Anomalous Origin of the Hepatic Artery from the Hepatomesenteric Trunk
Poorwa Baburao Kardile1, Jaideo Manohar Ughade2, Manohar Namdeo Ughade3, Abhijeet Dhende4, Sayyed Sadiq Ali5
1 Assistant Professor, Department of Anatomy, Shri Vasantrao Naik Government Medical College, Yavatmal, Maharashtra, India.
2 Assistant Professor, Department of Anatomy, Shri Vasantrao Naik Government Medical College, Yavatmal, Maharashtra, India.
3 Professor and Head, Department of Anatomy, ACPM Medical College, Dhule, India.
4 Assistant Professor, Department of Anatomy, Government Medical College, Miraj, India.
5 Assistant Professor, Department of Anatomy, Government Medical College, Miraj, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Poorwa Baburao Kardile, Assistant Professor, Department of Anatomy, MANOHAR' Bunglow No 49, Dhamangaon Road, Yavatmal- 445001, Maharashtra, India.
Phone: 09404847887
E-mail: drpoorwakardile@yahoo.com
During the routine dissection of the abdominal cavity of a 75 years old, embalmed, male cadaver in the Department of Anatomy, an anomalous origin of the common hepatic artery from the hepatomesenteric trunk was observed. The Hepatomesenteric trunk originated from the ventral surface of the aorta at the L1 level. After coursing anteriorly, the trunk divided into the common hepatic artery and the superior mesenteric artery. The common hepatic artery is normally a branch of the coeliac trunk, but in the present case, the coeliac trunk gave two branches i.e. the left gastric and the splenic arteries. The length and the external diameter of the variant arteries were measured by using a Vernier calliper. The type V of Adachi's classification resembled closely with the variation which was observed. A knowledge on such a variation is important to avoid upheavals during surgical procedures. It is also helpful for the radiologists in interventional processes such as embolization of the hepatic artery and chemotherapy.
Superior mesenteric artery, Hepatomesentric trunk, Coeliac artery, Common hepatic artery
INTRODUCTION
The digestive tract is embryologically divided into three segments, based on the vascular supply which arises as the unpaired anterior branches of the abdominal aorta. The foregut is supplied by the coeliac trunk. The coeliac trunk is the first ventral branch of the abdominal aorta which arises at the level of T12. The classical trifurcation of the coeliac trunk into the left gastric, the common hepatic and the splenic arteries was first observed by Haller in 1756. It is thus known as Tripus Halleri, which is considered as a normal pattern [1]. The midgut is supplied by the superior mesenteric artery. The superior mesenteric artery is the second ventral branch of the abdominal aorta which arises at the level of L1.
Its normal branches include the inferior pancreaticoduodenal, jejunal, ileal, ileocolic, right colic and the middle colic arteries. The hindgut is supplied by the inferior mesenteric artery. The inferior mesenteric artery is the third ventral branch of the abdominal aorta which arises at the level of L2. Its normal branches include the sigmoidal, the left colic and the superior rectal arteries [2]. The anatomical variations in the coeliac trunk and the superior mesenteric arteries were first studied and classified by Adachi in 1928 [3].
In the present study, we noted an anomalous origin of the common hepatic artery from the hepatomesenteric trunk. A knowledge on the variations which concern the vascular supply of the digestive tract is of extreme clinical importance during the performance of hepatic and pancreatic surgeries.
CASE REPORT
During a careful dissection of the abdominal cavity of a 75 years old, embalmed, male cadaver in the Department of Anatomy, an anomalous origin of the common hepatic artery from the hepatomesenteric trunk was observed. These findings were photographed and schematic diagrams of the arteries were made. The length and the external diameter of the variant arteries were measured by using a Vernier calliper.
The common hepatic artery which is normally a branch of the coeliac trunk, variably arose from the Hepatomesenteric trunk. The Hepatomesenteric trunk originated from the ventral surface of the aorta at L1 level and it had a length of 3cm. The external diameter of the trunk, at its origin, was 7.8mm. After coursing anteriorly, the trunk divided into the common hepatic artery and the superior mesenteric artery, as has been shown in [Table/Fig-1]. The external diameter of the common hepatic artery at its origin was 6.2mm and that of the superior mesenteric artery was 6.8mm.The coeliac artery divided into the left gastric and the splenic arteries.
Showing anomalous origin of hepatic artery from Hepatomesentric trunk
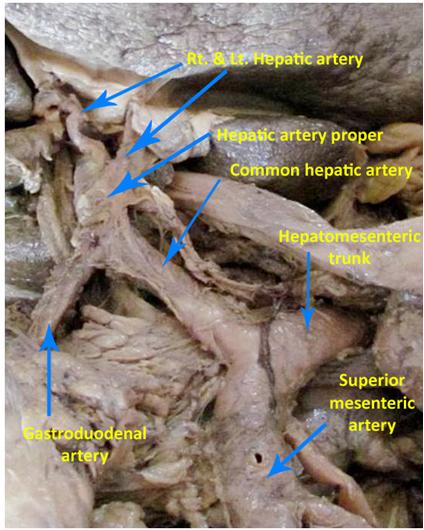
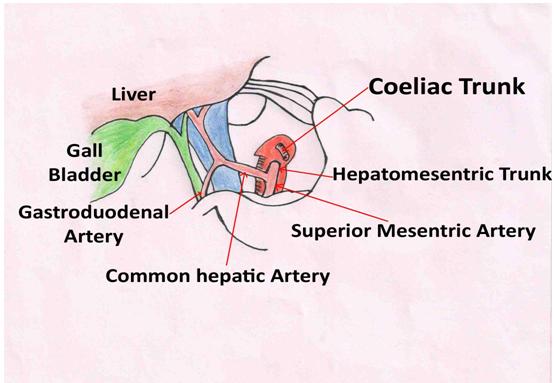
The common hepatic artery ascended laterally, anterior to the portal vein and it gave a gastroduodenal branch above the superior part of the duodenum, which then descended normally between the duodenum and the neck of the pancreas. The common hepatic artery, after giving a gastroduodenal branch, continued as the hepatic artery proper, which ascended to the portahepatis and divided into the right and left hepatic arteries and accompanied the portal vein and the hepatic duct, after giving the right gastric artery. The superior mesenteric artery further had a normal course and branches. The schematic diagram has been shown in [Table/Fig-2].
Schematic diagram of the anomalous Hepatomesentric trunk and its relations. (Adachi Type V)
DISCUSSION
There have been reports on the patterns of ramification of the coeliac trunk and the superior mesenteric artery, based on the Adachi (1928) classification, into six types. According to Adachi classification, the anomalies in which the hepatic artery arises from the hepatomesenteric trunk and passes anterior to the portal vein, at its origin ,belong to type V [3]. The present case reported a resembled Type V of Adachi. In accordance to our finding, Peschaud [4] et al., reported that the common hepatic artery usually passes in front of the portal vein when it originates as a branch of the hepatomesenteric trunk. Different researchers have reported this type in their studies to a varying extent, as has been shown in [Table/Fig-3]. This type of anomaly is rare and its incidence is not stable [5–7]. Almost a similar rare case was reported by Banerjee A et al., [8].
Incidence of type V pattern of Adachi
| Sr. No. | Author | Incidence in Percentage (No of Cases) |
|---|
| 1. | Akira Iimura et al., [5] | 0.4%(1 in 252) |
| 2. | Imakoshi [6] | 1.9%(2 in 107) |
| 3. | Shoumura [7] | 2%(9 in 450) |
The embryological discussions which are related to this anomaly were made by Tandler [9] and Morita [10]. Tandler provided an embryological explanation for the variations in the coeliac trunk and the superior mesenteric artery in 1904. The ventral branches develop initially from the abdominal aorta as paired vessels, which then coalesce in the median line to form the four roots for the gut. The four roots are connected by a ventral longitudinal anastomosis [9].
Normally, the first root forms the left gastric artery, the second root forms the splenic artery and the third root forms the common hepatic artery. The first three roots coalesce by the longitudinal anastomotic trunk to form the coeliac trunk. The superior mesenteric trunk develops from the fourth root, which migrates caudally with the ventral migration of the gut [3,7]. According to Morita, the anomalous ramification of the coeliac trunk and the superior mesenteric artery are due to the disappearance of the primitive ventral splanchnic arteries and their longitudinal anastomosis, as has been shown in [Table/Fig-4] [5,10].
Embryological basis of Anomalous Hepatomesentric trunk
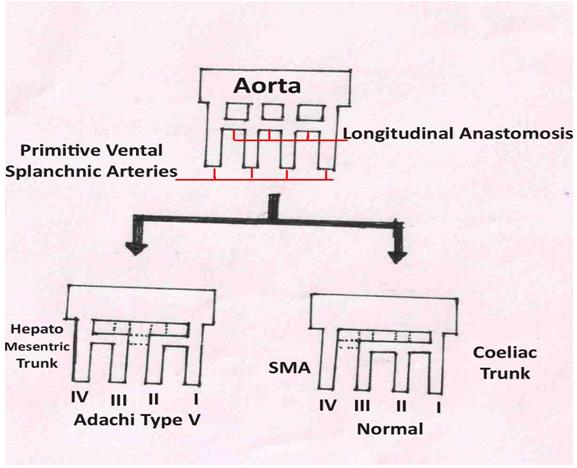
In the present case, due to the disappearance of the third root and the anastomosis between the second and the third root, which corresponded to the common hepatic artery, the hepatomesenteric trunk was formed from the fourth root, which corresponded to the superior mesenteric artery.
A knowledge on the variations in the coeliac trunk and the superior mesenteric artery are important in the Apple by procedure for carcinoma of the pancreas [11], laparoscopic surgeries, radiological procedures in the upper abdomen, interventional procedures like aortic replacements, chemoembolization of liver malignancies [12] and liver transplants [13].
[1]. Vandamme JP, Bonte J, The branches of the coeliac trunkActa Anat (Basel) 1985 122:110-14. [Google Scholar]
[2]. Gray H, Gray's Anatomy: The Anatomical Basis of clinical practice 2005 39thednElsevier Churchill Livingstone:1118 [Google Scholar]
[3]. Adachi B, Das Arterien Aystem Der Japaner, Band II. Kyoto: Verlag der Keiserlich-Japanischen Universitatzu Kyoto 1928 Maruzen Publishing Co:28:38:54(In Japanese) [Google Scholar]
[4]. Peschaud F, El-Hajjam M, Malafosse R, Goere D, Benoist S, Penna C, Nordlinger B, A common hepatic artery passing in front of the portal veinSurg. Radiol. Anat. 2006 28:202-05. [Google Scholar]
[5]. Iimura A, Oguchi T, Shibata M, Takahashi T, An anomalous case of the hepatic artery arising from the superior mesenteric arteryOkajimas Folia Anat. Jpn 2007 August 84(2):61-66. [Google Scholar]
[6]. Imakoshi K, Study of coeliac artery. Studies from the anatomical department of the Kanazawa medical college.(Thesis)1949; 37:1-14.(In Japanese)Cross ref from Banerjee A, Gupta AD, Kumar AI, Kumar PM, LAxmi PJ. Anomaly of Coeliaco-Mesenteric Axis: A Rare Arterial VariationJournal of Clinical and Diagnostic Research 2012 April 6(2):296-98. [Google Scholar]
[7]. Shomura S, Emua S, Anatomical study on the branches of the coeliac trunk (IV) comparison of the findings with Adachi's classificationActa Anat Nippon 1991 66:452-61. [Google Scholar]
[8]. Banerjee A, Gupta AD, Kumar AI, Kumar PM, Laxmi PJ, Anomaly of Coeliaco-Mesenteric Axis: A Rare Arterial VariationJournal of Clinical and Diagnostic Research 2012 April 6(2):296-98. [Google Scholar]
[9]. Tandler J, Uberdie Varietaten der arteriacoelia caunderen EntwiklungAnat Hefte 1904 25:473:500(In German) [Google Scholar]
[10]. Morita M, Reports and conception of three anomalous cases of the superior mesenteric arteriesIgaku Kenkyu 1935 9:1993:2006 [Google Scholar]
[11]. Lee SW, Shinohara H, Preoperative simulation of vascular anatomy by three dimensional computed tomography imaging in laparoscopic gastric cancer surgeryJ Am Coll Surg 2003 197(6):927-36. [Google Scholar]
[12]. Tsujimoto Y, Fukuda I, Kira M, Hepatic venous oxygen saturation monitoring indicated accidental resection of proper hepatic artery in a patient undergoing pancreatectomyThe Journal of Japan Society for Clinical Anesthesia 2004 24(9):412-15. [Google Scholar]
[13]. Ishigami K, Zhang Y, Rayhill S, Katz D, Stolpen A, Does Variant Hepatic Artery Anatomy in a Liver Transplant Recipient Increase the Risk of Hepatic Artery Complications After Transplantation?AJR 2004 183:1577-84. [Google Scholar]