Askin’s Tumour in an Adult, with a Varied Clinical Presentation
Arun Ramasamy1, M.R. Madan Karthik Raj2, Rekha Pobbi Shetty Radhakrishna3, Thirugnana Sambandan Veeramani4, Singaravelu M Chinniah5
1 Postgraduate Student, Department of General Surgery, Vinayaka Mission’s Kirupanada Variyar Medical College and Hospital, Chinnaseeragapadi, Salem, Tamil Nadu-636308, India.
2 Assistant Professor, Department of General Surgery, Vinayaka Mission’s Kirupanada Variyar Medical College and Hospital, Chinnaseeragapadi, Salem, Tamil Nadu-636308, India.
3 Associate Professor, Department of Pathology, Vinayaka Mission’s Kirupanada Variyar Medical College and Hospital, Chinnaseeragapadi, Salem, Tamil Nadu-636308, India.
4 Professor, Department of General Surgery, Vinayaka Mission’s Kirupanada Variyar Medical College and Hospital, Chinnaseeragapadi, Salem, Tamil Nadu-636308, India.
5 Professor, Department of General Surgery, Vinayaka Mission’s Kirupanada Variyar Medical College and Hospital, Chinnaseeragapadi, Salem, Tamil Nadu-636308, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arun R., Postgraduate Student, Department of General Surgery, Vinayaka Mission’s Kirupanada Variyar Medical College and Hospital, Chinnaseeragapadi, Salem, Tamil Nadu-636308 (India)
Phone: +919894428790
E-mail: drarunram@gmail.com
We are reporting a case of Askin’s tumour in a 28 year old male, on the right side of the chest wall, with no symptoms and signs of a pulmonary involvement or a distant metastasis. A wide excision of the tumour mass was done. Immunohistochemistry strongly expressed MIC-2. The prognosis of Askin’s tumour is poor. An early diagnosis and treatment are important to improve the chances of a survival.
Chest wall, Wide excision, MIC-2
INTRODUCTION
Primitive Neuroectodermal Tumour (PNET) of the chest wall or Askin’s tumour is a rare neoplasm of the chest wall. It was described by Askin et al in 1979. Askin’s tumor belongs to the Ewing’s family of tumours, which is characterized by a reciprocal chromosomal translocation, t(11:22) [1]. A primitive neuroectodermal tumour of the thoracopulmonary region probably occurs more commonly than is generally appreciated. This report emphasises its varied clinical presentation and the importance of cytology and histopathology, followed by immunohistochemistry in the diagnosis and the management of Askin’s tumour.
CASE REPORT
A 28 year old male patient without any significant past history, presented with a swelling and pain on the right side of the chest, which was there for the past 2 years and 6 months. On examination, a swelling of size, 25x20cm was seen on the right anterolateral part of the chest wall, with reddish pigmentation and dilated veins [Table/Fig-1]. The swelling was warm and tender, variable in consistency and had ill defined margins and it was fixed to the pectoralis major muscle. There were no palpable regional lymph nodes and no distal neurovascular deficit. The differential diagnoses of soft tissue sarcoma, chondrosarcoma, lymphoma, Ewing’s group of tumours and osteosarcoma were considered.
Photograph showing large mass with dilated veins and reddish pigmentation

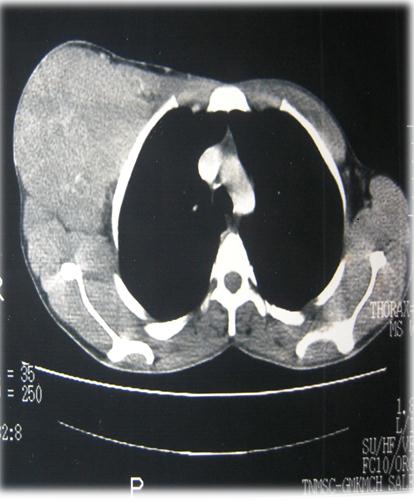
The PA view of an X-Ray of the chest showed a radio-opaque shadow which involved the right axilla and the chest wall. An ultrasonogram and Doppler of the right axilla revealed a solid mixed echogenic large lesion with internal vascularity. Computerized tomography of the upper chest revealed a large, well defined, heterogeneously enhancing, soft tissue mass which measured 13x12.2x14cm, with multiple specks of calcifications in the right upper anterior chest wall and mild enlargement of the axillary group of lymph nodes without invasion to the underlying bone [Table/ Fig-2]. Hence, the possibility of an osteosarcoma was ruled out. Therefore, fine needle aspiration studies were asked for, which were suggestive of a small, blue, round cell tumour of the chest wall and considering lymphoma, the Ewing’s group of tumours and a small cell variant of sarcoma as the differential diagnosis.
C.T upper chest showing a large,well defined heterogeneous mass with no bony erosion and pulmonary involvement.
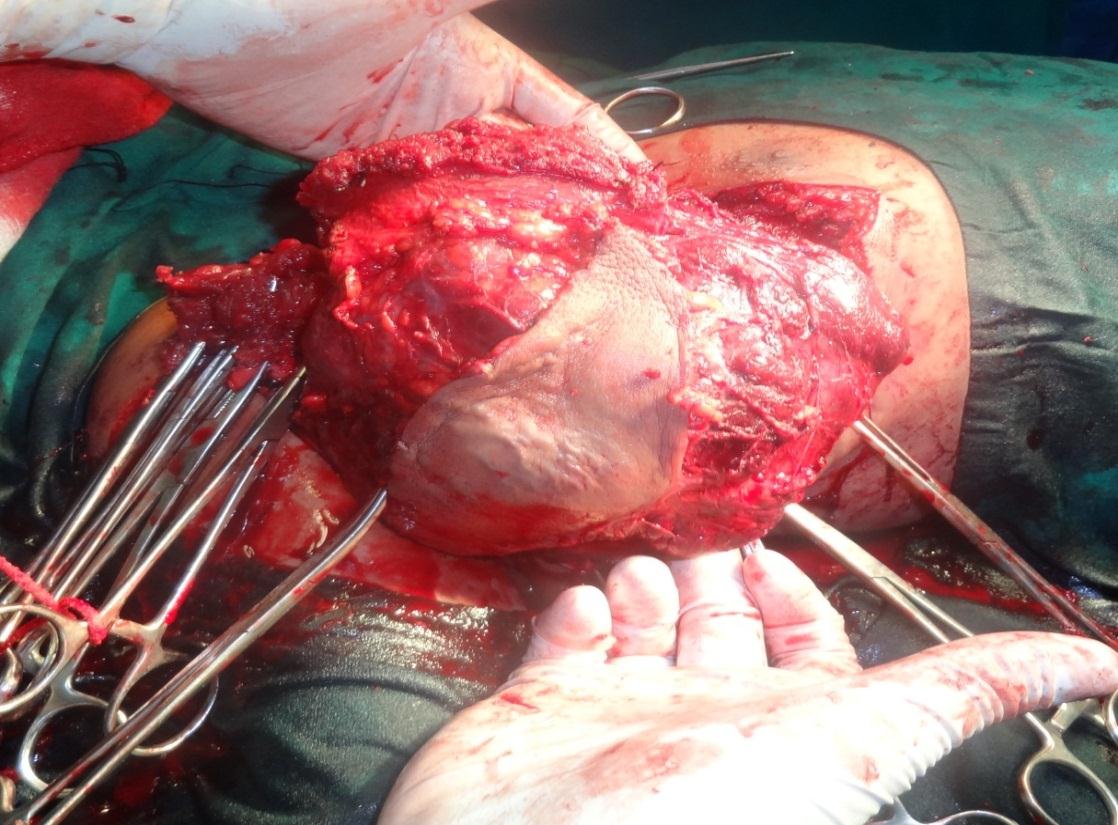
An oncologist’s opinion was obtained and a wide excision of the mass was done by making a transverse elliptical incision over the swelling. The intraoperative findings revealed that the tumour was adherent to the pectoralis major and minor muscle and that it had high vascularity [Table/Fig-3]. Superiorly, the mass was close to the axillary vein. The tumour mass was removed with 2-3cm free margins, along with a major part of the pectoralis major and minor muscle. The axillary fat and the axillary lymph node clearance was done upto Level II.
Photograph showing the tumour mass is being removed by wide excision
On gross examination , the mass was found to be capsulated and on cut section, it was found to be pinkish white in colour.
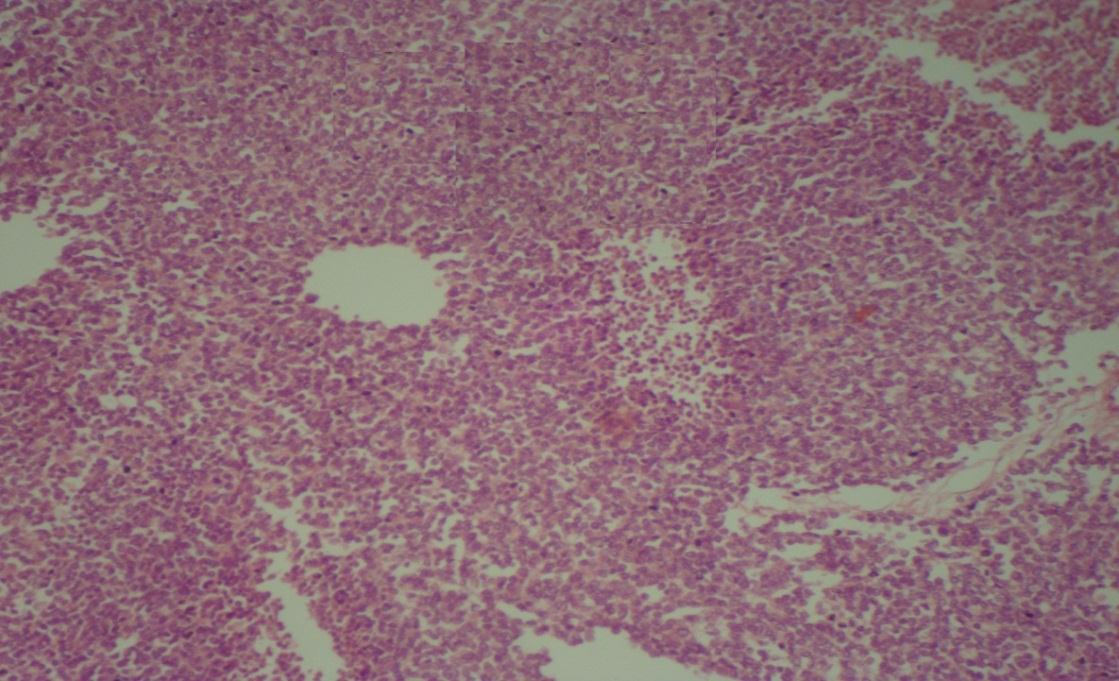
A microscopic examination revealed a tumour which comprised of small blue cells which were interspersed by blood vessels, The tumour cells were arranged in diffuse sheets and in clusters with areas of necrosis and few atypical mitotic figures. The resected margins showed an evidence of tumour cell infiltration [Table/Fig-4]. Immuno histochemistry revealed a strong expression of MIC-2 and the mass was immunonegative for Fli 1, Bcl2, WT 1 and desmin, thus confirming the diagnosis as an Ewing’s of group tumour. As the tumour arose from the chest wall without any bone involvement or invasion into the bone, a final diagnosis of Askin’s tumour was made. The patient recovered without any complications.
H&E(40X) showing small round cells in diffuse sheets and clusters
DISCUSSION
Askin’s tumour is a rare, malignant, small-cell neuroepithelioma that arises from the soft tissues of the chest wall or the lung and it predominantly occurs in children and in young adults who are in the age range of 10 to 30 years [2]. Askin et al. reported that, these tumours are common in females and that the median age for these is 14.5 years [3]. Our case was a 28 year old male with a rapid progression of the disease. A chest wall mass is the typical clinical presentation with or without pain [1]. Among the newly diagnosed patients, less than 25% have a pulmonary involvement and 20- 25% have distant metastases to the bone or the bone marrow [1,4]. Our patient presented with a chest wall mass and pain, with no symptoms and signs of a pulmonary involvement or distant metastases.
On plain radiography, Askin’s tumour commonly presents as a mass in the chest wall with soft tissue density. On computerized tomography, Askin’s tumour presents as a large ill defined mass with a heterogenous appearance, which often invades the surrounding tissues (local rib erosion) and with pleural effusions and pulmonary metastases. As a rule, there is no calcification [5]. In our case, it was a well defined, lobulated heterogenous mass with multiple specks of calcification. There was no evidence of a bony erosion or a pulmonary involvement.
An accurate diagnosis of Askin’s tumour poses a diagnostic challenge and it is imperative for both instituting the specific therapy and for the prognosis. Immunohistochemistry helps in distinguishing the primitive neuroectodermal tumours and the Ewing’s family of tumours from the other small, round cell tumours. The demonstration of a membrane-pattern positivity for MIC- 2(CD99), the neural markers (S-100, Synaptophysin) and vimentin and a negativity for the muscle markers confirms the diagnosis [6].
The treatment in Askin’s tumour consists of a radical surgery, neoadjuvant or adjuvant chemotherapy and radiotherapy. The long term survival can be improved with both local and adjuvant therapy in the form of multidrug chemotherapy. In a recent study, the overall 4 year survival rates for patients with locoregional and distant metastases were 89% and 17.8% respectively [4].
[1]. Verma Sanjeev, Prakash Prashant, Yadav Pushpa, Srivastava Dinesh, Sharma SC, Primitive Neuroectodermal Tumour of the Chest Wall in an AdultJIACM 2008 9(3):237-39. [Google Scholar]
[2]. Kransdorf Mark J, Murphey Mark D, Neurogenic tumours; Imaging of soft tissue tumors 2006 2ndPhiladelphia,USALippincot Williams and Wilkins:371-74. [Google Scholar]
[3]. Ozlem (Malas) Oru MD, Arzu Hocaoglu, MD, Benan Caglayan, MD, Ozdogan E Sevda, MD, Nusret Erdogan, MD, Askin Tumor : Malignant Round Cell Tumor in the Thoracopulmonary RegionTurkish Respiratory Journal 2002 3(3):109-12. [Google Scholar]
[4]. Hari MD, Jain T P, MD, Thulkar S, MD, Bakshi MD, DM, Pictorail review-Imaging features of peripheral primitive neuroectodermal tumoursThe British Journal of Radiology 2008 81:975-83. [Google Scholar]
[5]. de Schepper AMA, Parizel Paul M, Vanhoenacker Filip M, Primitive Neuroectodermal Leisons and Related LesionsImaging of Soft Tissue Tumors 2006 3rdGermanySpringer:379-84. [Google Scholar]
[6]. Gulati Maj D, Bahal Maj A, Dhar Col AK, Chakravorty Lt Col N, Muttagikar Brig MP, Lakhtakia Col R, Askin Rosai TumourMJAFI 2007 63:284-85. [Google Scholar]