The Spontaneous Prelabour Rupture of Anunscarred Uterus at 34 Weeks of Pregnancy
Malabika Misra1, Ronita Roychowdhury2, Nayan Chandra Sarkar3, Murary Mohan Koley4
1 Assistant Professor, Department of Obstetrics and Gynaecology,
2 Clinical Tutor, Department of Obstetrics and Gynaecology,
3 Assistant Professor, Department of Obstetrics and Gynaecology,
4 Associate Professor, Department of Obstetrics and Gynaecology, College of Medicine & JNM Hospital, WBUHS
NAME, ADRES, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Malabika Misra, Assistant Professor, Department of Obstetrics and Gynaecology, 8,Moore avenue, Kolkata-700040, India.
Phone: 9830952305 E-Mail: misra_malabika@rediffmail.com
Uterine rupture is an obstetric emergency needs immediate surgery and is associated with poor fetal & maternal outcome. Usually uterine rupture occurs at the lower segment (weakest part) if there is no history of uterine surgery. We hereby are reporting a case of spontaneous uterine rupture at fundus, at 34 weeks of gestation in a patient who has never had uterine surgery. Only uterine curettage was done once for missed abortion.
In this case, diagnosis was delayed until the patient went into massive hemorrhagic shock; because, there was no history of previous uterine surgery. However, clinical picture of the ruptured uterus at the fundus suggests there was some weakness at the fundus. Thereafter, D & C operation was taken into account. Subtotal hysterectomy was done as the rupture was irreparable damage to the fundus. Her one month follow up was uneventful.
Unscarred ruptured uterus, Preterm uterine rupture, Fundal rupture
CASE REPORT
Mrs. S.D. a 35 years old lady who was in the 34th week of her pregnancy, with an obstetric history of a twin delivery 13 years back and one D/C operation 12 years back, was admitted with acute pain in the abdomen, in the emergency labour ward of our hospital. At first, she had felt an acute onset of severe pain in the abdomen in the evening, and was admitted at a rural hospital immediately. There, she was treated conservatively. As the pain was not relieved and as her USG-scan revealed an I.U.F.D, she was referred to our hospital on the very next day. On admission, she was in the process of hemorrhagic shock (her pulse rate was 110/min, BP was 100/70 and pallor was mild to moderate). There was moderate tenderness over the uterus and P/V examination revealed cervix was un-favorable. We missed the diagnosis.
Thereafter, the patient was treated for the induction of labour by the intra-cervical PGE2 gel and oxytocin infusion in escalating doses for more than 24 hours. Her cervix remained unfavourable but the patient developed severe pallor and a hypovolaemic shock. The pains of uterine contraction subsided but a diffuse tenderness developed in the whole abdomen.
Her pulse rate was raised to 120/min, her BP was fell to 80/50, her urine output was reduced to 50ml/hr and her abdomen became distended and tender. This raised a clinical suspicion of a ruptured uterus. So, a laparotomy was done and the haemoperitoneum was detected. The baby was delivered by LSCS.
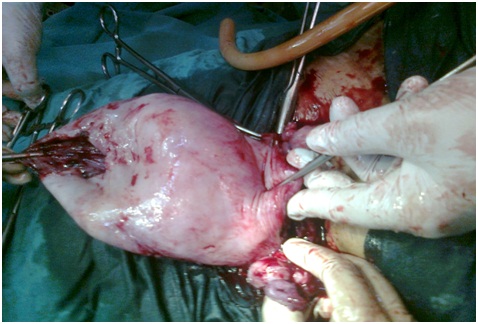
The fresh, stillborn, male baby was born weighing 2.1kg. [Table/Fig-1] and the uterus was found to have a large rent at the fundus, with a thin irregular margin [Table/Fig-2] and the placenta was partially detached over the rent. A large blood clot (500 ml) was attached at the fundus at the site of the tear. 1500ml of free blood with amniotic fluid was collected in a sucker bottle. On seeing the thin and flaccid condition of the fundus of the uterus, a subtotal hysterectomy was done. She was discharged on the 8th postoperative day. Her follow up period was uneventful.

DISCUSSION
When the rupture of a gravid uterus occurs at the fundus of an apparently unscarred uterus, prior to the onset of labour, the diagnosis is often delayed. Because, patient is considered as low risk case and hemorrhage is not revealed as blood collects into the intra-peritoneal space through the rent. The absence of a haemorrhage and no history of a uterine surgery give a false sense of security. The predisposing factors of uterine ruptures are multiparty, multiple pregnancies, big babies, the injudicious use of oxytocics, a contracted pelvis, malpresentation, an internal podalic version and instrumental deliveries. In our case, there was no such factor. There was a H/O a twin delivery and a D/C operation which was done for a missed abortion within one year of a delivery. So, we think that our patient may have had a uterine scar from an unnoticed perforation during the curettage. That scar of the uterus was probably stretched with the foetus and at a certain point of distention, it may not have been able to withstand the stretching and so had given way. The large blood clot at the site of the perforation signified that initially the rent may have been small, which may have led to the placental site haemorrhage and the foetal death. The mother developed shock on the 4th day of the onset of the pain. This indicated that the oxytocin which was used for the induction of labour, may have intensified the uterine contraction, which may have led to the bursting of the uterus at the weakest point. Similar cases were reported by Yazawa H et al., and Kelly Albrecht in their cases there was no history of uterine surgery and like our case rupture occurred during pregnancy or before the onset of labour [1,2]. E. Nkwabong et al., and) reported case where rupture occurred in pregnancy after correction of Asherman’s syndrome [3]. Y azawa H et al., reported a case of rupture uterus at 33 weeks of IVF pregnancy following laparoscopic enucleation of uterine tomour [4].
CONCLUSION
A pregnancy in a scarred uterus (after a caesarean section or a myomectomy) gets better surveillance than that after a normal delivery gets. Our case report suggests that a past history of a curettage should be considered as a risk factor for a uterine rupture during a pregnancy in an apparently unscarred uterus. Therefore, a past history of a D/C operation, especially after multiple pregnancies, an acute onset of severe pain in the abdomen with a sudden loss of perception of the foetal movements by the mother and a diffuse tenderness in the abdomen, all these together should raise the suspicion of a concealed uterine rupture.
[1]. Nkwabong E., Kouam L., Takang W., spontaneous uterine rupture during pregnancy: case report and review of literatureAfrican Journal of Reproductive Health August. 2007 11(2) [Google Scholar]
[2]. Albrecht Kelly, Lam Gail, reterm spontaneous uterine rupture in a Non-labouring Grand Multipara: A case reportJ Obstet Gynaecol Can 2008 30(7):586-89. [Google Scholar]
[3]. Deaton JL, Maier D, Andreoli J Jr, spontaneous uterine rupture during pregnancy after treatment of Asherman’s syndromeAm J Obstet Gynecol 1989 May 160(5 Pt 1):1053-54. [Google Scholar]
[4]. Yazawa H, Endo S, Hayashi S, Suzuki S, Ito A, Fujimori K, spontaneous uterine rupture in the 33rd week of IVF pregnancy after laparoscopically assisted enucleation of uterine adenomatoid tumourJ Obstet Gynaecol Res 2011 Jan 5 doi: 10.1111/j.1447-0756.2010.01361.x. [Epub ahead of print]. [Google Scholar]