Anatomical Variations in the Emergence of the Cutaneous Nerves from the Nerve Point in the Neck and Identification of the Landmarks to Locate the Nerve Point with Its Clinical Implications: A Cadaveric Study on South Indian Human Foetuses
Chandni Gupta1, Antony Sylvan D’souza2, Biswabswabina Raythe3
1 Assistant Professor, Department of Anatomy, Kasturba Medical College, Manipal, India.
2 Professor and Head, Department of Anatomy, Kasturba Medical College, Manipal, India.
3 Associate Professor, Department of Anatomy, Kasturba Medical College, Manipal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Chandni Gupta, Department of Anatomy Kasturba Medical College, Manipal, India.
Phone: 9886738555
E-mail: chandnipalimar@gmail.com
Objective: The cutaneous nerves from the cervical plexuses are anaesthetized by using local anaesthetics for pain relief or when minor surgical operations are performed. Knowing the variations in these nerves is important for anaestheticists to administer an effective anaesthesia to a particular nerve. So, the aim of this study was to look for the variations in the emerging patterns of the cervical cutaneous nerves in the neck and to locate the nerve point in the neck by using the superficial landmarks.
Materials and Methods: The neck was dissected in 16 foetal cadavers (total 32). The foetuses were divided into 2 groups, depending upon their ages- group 1 (13-24wks) and group 2 (24-38wks). The cervical cutaneous nerves were dissected. Measurements for locating the nerve point, were taken in both the groups.
Results: The statistical analysis of the measurements was done. In group 1, the mean distances of the nerve point from the External Acoustic Meatus (EAM), on the right and left sides, were 2.06cm and1.85cm and in group 2, the distances on the right and left sides were 2.32cm and 2.08cm. The mean distance of the nerve point from the clavicle in group 1, on both the right and the left sides was 1.85cm, and in group 2, the mean distances on the right and left sides were 2.67cm and 2.62cm. The variations in the cutaneous nerves which emerged from the nerve point were recorded and photographed.
Conclusion: These landmarks will help the anaestheticists in locating the nerve point. These variations in the branches of the cervical plexus should be known to the anaestheticists while they give anaesthesia to a particular nerve during a nerve block.
Nerve point, Lesser occipital nerve, Great occipital nerve, Transverse cervical nerve, Supraclavicular nerve
INTRODUCTION
The cervical cutaneous nerves from the cervical plexus arise through the superficial cervical fascia as four different nerves, the lesser occipital nerve (C2), the greater auricular nerve (C2, C3), the transverse cutaneous nerve of the neck (C2, C3) and three supraclavicular nerves (medial, intermediate and lateral) (C3,C4) on the posterior border of the Sterno Cleido Mastoid (SCM) muscle. These cervical cutaneous nerves carry the sensation from the antero-lateral cervical skin. During dissection of the neck, it is usually found that these cutaneous branches emerge on the posterior border of the SCM, at a point which is described as a nerve point. The identification of the nerve point is important clinically [1].
Generally, these cutaneous nerves are anaesthetized by using local anaesthetics for pain relief or when minor surgical procedures are performed. This anaesthetic procedure is also beneficial for the control of the pain in the temporomandibular joint area. Overall, to accomplish an effective anaesthetization of these cutaneous nerves, the anaesthetic is injected into the middle portion of the posterior border of the SCM [1].
The variable sites and the distributions of the cervical cutaneous nerves lead to surgical complications during the performance of Raythe anaesthetic technique. For this purpose, a careful anaesthesia of a certain branch of the cervical cutaneous nerves cannot be achieved efficiently. There are insufficient published studies that have described the emerging patterns and the branch distributions of the cervical cutaneous nerves. The variations in the cervical cutaneous nerve and the identification of the nerve point by using the superficial landmarks are clinically important. Therefore, knowledge on the anatomical variations of the distribution and the location of the point of emergence is essential before this information can be exploited clinically [1].
The aim of this study was to locate the nerve point by using superficial landmarks and to look for the variations in the emergence of the cervical cutaneous nerves in the neck, and to thereby, provide critical data for the clinical aspects.
MATATERIALS AND METHODS
In this study, the necks from 16 formalin fixed human foetuses were dissected in the Department of Anatomy, KMC, Manipal, Karnataka, India. The foetuses were divided into 2 groups according to their ages- group 1 (13-24 weeks) and group 2 (24-38 weeks). Among the 16 foetuses, there were 9 foetuses in group 1 (7 females and 2 males) and 7 in group 2 (3 females and 4 males). Dissection of the cervical cutaneous nerves was done according to the guidelines of Cunningham’s Manual of Practical Anatomy [2]. The variations in the cutaneous nerves which emerged from the nerve point were recorded and photographed. The measurements were made in both the groups between the nerve point and the surrounding landmarks by using a digital caliper on both sides of the neck. The measurements which were done were [Table/Fig-1]:
The distance between the nerve point and the mid-point of the clavicle.
The distance between the nerve point and the External Acoustic Meatus (EAM).
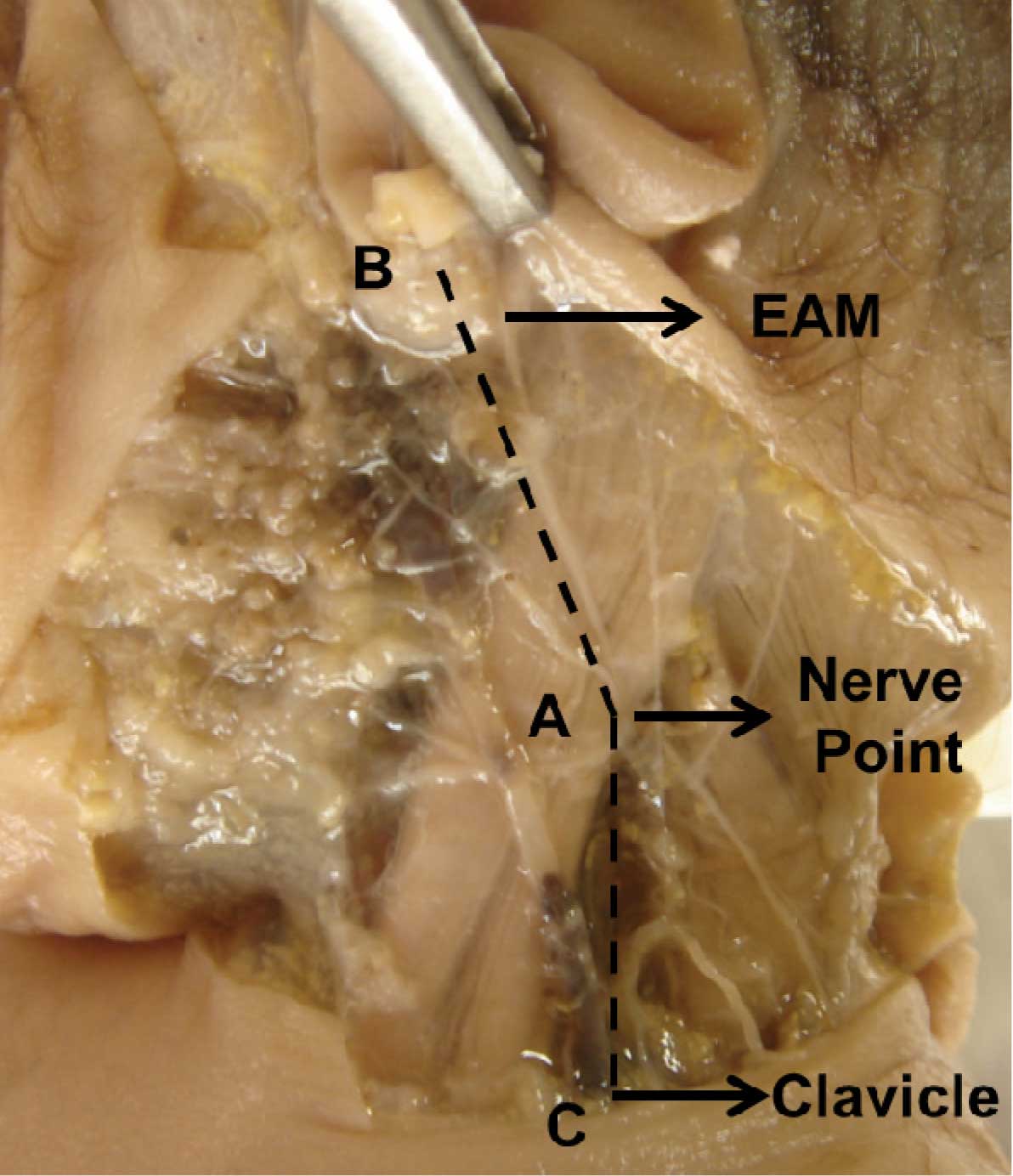
Photograph showing the measurements done for nerve point. AB- The distance between the nerve point and EAM. AC- The distance between the nerve point and the clavicle.
A digital photographic documentation was done. A statistical analysis was done for all the measurements and it was tabulated.
RESULT
Among the 16 foetuses, there were 9 foetuses in group 1 (7 females and 2 males) and 7 in group 2 (3 females and 4 males).
The mean of the parameters which we have measured in both groups of foetuses to locate the nerve point, is given in [Table/Fig-2].
Mean of parameters for group 1 and 2 fetuses.
| Parameters in foetuses of 13-24 weeks (group 1) |
|---|
| Parameters | Mean | Range |
|---|
| Right | Left | Right | Left |
|---|
| The distance between the nerve point and the clavicle | 1.85cm | 1.85cm | 1.4-2.7cm | 1.1-2.9cm |
| The distance between the nerve point and EAM | 2.06cm | 1.85cm | 1.6-2.7cm | 1.5-2.5cm |
| Parameters in foetuses of 25-38wks (group 2) |
| The distance between the nerve point and the clavicle | 2.67cm | 2.62cm | 1.5-3.3cm | 1.8-3.4cm |
| The distance between the nerve point and EAM | 2.32cm | 2.08cm | 2.1-2.6cm | 1.4-2.8cm |
The mean distance of the nerve point from the clavicle in the group 1 foetuses on both the right and left sides was 1.85cm, while the mean distances of the nerve point from the EAM on the right and left sides were 2.06cm and 1.85cm. The mean distances of the nerve point from the clavicle in the group 2 foetuses on the right and left sides were 2.67cm and 2.62cm, while the mean distances of the nerve point from the EAM on the right and left sides were 2.32cm and 2.08cm.
We found that in group 1, there were 2, 3 and 4 greater auricular nerves in 38.8, 16.6 and 5.5% of the cases. The duplication of a lesser occipital nerve was seen in 22.2% of the cases. The transverse cutaneous nerve was absent in 5.5% of the cases and it was duplicated in 5.5% of the cases.
In group 2, we found triplication and duplication of the greater auricular nerve in 35.7 and 21.4% of the cases. Duplication of the lesser occipital nerve was seen in 42.8% of the cases, which has been reported in text books [3, 4]. Duplication of the transverse cutaneous nerve of the neck was seen in 14.2% of the cases.
No variation was noted in the supraclavicular nerves. In all the foetuses, there were 3 variations in number, the medial, intermediate and the lateral.
The variations in the number of each cutaneous nerve which emerged from the nerve point in the groups 1 and 2 are shown in the [Table/Fig-3, 4, 5, 6, and 7].
Percentage of number of each cutaneous nerve in group 1 foetuses
| Nerve | 1 in Number (%) | 2 in Number (%) | 3 in Number (%) | 4 in Number (%) | Absent (%) |
|---|
| Greater Auricular | 38.8 | 38.8 | 16.6 | 5.5 | nil |
| Lesser Occipital | 77.7 | 22.2 | nil | nil | nil |
| Transverse Cutaneous Nerve of Neck | 88.8 | 5.5 | nil | nil | 5.5 |
Percentage of number of each cutaneous nerve in group 2 foetuses
| Nerve | 1 in Number (%) | 2 in Number (%) | 3 in Number (%) |
|---|
| Greater Auricular | 42.85 | 35.7 | 21.4 |
| Lesser Occipital | 57.1 | 42.8 | nil |
| Transverse Cutaneous Nerve of Neck | 85.7 | 14.2 | nil |
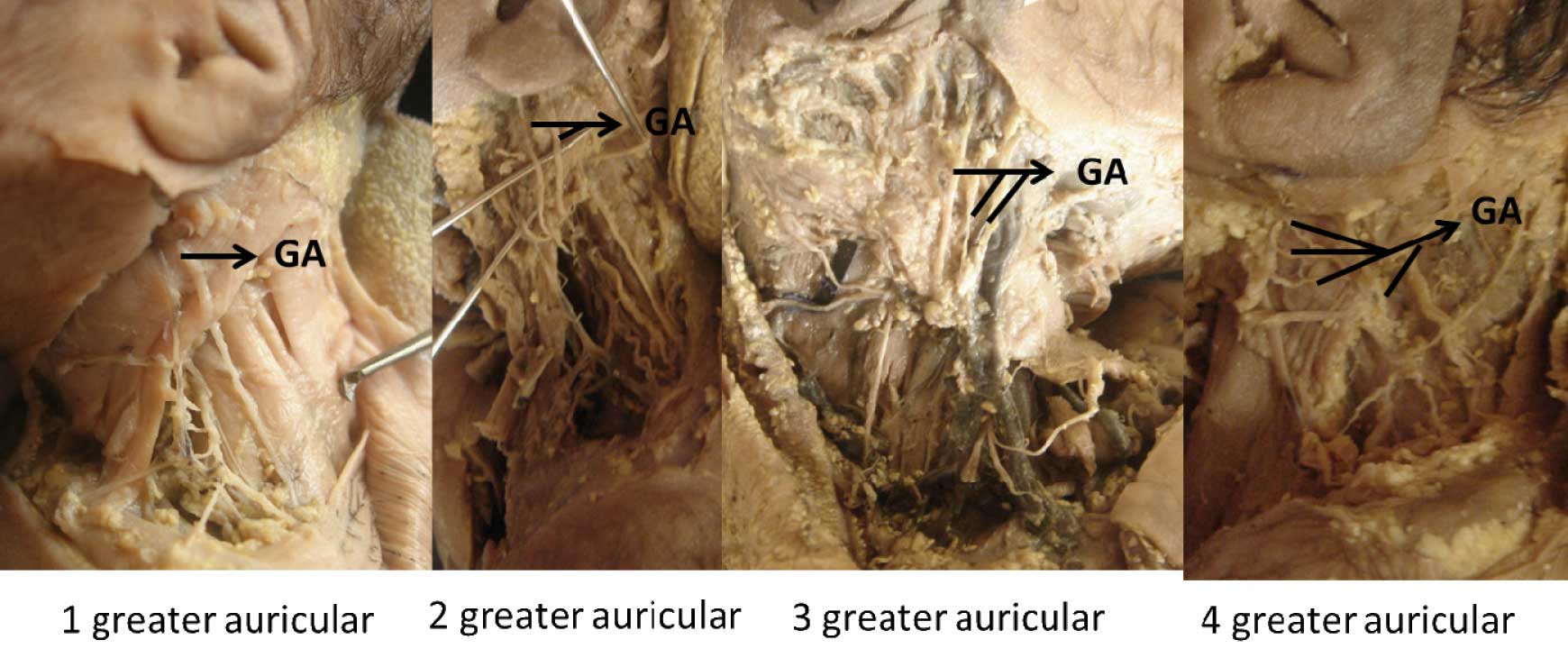
Photograph showing variation in the number of greater auricular nerves emerging from the nerve point. GA- greater auricular nerve.
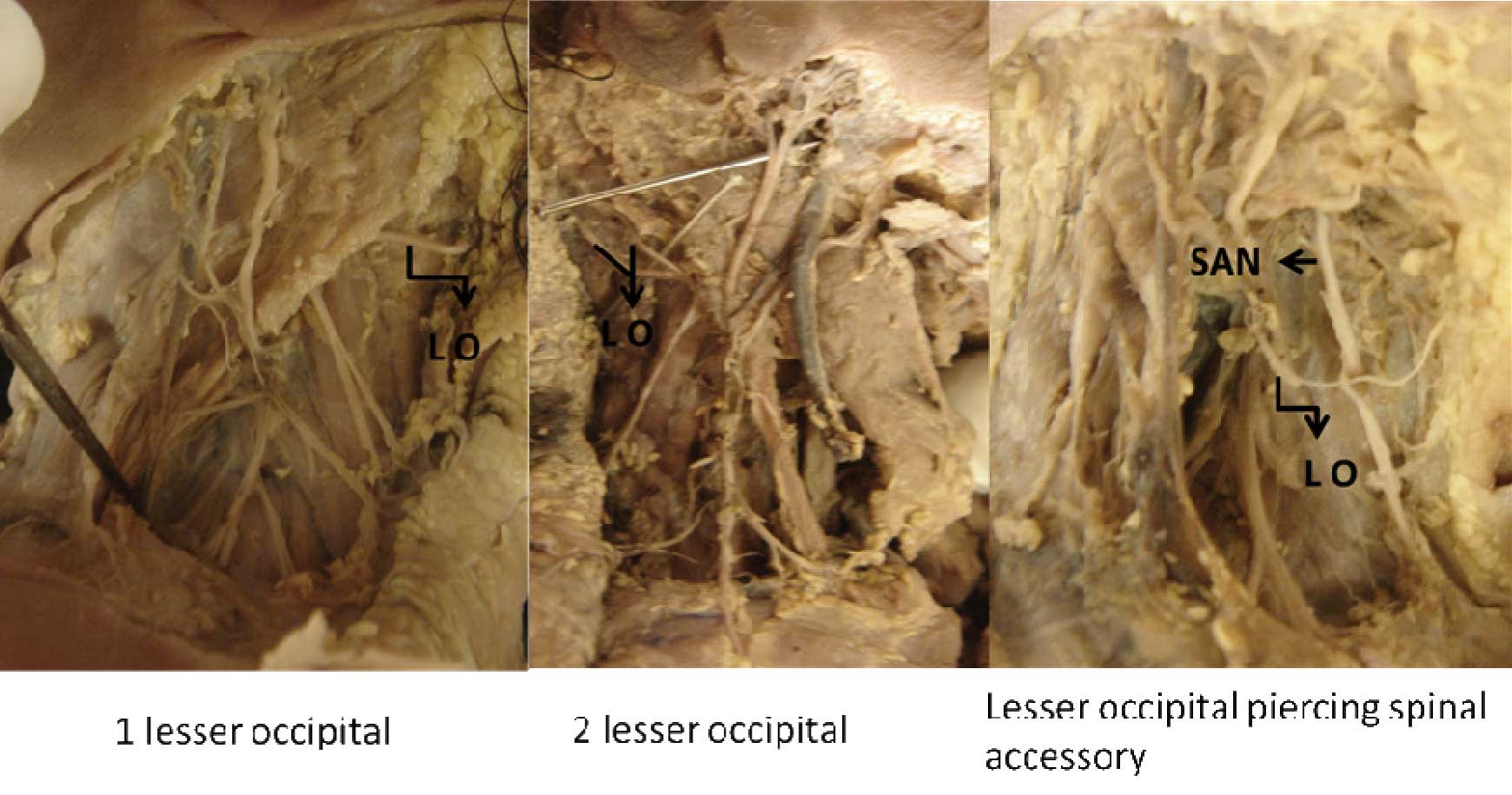
Photograph showing variation in the number of lesser occipital nerves emerging from the nerve point and also lesser occipital nerve piercing spinal accessory nerve in the posterior triangle. LO- lesser occipital nerve, SAN- spinal accessory nerve.
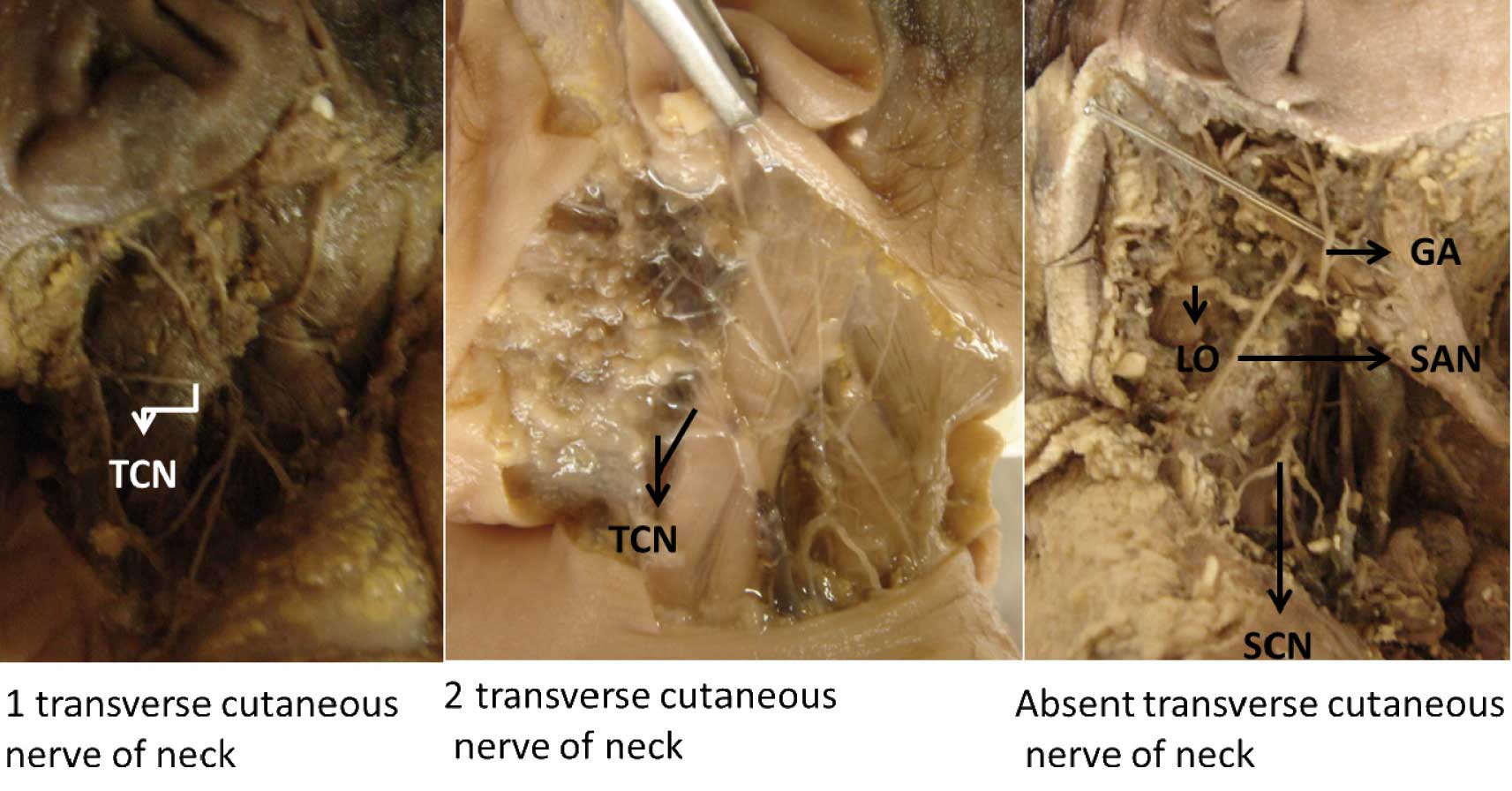
Photograph showing variation in the number of transverse cutaneous nerve of neck emerging from the nerve point. TCN- transverse cutaneous nerve of neck, SAN- spinal accessory nerve. SCN- supraclavicular nerve, LO- lesser occipital nerve, GA- greater auricular nerve.
We also got two important variations in 2 foetuses in one there was lesser occipital nerve piercing the spinal accessory nerve and in the other one there was a loop between spinal accessory nerve and C3 and C4 nerve which supply the trapezius [Table/Fig-6 and 8].
Photograph showing the communication between spinal accessory nerve and C3, C4 nerves supplying the trapezius in the posterior triangle. SAN- spinal accessory nerve. SCN- supraclavicular nerve, LO- lesser occipital nerve, GA- greater auricular nerve.

DISCUSSION
Several reports exist, on the clinical perspectives of the 4 cervical cutaneous nerves. Unfortunately, a thorough description of the variations in the cervical cutaneous nerves has not yet been published.
In one case, we also found that the spinal accessory nerve was pierced by the lesser occipital nerve in the posterior triangle, while looping it. This variation is important, because some studies have quoted that the lesser occipital nerve has been implicated in cervicogenic headaches and in occipital neuralgia [5].
We also found one case in which there was a communication between the spinal accessory nerve and the C3 and the C4 nerves which supplied the trapezius muscle in the posterior triangle. Normally, deep in the trapezius, the spinal accessory nerve forms a plexus with the branches from C3 and C4, but in our study, it communicated with them in the posterior triangle [6].
There is no literature which has mentioned about these variations.
In the literature, no study was found, which was done to localize the nerve point and the variations in the cutaneous branches which emerged from it.
Anaesthetizing these nerve branches is vital for operations in the superficial cervical region. But anaesthetizing these nerves occasionally produces an unpredicted loss of sensation beyond the operative field. The cause of this phenomenon is that the supply of the cervical cutaneous nerves differs and that the emerging points of these nerves are difficult to identify during anaesthetization [1]
Some reports have been published on the levels of the sites of the cervical cutaneous nerves with reference to the surrounding anatomical structures, but they have been studied singly, for each nerve. The height of the emerging point (nerve point) of the cervical cutaneous nerves along the SCM from the EAM and the clavicle were not studied. Because the cervical cutaneous nerves lie along the posterior border of the SCM, an estimation of the height of the emerging points of the cervical cutaneous nerves as compared to the SCM, is believed to be more valuable in clinical applications.
H. J. Kim et al., classified the emerging patterns of the cervical cutaneous nerves in the superficial neck into 7 types, based on the locations of their emergence. They also measured the heights from the clavicular attachment of the SCM to the emergence point of each of the four cervical cutaneous nerve branches, the lesser occipital, the great auricular, the transverse cervical, and the supraclavicular nerves on the posterior border of the SCM. But we took the point of emergence of all the cutaneous nerves as the nerve point and measured its distance from the clavicle, as well as from the EAM [1].
Our study has documented actually, the beneficial superficial bony landmarks for the identification of the nerve point in the neck and the variations which can occur in the number of these cutaneous nerves. It is our anticipation that these data will help the surgeons and the clinicians in avoiding the complications which occur in this region.
[1]. Kim HJ, Koh KS, Oh CS, Hu KS, Kang JW, Chung IH, Emerging patterns of the cervical cutaneous nerves in AsiansInt. J. Oral Maxillofac. Surg 2002 31:53-56. [Google Scholar]
[2]. Romanes GJ, Cunningham’s Manual of Practical Anatomy 2000 14thNew YorkUnited States, Oxford University Press:19-21. [Google Scholar]
[3]. Berry M, Bannister LH, Standring SM, Nervous system. In: Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Ferguson MWJ, editorsGray’s anatomy 1995 38thEdinburghChurchill Livingstone:1264 [Google Scholar]
[4]. Romanes GJ, The peripheral nervous system. InCunningham’s Textbook of Anatomy 1987 12thOxfordOxford University Press:770 [Google Scholar]
[5]. Holla Madhavi, Triplication of the Lesser Occipital NerveClinical Anatomy 2004 17:667-71. [Google Scholar]
[6]. Williams WW, Twyman RS, Donell ST, Birch MR, The posterior triangle and the painful shoulder: spinal accessory nerve injuriesAnn R Coll Surg Engl 1996 78:521-25. [Google Scholar]