fat cells of varying sizes which were separated by slender connective tissue septae. The neoplastic cells were uni or multivacuolated (lipoblasts) with moderately pleomorphic hyperchromatic nuclei, with a multivacuolated, clear cytoplasm [Table/Fig-5a and 5b] At places, the signet ring cell appearance of the tumour cells was noted. Areas of lipoma, sclerosis, calcification and haemorrhage were noted.
Light microscopy showed well differentiated Liposarcoma arranged back to back with a Spindle cell tumor (H &E stain, x100)
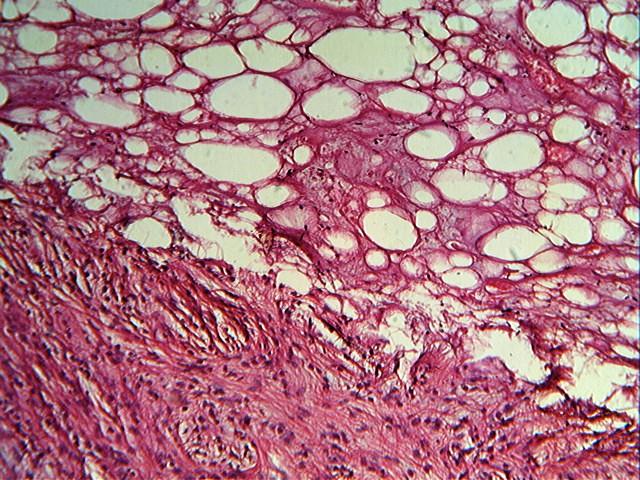
Lipogenic component composed of fat cells of varying sizes separated by slender connective tissue septae with uni or multivacuolated(lipoblasts) with moderately pleomorphic hyperchromatic nuclei with multivacuolated clear cytoplasm (H &E stain, x100 &x400)
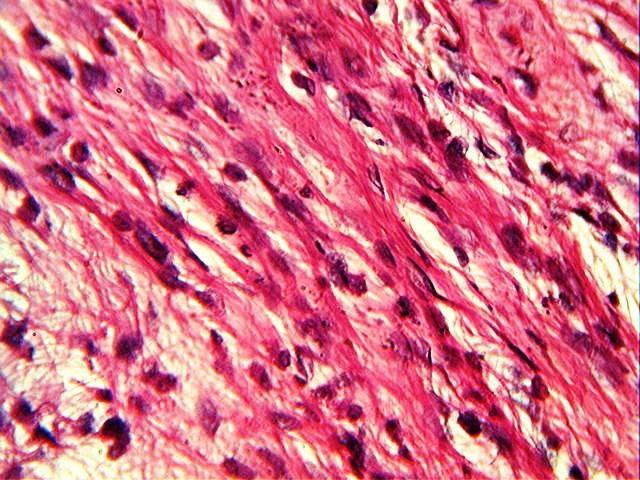
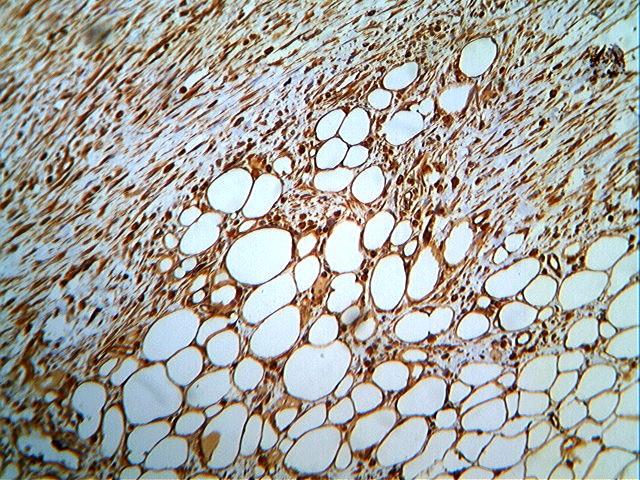
The nonlipogenic spindle cell component (dedifferentiated) was a fibrosarcoma which was arranged in interlacing bundles, sheets, clusters and a herringbone pattern. The nuclei showed moderate to marked pleomorphism with irregular, dispersed chromatin. [Table/Fig-6] The mitoses ranged from 9 to 10/10HPF. The stroma showed a focal dense infiltration with lymphocytes, plasma cells and eosinophils. Areas of haemorrhage and necrosis were noted. The final histopathological diagnosis given was a malignant soft tissue tumour-dedifferentiated liposarcoma with a high grade fibrosarcomatous differentiation. Immunohistological studies were carried out, which confirmed the diagnosis. The tumour cells showed a widespread cytoplasmic immunoreactivity for vimentin [Table/Fig-7] and a nuclear immunopositivity for MDM2 . The tumour cells were immunonegative for CK, EMA, SMA, desmin, muscle specific actin, caldesmon, S-100, myogenin and CD34. The Ki-67 proliferative index in the spindle cell component was 27%.
Dedifferentiated component-Fibrosarcoma showed moderate to marked pleomorphic nuclei with irregular dispersed chromatin (H &E stain, x400).
The tumor cells show widespread cytoplasmic immunoreactivity for vimentin (H &E Stain , x100)
DISCUSSION
Dedifferentiated liposarcoma comprises less than 10% of all the liposarcomas and it is found most often in the retroperitoneum and the mediastinum and rarely in the extremities, the spermatic cord and the head and neck [5]. This entity was first introduced by Evan [2] in 1979. Dedifferentiated liposarcoma is a biphasic, well differentiated liposarcoma with a high grade pleomorphic sarcoma, which occurs either as a primary, denovo complication or a secondary, late stage complication [6]. Henricks and collegues [7] analyzed 155 cases and proposed about expanding the definition to include the dedifferentiated liposarcomas which also contained areas of low grade dedifferentiation or low percentage dedifferentiation, as they exhibited the same behaviour as a fully malignant, high grade sarcoma. This is the definition which is used today [7].
Dedifferentiation is a histological form of tumour presentation. Its identification in the lipomatous tumours of the extremities may have significant implications in the management of the patients [6–8]. In general, dedifferentiated sarcomas are considered as high grade tumours, and the dedifferentiated component (rather than the fatty component) has a metastatic potential [8].
Dedifferentiation most commonly occurs within a well-differentiated liposarcoma in the retroperitoneum and the inguinal regions, but it may rarely be encountered in the deep soft tissues of the extremities [3], as in our case.
The dedifferentiated liposarcomas behave aggressively. They have a local recurrence rate of 41%, a metastatic rate of 17% and a disease related mortality of 28% [1,9]. The mortality is related to the uncontrolled local recurrences rather than to the metastatic spread [3].
Regarding the differential diagnoses, other pleomorphic sarcomas (most often pleomorphic leiomyosarcomas) that occur in the retroperitoneum, as well as nonsarcomatous lesions such as the sarcomatoid carcinomas should be keep in mind. A histopathological examination can differentiate these conditions and they can be further confirmed by immunohistochemistry [1,3].
The standard treatment for a dedifferentiated liposarcoma is a wide surgical excision. In the retroperitoneal location, the resection should include the adjacent viscera. In our case, a wide surgical excision with preservation of the vessels, muscles and the sciatic nerve was performed.
Dedifferentiated liposarcomas which occur outside the mediastinum, retroperitoneum or the inguinal are exceedingly rare. There are only 10 previous papers which are available in the literature either on the radiological or the pathological findings of dedifferentiated liposarcomas [5,6,10–12]. Dedifferentiated liposarcoma of the extremities is rare, and the true prevalence is unknown [6].
In our case, the 60 year female patient presented with a dedifferentiated liposarcoma with a high grade fibrosarcomatous dedifferentiation in the thigh, with a local recurrence and morbidity due to its huge size.
CONCLUSION
We are reporting a a huge dedifferentiated liposarcoma of the thigh with a high grade fibrosarcomatous differentiation and a local recurrence in a 60 year old female patient. This is a rare finding in the literature, as there are only ten previous reports of either radiological or pathological cases of dedifferentiated liposarcomas. To the best of our knowledge, ours is the 11th case of dedifferentiated liposarcoma with a fibrosarcomatous dedifferentiation, with both pathological and radiological findings.
[1]. Goldblum JR, Weiss SW, Liposarcoma.In: Goldblum JR and Weiss SD (edi)Enzinger and Weiss’s Soft tissue tumors 2001 4thMosby Pub.:662-71. [Google Scholar]
[2]. Evans HL, Liposarcoma: A study of 55 cases with reassessment of its classificationAm J Surg Pathol 1979 3:507-23. [Google Scholar]
[3]. Angelo Paulo Dei TOS, Adipocytic tumors. In: Goldblum JR, Flope AC, Inwards CY (edi)Bone and soft tissue pathology 2010 Saunders Elsevier Pub.:111-13. [Google Scholar]
[4]. Dalal KM, Kattan MW, Antonesau CR, Brennan MF, Singer S, Subtype Specific prognostic monogram for patients with primary liposarcoma of the retroperitoneum, extremity or trunkAnn Surg 2006 244(3):381-91. [Google Scholar]
[5]. Sunwoo MO, Park HY, Oh HK, Choi HY, Dedifferentiated Liposarcoma of the thigh: Case reportJ Korean Radiol Soc 2002 47(5):527-31. [Google Scholar]
[6]. Kransdorf MJ, Meis JM, Jelinek JS, Dedifferentiated Liposarcoma of the extremities. Imaging findings in four patientsAm J Roentgenol 1993 161:127-30. [Google Scholar]
[7]. Henricks WH, Chn YC, Goldblum JR, Weiss SW, Dedifferentiated Liposarcoma : a clinicopathological analysis of 155 cases with a proposal for expanded definition of dedifferentiationAm J Surg Pathol 1997 21(3):271-81. [Google Scholar]
[8]. Meiss JM, Dedifferentiation in bone and soft-tissue tumors : a histologic indicator of tumor progression : implications for managementSurg Pathol 1990 3:169-78. [Google Scholar]
[9]. Evans HL, Khurana KK, Kemp BL, Ayala AG, Heterologous elements in the dedifferentiated component of dedifferentiated liposarcomaAm J Surg Pathol 1994 18:1150-57. [Google Scholar]
[10]. Hoshi M, Matsumoto S, Manabe J, Tanizana T, Shigemitsu T, Koyanagi H, Surgery for dedifferentiated liposarcoma, presenting two radiologically and pathologically distinctive patternsJpn J Clin Oncol 2006 36(7):462-67. [Google Scholar]
[11]. Yu L, Fung S, Hojnowski L, Damron T, Dedifferentiated liposarcoma of soft tissue with high grade osteosarcomatous dedifferentiationRadiographics 2005 25(4):1082-86. [Google Scholar]
[12]. Yoon RS, Benevenia J, Beebe KS, Hameed M, Dedifferentiated Liposarcoma of thigh with chomdrosarcomatous dedifferentiated componentAm J Orthop 2010 39(11):114-18. [Google Scholar]