Multiple Splenic Artery Aneurysms Secondary to Extra Hepatic Portal Vein Obstruction
Y.C. Manjunatha1, K.N.V. Prasad2, Y.C. Beeregowda3, A. Bhaskaran4
1 Department of Radiodiagnosis, Pondicherry Institute of Medical Sciences, Puducherry-605 014, India.
2 Department of Paediatrics, Sri Devaraj Urs Medical College, Tamaka, Kolar-563101, India.
3 Department of Paediatrics, Sri Devaraj Urs Medical College, Tamaka, Kolar-563101, India.
4 Department of Surgery, Sri Devaraj Urs Medical College, Tamaka, Kolar-563101, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manjunatha YC, Assistant Professor, Department of Radiodiagnosis, Sri Devaraj Urs Medical College, Tamaka, Kolar-563101, India.
Phone: +919478026631
E-mail: manjuyc@gmail.com
Splenic artery, Aneurysm, Extra hepatic
INTRODUCTION
A 14 year old girl presented with vague abdominal pain, recurrent, well tolerated haematemesis and feeling of presence of a lump in the abdomen. Her abdominal examination revealed gross splenomegaly. The laboratory tests, haematological counts, liver enzymes, platelet counts and the international normalized ratio were within the normal limits. Upper gastrointestinal endoscopy showed grade II oesophageal varices. Ultrasonography showed that the portal vein was replaced by multiple, dilated, collateral venous channels around the porta, with collaterals around the pancreas and splenic hilum. There was splenomegaly with a suspicious aneurysm of the splenic artery at the hilum. She was recommended Computed Tomography (CT) angiography, as it was difficult to differentiate aneurysm from collaterals at the splenic hilum on ultrasonography. CT angiography revealed multiple aneurysms in the main splenic artery, at the splenic hilum and at intra parenchymal branches, with largest being seen at the splenic hilum, which measured 18 x 15mm [Table/Fig-1A and B].
CT angiography axial section in 14 year old girl showing tortuous splenic artery with large aneurysm in the distal part of the splenic artery (arrow) and another smaller one in the intra parenchymal branch (arrow head).
Coronal reformatted CT angiography image showing splenic aneurysm.

Portovenous phase CT showed multiple dilated venous collaterals replacing the main portal vein with multiple collaterals around the pancreatic head and the splenic hilum. There was gross splenomegaly [Table/Fig-1C and D].
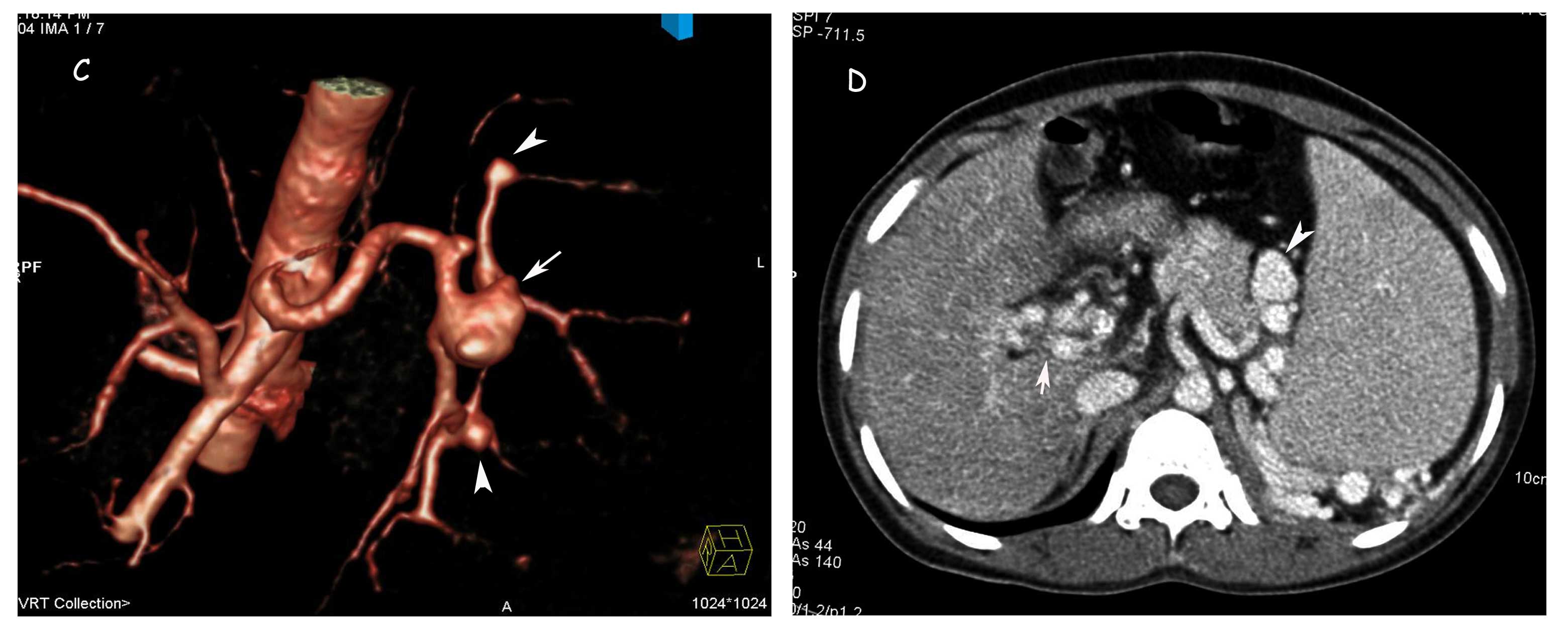
3D volume rendered CT angiography image better depicting the SAA (arrow) and small aneurysms in intraparenchymal branches (arrow heads).
Axial CT section in portovenous phase showing collateral veins replacing the main portal vein at porta (arrow) and multiple dilated collateral venous channels around the spleen indistinguishable from the SAA (arrow head).
The aneurysms were indistinguishable from the dilated collaterals on portovenous phase CT. A diagnosis of extra hepatic portal vein obstruction with splenomegaly and multiple splenic aneurysms was made. Splenectomy, aneurysmectomy and a splenorenal shunt were performed. The post operative period was uneventful.
DISCUSSION
Splenic Artery Aneurysms (SAAs) occur in around 4% of the patients with chronic liver disease and more commonly in females. The risk factors for the SAAs are arterial fibrodysplasia, multiparity, arteriosclerosis, pancreatitis, trauma, chronic liver disease and portal hypertension, the latter two being the commonest, as was in our case. The most common location of the aneurysm was the distal third of the splenic artery and the intra parenchymal branches. The increased concentration of few hormones may play a major role in the development of the aneurysms. The risk of the SAAs may increase with an increase in the patients’ age, the spleen size and the portal vein pathologies. The clinical significance of the SAAs is prevention of the fatal complications of the rupture, although they are rare. It is important to diagnose SAAs before liver transplantation because of their propensity for rupture in the post transplant period. Identifying the SAAs in the setting of the large dilated collaterals in the splenic hilum can be difficult by ultrasonography and by portovenous phase CT scan [1]. A dedicated arterial and venous phase CT should be performed to diagnose SAAs. SAAs can be treated with either an endovascular approach or a surgical approach. The endovascular treatment makes use of coiling or covered stents and the surgical treatment includes aneurysmectomy with or without splenectomy.
[1]. Ulu EM, Kirbas I, Emiroglu FK, Cakir B, Harman A, Bakar C, Multidetector CT findings of splenic artery aneurysms in children with chronic liver diseasePediatr Radiol. 2008 Oct 38(10):1095-98. [Google Scholar]