An Anatomical Study on the Foramen Ovale and the Foramen Spinosum
Karan Bhagwawan Khairnar1, Prashant Amanrao Bhusari2
1 Assistant Professor, Department of Anatomy, MVPS Dr. Vasantrao Pawar Medical College, Adgaon, Nasik 03, Maharashtra, India.
2 Associate Professor & Head, Department of Anatomy, MVPS Dr. Vasantrao Pawar Medical College, Adgaon, Nasik 03, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Karan Bhagwan Khairnar, Assistant Professor, Department of Anatomy, MVPS Dr. Vasantrao Pawar Medical College, Adgaon, Nasik 03 Maharashtra, India.
Phone: 07507177677
E-mail: khairnarkaran@gmail.com
Introduction: An anatomical study was undertaken to note the shape of the foramen ovale(FO), foramen spinosum (FS) & presence or absence of canalis innominatus. FO is present in the posterior part of the greater wing of sphenoid. FS is located posterolareral to foramen ovale.
Aims & Objective: We attempted this study to find out the variations in shape, bony growth & divisions of FO & FS in available dry human skulls.
Material & Methods: We studied 100 human skulls available in the Department of Anatomy MVPS Medical College, Nashik. This study of FO & FS was done in both male & female skulls.
Observation & Results: We found oval, round, almond, triangular
shaped FO. Variations in the shape of FO showed the maximum as oval shaped followed by almond, round & slit like.
Conclusion: FO is of great surgical & diagnostic importance in procedures like percutaneous trigeminal rizotomy in trigeminal neuralgia, transfacial fine needle aspiration technique etc. Considering such clinical importance of FO & FS, this study was worthwhile as far as neurosurgeons are concerned.
Foramen ovale, Foramen spinosum, Canalis innominatus, Trigeminal neuralgia, Percutaneous trigeminal rizotomy
INTRODUCTION
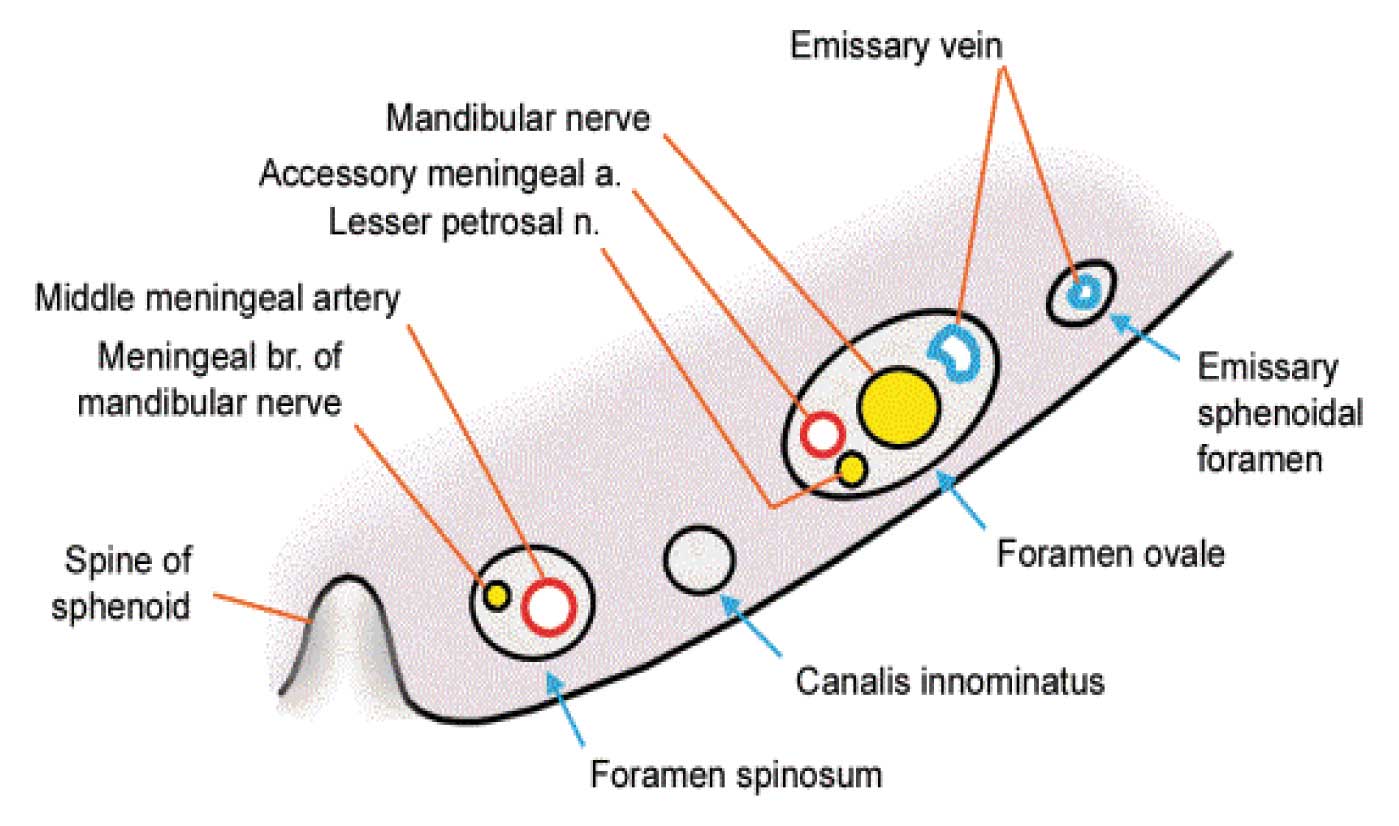
The FO is present in the posterior part of the greater wing of the sphenoid. The important structures which pass through it are the mandibular nerve, the accessory meningeal artery, the lesser superficial petrosal nerve and the emmissary vein [1]. This is the one of the important foramina which are situated at the transition zone between the intracranial and the extracranial structures [2]. The FO opens into the infratemporal fossa, through its other opening on the lateral surface of the greater wing [3]. The FS is located posterolareral to the foramen ovale, which also leads to the infratemporal fossa [4] and it transmits the Middle Meningeal Artery (MMA) and the nervus spinosus. However, the FS is much smaller than the FO and it is circular. Sometimes, there is a separate foramen for the lesser petrosal nerve, which is known as the Canaliculus Innominatus of Arnold. The structures which pass through the FO and through the smaller foramina near it have been shown in [Table/Fig-1]. The lesser petrosal nerve sometimes passes through the canalis innominatus [5]. Although variations in the shape of the FO may normally be present, a careful evaluation of these foramina will facilitate the diagnosis of the lesions which are present in the middle cranial fossa and the nasopharynx. When an enlargement of the FO occurs, it is tempting to consider neurinoma of the fifth nerve [6]. This study not only has developmental anatomical importance, but it also has a profound surgical importance, as in trigeminal neuralgia and a diagnostic importance as in tumours and in various types of epilepsy, as of the fine needle aspiration technique in a perineural spread of the tumour and as of the electroencephalographic analysis in seizures. Only scattered reports are available on the variations of the FO and the FS. Hence, the authors feel that they have been studied.
Showing structure passing through FO and FS [5]
AIMS AND OBJECTIVES
To find the variations in the shape, bony growth and the divisions of the FO and the FS.
To measure the distance between these two foramina.
To compare these data with those which is available in the literature.
MATATERIALS AND METHODS
A total of 100 dried adult human skulls (males-70, females-30) were selected for the present study. These skulls were obtained from the Department of Anatomy, MVPS Medical College, Nasik, India. The shape of the FO and the bony growth and any division of the FO were noted. The distance between the FO and the FS was also recorded with the help of a vernier caliper, a divider and a scale.
OBSERVATIONS
We found the maximum number of FOs as oval shaped;followed by almond shaped ,round and slit like FOs [Table/Fig-2]. We also measured the distance between FO & FS [Table/Fig-3].
Showing % of different shapes of FO
| M F | M F | Total % of Diff. Shapes (200 Sides) |
|---|
| OVAL- RT | 55 | 23 | 78.5 | 76.6 | 76.5% |
| LT | 54 | 21 | 77.1 | 70.0 | |
| ALMOND-RT | 6 | 3 | 8.5 | 10 .0 | 10.5% |
| LT | 9 | 3 | 12.9 | 10 | |
| ROUND-RT | 5 | 1 | 7.1 | 3.3 | 7% |
| LT | 5 | 3 | 7.1 | 10 | |
| SLIT-RT | 4 | 3 | 5.7 | 10 | 6% |
| LT | 2 | 3 | 2.9 | 10 | |
Showing Distance between FO & FS
| Parameters (mm) | Male | Female |
|---|
| Rt | Lt | Rt | Lt |
|---|
| Distance between FO & FS- | Mean | 4. | 3.8 | 3.6 | 3.2 |
| Max | 7.0 | 7.0 | 7.0 | 5.0 |
| Min | 1.0 | 2.0 | 2.0 | 2.0 |
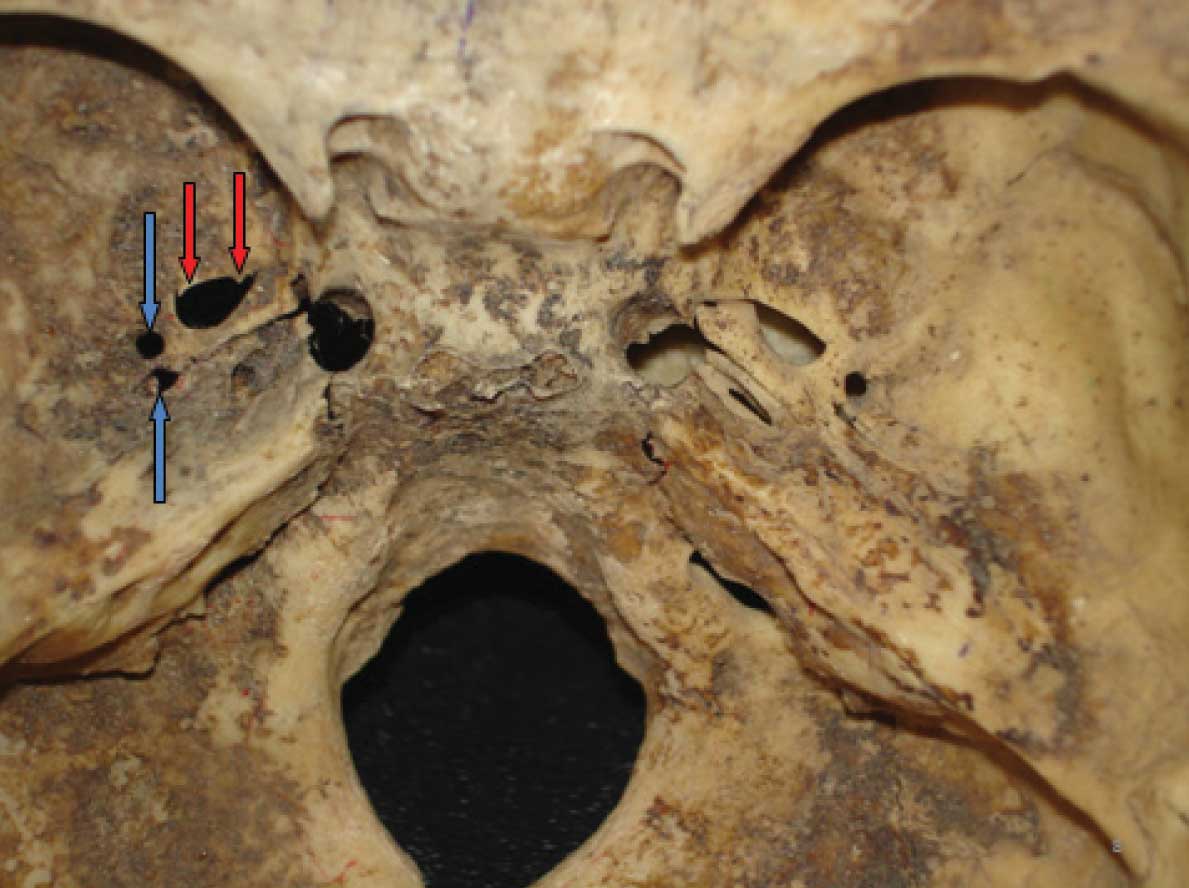
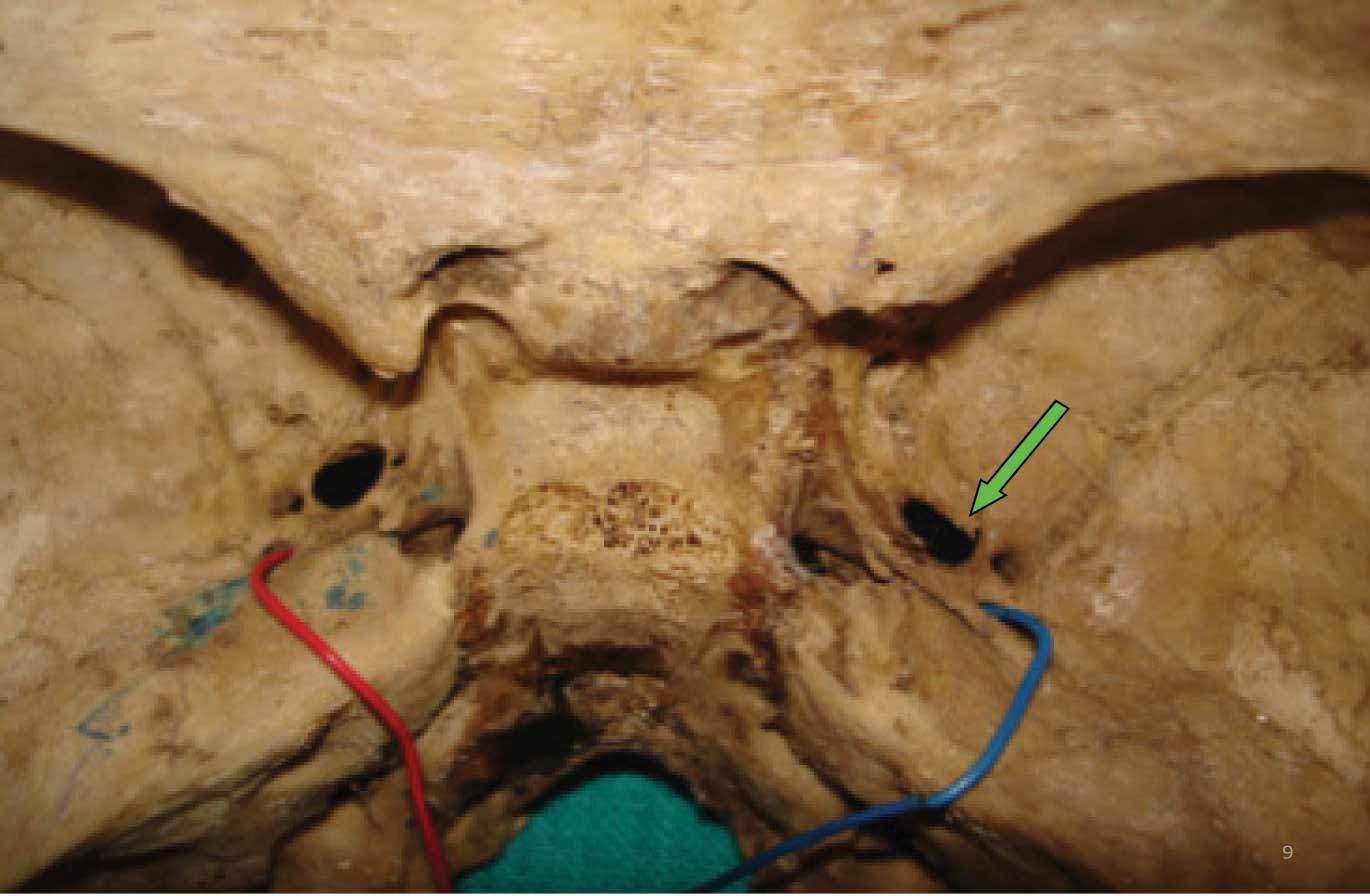
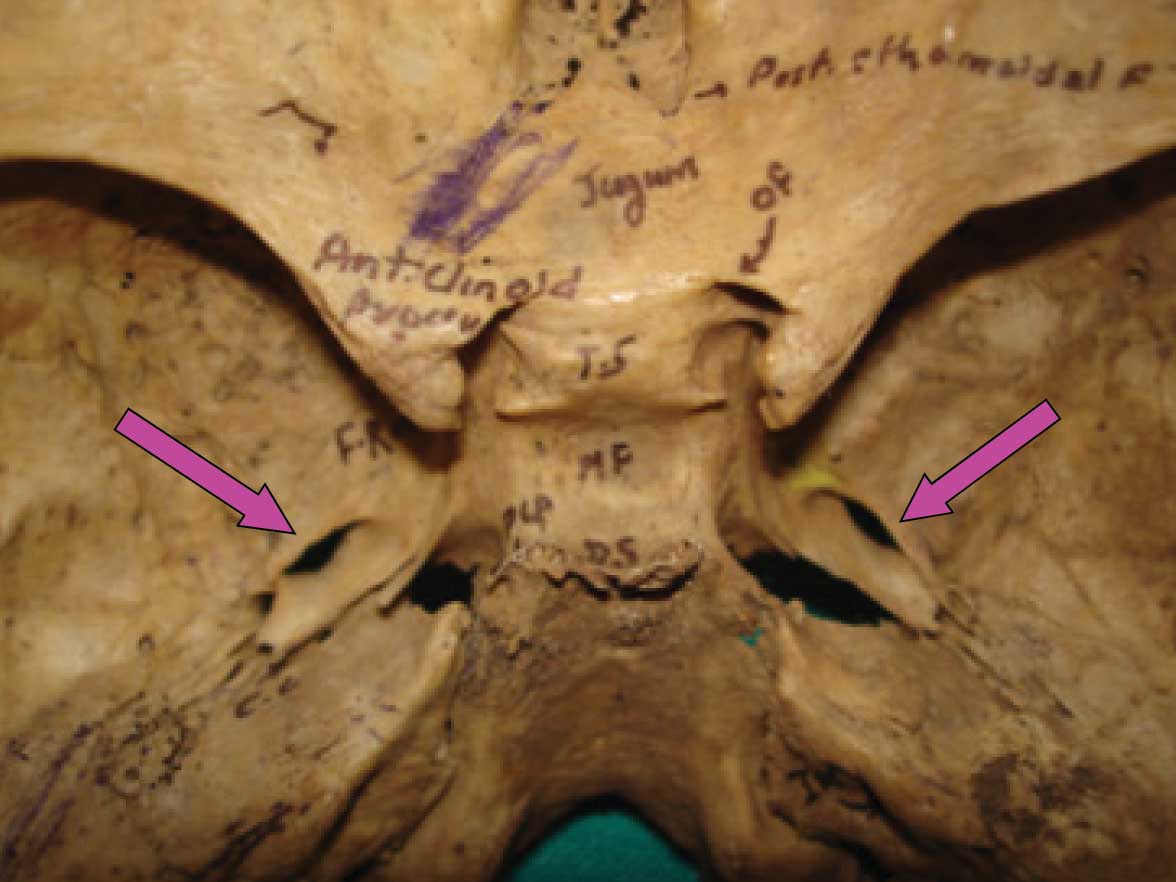
Fourteen cases (Rt-5, Lt-9) out of 200 sides (one case means one side of a skull) had shown a bony growth on the margin of the FO. Out of these, 8 cases had tubercles protruding from the margin, as shown in [Table/Fig-4]. Two cases had bony spurs, as shown in [Table/Fig-5]. Four cases showed bony plates protruding from the margin of the FO, as shown in [Table/Fig-6]. We found a doubled FO in three cases (M-2, F-1) out of 100 skulls, as in [Table/Fig-7].
Showing tubercles protruding from margin of left FO & doubled left sided FS.
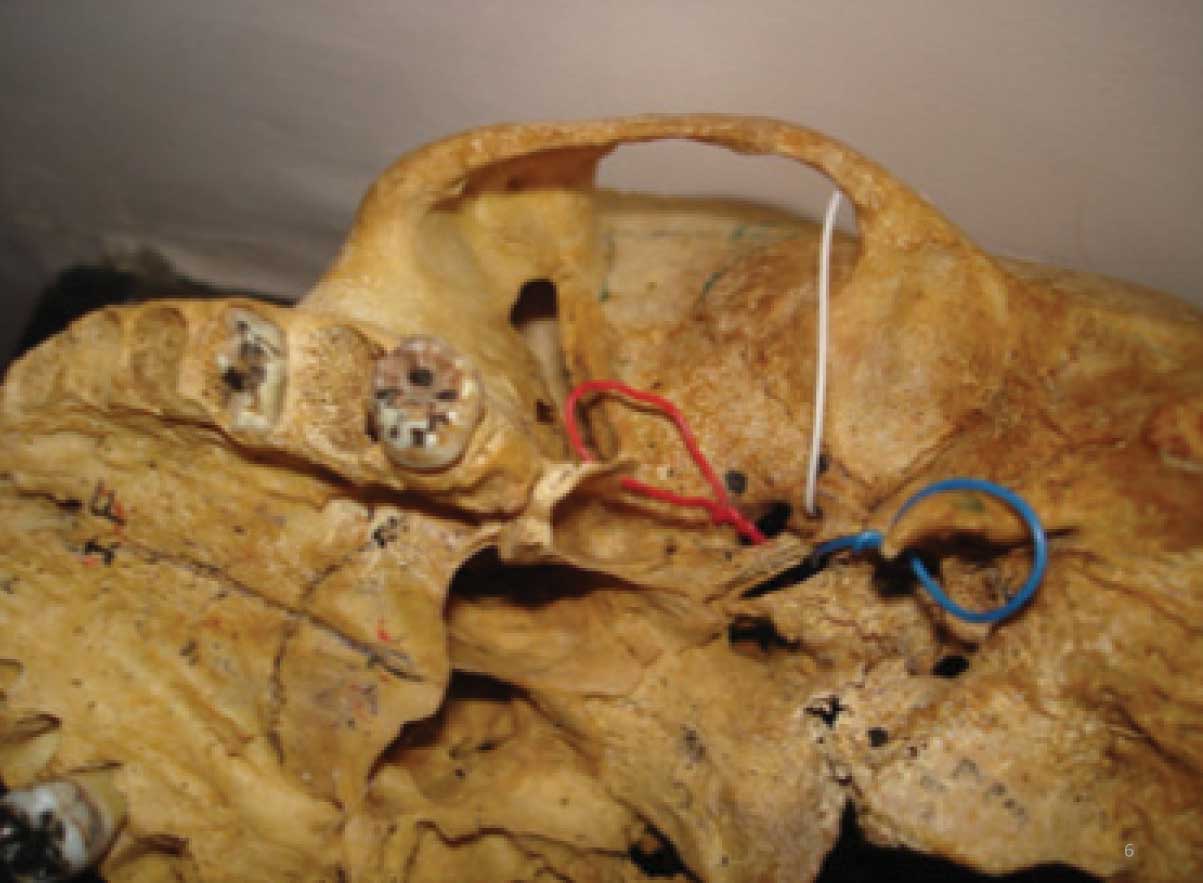
Showing bony spur protruding from margin of right FO & doubled FS on both sides.
Showing bony plate protruding from margin of left FO & doubled right FS.

DISCUSSION
The appearance of the various bony outgrowths of the foramen ovale like spines, spurs, tubercles, bony plates, etc indicate bony overgrowths during its developmental process, between its first appearance and the perfect ring formation. In one study which was conducted in India, forty patients of trigeminal neuralgia were treated with percutaneous trigeminal ganglion balloon compression. In all the patients except one, the needle could be introduced easily. The only exception was a patient with a variation in shape of the FO, in whom; the needle just fitted in the foramen [7]. The variations in the shape of FO showed the maximum number of FOs as oval shaped; followed by almond, round & slit like FOs [Table/Fig-8].
Showing slit like FO on both sides.
Our findings were on the higher side as compared to those of other workers [8, 9, 10]. In 9% males and in 10% females, a slit like foramina was present [Table/Fig-8]. We found a double FS in 6 cases and in 2 cases, it was very tiny and it was absent on 1 side (Rt).Singh et al., [11] also found a duplicated FS in 2 cases and it was absent in 1 case. The venous segment of the FO may be separated from its other contents. This results in a doubled FO (Lang J.) [12]. Sometimes the FO and the FS may be continuous. Rarely, may the FS be absent; in such a case, the MMA enters the cranial cavity through the FO. Tubbs et al., [13], in their study on the ossification of the ligaments near the foramen ovale, revealed that the ossified pterygospinous (ligament of Civinini) and pterygoalar (ligament of Hyrtl) ligaments divide the foramen ovale into two compartments. They concluded that such bony obstructions could interfere with the transcutaneous needle placement into the foramen ovale. Khan A. A. [14] observed three cases of variant foramen spinosum among 25 skulls which were studied. The electrode technique through the FO is one of the best neurological examinations for hippocampectomy [15]. In case of the FO, the puncture advancement of a catheter, more than 10mm from the FO, is likely to damage the internal carotid artery [16]. In the treatment of Trigeminal neuralgia, an alcohol injection is made into the Gusserian ganglion which is situated just below the foramen ovale [17]. Variations in the shapes of the FO are found due to developmental reasons, which may seriously hamper clinical and diagnostic procedures. This shows the need of a study.
CONCLUSIONS
This study intended to offer specific anatomical data with morphological patterns to increase the understanding of the FO and the FS features. Some FOs show tubercles, bony plates, etc. The slit like shape signifies an over-ossification during the developmental process. The FO allows the passage of the mandibular branch of the trigeminal nerve, which is the target of the trigeminal radiofrequency rhizotomy. The data of the present study may be helpful for knowing the different variations of these foramina and so they should be taken into account when neurosurgical procedures are planned in the middle cranial fossa. The FS is an easily identifiable landmark in microsurgery in the middle cranial fossa and the knowledge on such variations is important for neurosurgeons, radiologists and anatomists because of the refined techniques which are available these days. In conclusion, this study was of clinical and anatomical significance to the medical practitioners in cases of trigeminal neuralgia and in diagnosing any aneurysm or vascular lesions of the cranial cavity. This knowledge will be useful to neurosurgeons for the identification and preservation of the neurovascular structures, when they plan approaches to the middle cranial fossa. We believe that our data on the FO will be enlightening, not only for anatomists, but also for clinicians.
[1]. Gray Henry, Osteology. In:Peter L Williams, Warwick, RogerGray’s Anatomy of Human Body 1989 37thNew York and LondonChurchill Livingstone:267-447. [Google Scholar]
[2]. Ray B, Gupta N, Ghose S, Anatomic variations of foramen ovaleKathmandu University Med J 2005 (3):64-68. [Google Scholar]
[3]. Soames RW, Gray’s Anatomy of the Human Body 1995 38thChurchill Livingstone:425-736. [Google Scholar]
[4]. Chaurasia B.D., Osteology. In: Krishna GargB.D Chaurasia’s Human Anatomy 2004 34thNew DelhiCBS publishers:3-43. [Google Scholar]
[5]. Singh Inderbir, Textbook of Inderbir Singh with colour atlas 4th edition, Jaypee brothers publishers, Chapt.Osteology 2007 (1):124 [Google Scholar]
[6]. Palacios E, MacGee E, Radiological diagnosis of trigeminal neurinomasJournal of Neurosurgeries 1972 :153-56. [Google Scholar]
[7]. Natarajan M, Percutaneous trigeminal balloon compression: experience in 40 patientsNeurology India 2000 99:785-86. [Google Scholar]
[8]. Ray Biswabina, Gupta Nirupama, Ghose Supriya, Anatomical variations of foramen ovaleKathamandu University Medical Journal 2005 3 (1)(9):64-68. [Google Scholar]
[9]. Yanagi S, Development studies on foramen rotundum,foramen ovale & foramen Spinosum of human sphenoid boneThe Hokkoido Journal of Medical Sciences 1987 62(3):485-96.PMID 3610040 [Google Scholar]
[10]. Lang J, Maier R, Schafhauser O, Postnatal enlargement of foramina rotundum ,ovale et spinosum and their topographical changesAnatomischer Anzeiger 1984 156(5):351-87.PMID 6486466 [Google Scholar]
[11]. Singh Brinjendra, Singh Balbir, Study of middle cranial foramina GMC, ChandigarhJ. Anat. Soc. India 2001 50(1):69-98. [Google Scholar]
[12]. Lang J, Clinical Anatomy of the Head, Neurocranium, Orbit and Craniocervical Region Springer-Verlag, Berlin.1883 [Google Scholar]
[13]. Tubbs RS, May WR Jr, Apaydin N, Shoja Shokouhi G, Loukas M, Cohen-Gadol A, A Ossification of ligaments near the foramen ovale: an anatomic study with potential clinical significance regarding transcutaneous approaches to the skull baseNeurosurgery 2009 65(6 Suppl):60-64. [Google Scholar]
[14]. Khan AA, Asari MA, Hassan A, Anatomic variants of foramen ovale and spinosum in human skullsInt. J. Morphol 2012 30(2):445-49. [Google Scholar]
[15]. Weiser HG, Siegel AM, Analysis of foramen ovale electrode recorded seizures and correlation with outcome following hippocampectomyEpilepsia 1991 32:838-50. [Google Scholar]
[16]. Kale Aysin, Aksu Funda, Ozturk Adnan, Gurses Ilke, Gayretli Ozean, Zaybek Fatma, Review of complications due to foramen ovale punctureSaudi Medical Journal 2009 Jan 30(1):56-59. [Google Scholar]
[17]. Bailey Love, Nerves In: Macneill loveBailey and Love’s Short Practice of Surgery 1971 15thH.K.Lewis and Co.Ltd:452 [Google Scholar]