An Epidermal Cyst in the Floor of the Mouth: A Rare Presentation
Suraj Mammen1, Anu Korulla2, M.J. Paul3
1 Department of Radiology, Department of Radiodiagnosis, Christian Medical College, Vellore, Tamil Nadu, India.
2 Department of Pathology, Department of Radiodiagnosis, Christian Medical College, Vellore, Tamil Nadu, India.
3 Department of Surgery, Department of Radiodiagnosis, Christian Medical College, Vellore, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Suraj Mammen, Assistant Professor, Department of Radiology, Christian Medical College, Vellore, Tamil Nadu-632004, India. Fax: 91-416 – 2232035 Email:surajmammen77@gmail.com
Epidermal cysts rarely occur in the head and neck region as compared to the dermoid cysts and when they do occur in this region, they present in the floor of the mouth. We are reporting a rare case of an epidermal cyst in the floor of the mouth, with a brief review of the literature.
Epidermal cyst, inclusion cyst
INTRODUCTION
Epidermal cysts are rare tumours under the spectrum of teratomas, with the absence of skin appendages within their squamous epithelium lined walls. The epidermal cysts in the head and neck region tend to occur in the floor of the mouth, though the frequency of their occurrence is unknown. These cysts tend to present in infancy or they may be uncommonly seen in the third and fourth decades of life, as has been presented in this case report. They may present as painless, slow growing swellings in the midline. Their characteristic Ultrasonography (USG) and Computerized Tomogram (CT) appearances help in narrowing down on the possible differential diagnoses, in thus providing the correct preoperative diagnoses and in facilitating an early surgical intervention.
CASE REPORT
A 57 years old man presented to the surgical outpatient services with a mildly painful, progressively increasing, midline swelling in the submental region, of three months duration. The examination of his neck revealed a 4 x 5cm cystic, firm, non-transilluminant swelling in the submental region. There were no palpable lymph nodes in the neck.
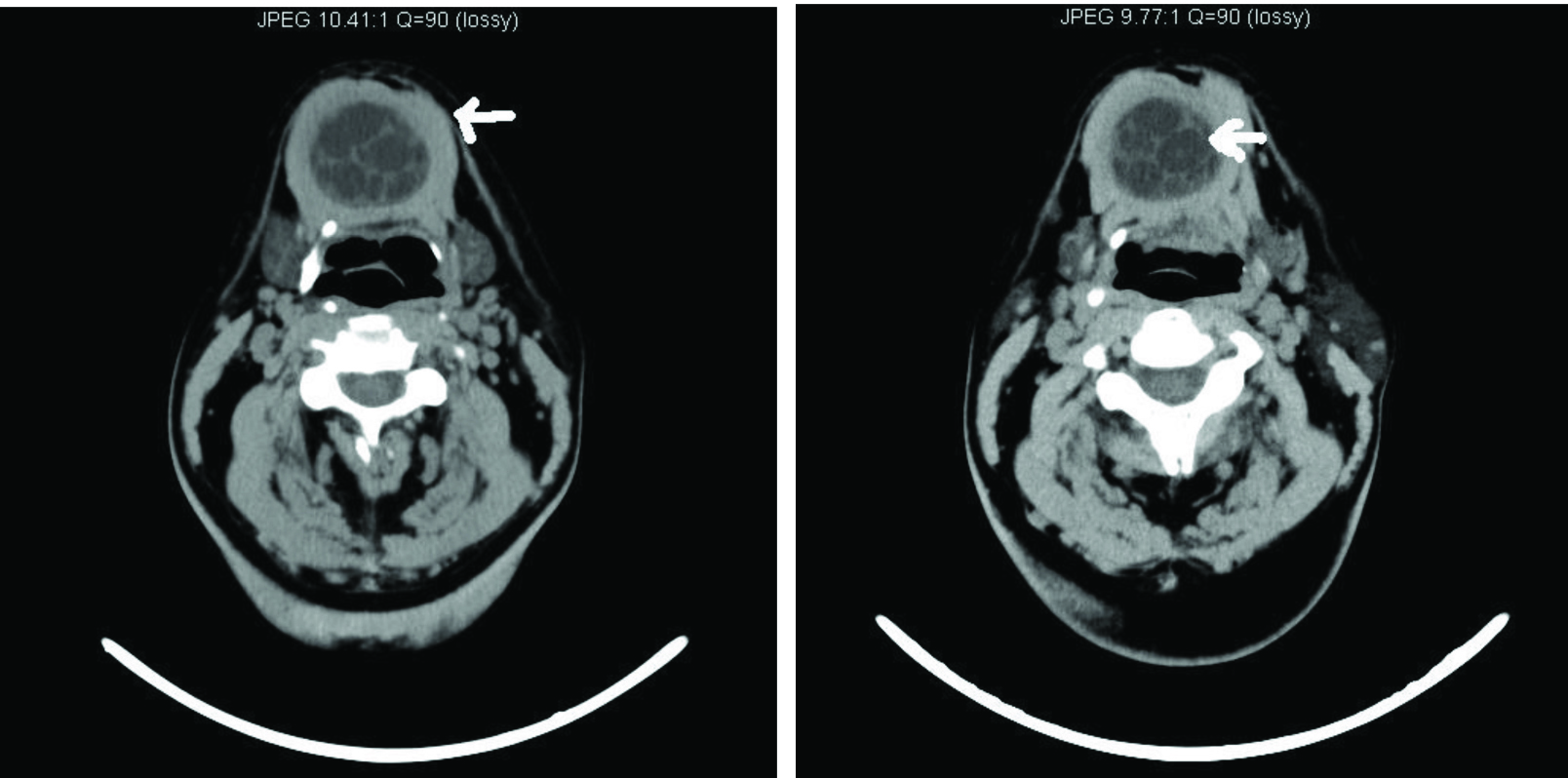
USG of the neck was done on a Philips HD 11 machine by using the 3-12 MHz linear probe. The USG was done through the submental approach in the axial and the sagittal planes and it revealed a 3 x 3.8cm, well-circumscribed, encapsulated cystic lesion in the submental region, which was located between the anterior bellies of the digastric muscles [Table/Fig-1] and below the mylohyoid muscle [Table/Fig-3]. It contained multiple echogenic coalescent nodules which were separated by anechoic areas, with specks of hyperechoic areas within the nodules [Table/Fig-1 and 2]. The nodules were found to be sparingly mobile within the lesion. The differential diagnoses of dermoid cyst, epidermal cyst and complicated ranula were considered. A non contrast CT was performed by using a Philips, Brilliance 6 slicer, to detect any lipid content within the lesion. The lesion had a central cavity with a homogenous, hypo-attenuating (0-18HU) fluid material which was filled with multiple “marbles” due to the coalescence of fat into the small nodules, thus giving a stack-of- marbles appearance, as has been described in the literature [1]. Fine needle aspiration smears which were performed from the submental lesion showed a mainly acute inflammatory exudate and a few benign squamous cells.
Ultrasonography A and B in the saggital and transverse plane show a well encapsulated fluid filled cavity, filled with multiple small nodules giving a stack of marble appearance; the nodules are due to the keratin sphere formation, axial section C depicts splitting of the anterior belly of digastic muscle D and mylohyoid M in the posterior aspect of the lesion.

Axial non contrast CT A(arrow) shows an encapsulated, hypo-attenuated mass lesion with partial adipose content, B (arrow) coalescence of the lipid material produces a stack-of marble appearance
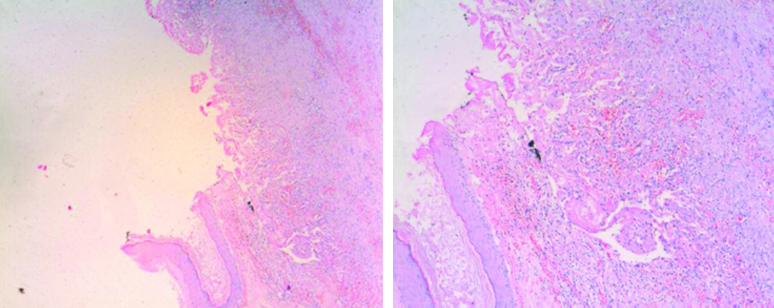
Photomicrograph A,X50 & B, X100 H&E, Low power view of the epidermal inclusion cyst specimen shows the cyst wall with extensive ulceration replaced by inflammatory granulation tissue. Lining stratified squamous epithelium seen in the lower part.
The cyst was completely removed by surgical excision by using a cervical approach and it was sent for a histopathological examination. The lesion had a thin wall and there was no evidence of dermal appendages. The lumen contained keratin material which was suggestive of an epidermal cyst. The striking sonographic appearance of the multiple echogenic nodules within the lesion was caused by multiple spherical keratin formations. The postoperative period was uneventful.
DISCUSSION
The term, “dermoid cyst” is ambiguously used for several different pathological entities which include benign cystic teratomas and various sequestration type cysts [1]. True dermoid cysts, epidermal cysts and teratoid cysts complete the spectrum of teratomas, and these are covered by squamous epithelium [2,3]. The aetiology of both the dermoid and the epidermal cysts is the failure of the surface ectoderm in separating from the underlying structures, resulting in the sequestration and the implantation of the surface ectoderm [2]. There is no gender predilection for epidermal cysts. The most common cervical location of the dermoid and the epidermal cysts is the floor of the mouth. They present as soft, mobile and slow growing masses and they are unattached to the overlying skin. They have no intimate association with the hyoid bone; hence, they do not tend to move on the protrusion of the tongue [1].
The gross specimen of an epidermal cyst is often described as a “pearly tumour” because of the shiny, smooth and waxy character of its “dry keratin.” Histologically, epidermal cysts are lined by a thin squamous epithelium and they are rarely calcified. These cysts contain debris from the desquamating lining epithelium, keratin and cholesterol [2,4].
Ultrasonographically they have solid and cystic structures within a heterogeneous mass, rarely with calcifications [5]. On CT scans, they are found to be moderately thin walled, unilocular masses which are filled with a homogeneous, hypoattenuating (0–18 HU) fluid material, with multiple hypoattenuating fat nodules, giving a “sack-of-marbles” appearance, which is virtually pathognomonic for the dermoid cysts in this location [1]. However, an epidermal cyst may also show similar findings. Fluid-fluid levels with supernatant lipid may be seen. The rim of these cysts often enhances following the administration of a contrast material [1].
The treatment involves complete surgical excision without rupturing the cyst, as the contents may act as irritants to the surrounding fibrovascular tissue, producing postoperative inflammation [6]. A recurrence is unlikely after a complete surgical excision.
CONCLUSION
This is a rare case of an epidermal cyst in the floor of the neck. Such cysts are often slow-growing masses and they cause symptoms only after they enlarge sufficiently or when they are infected. Ultrasonography is frequently used initially to confirm the nature of the lesion, while CT may be used for the optimal preoperative assessment and planning. However, an ultrasonographic evaluation can sometimes give all the necessary information for a surgical intervention, as in our case. The only important issue is determining the relationship of the lesion to the mylohyoid muscle, to plan the surgical approach.
[1]. Hunter T, Paplanus S, Chernin M, Coulthard S, Dermoid cyst of the floor of the mouth: CT appearanceAJR 1983 141:1239-40. [Google Scholar]
[2]. Smirniotopoulos J, Chiechi M, Teratomas, dermoids, and epidermoids of the head and neckRadio Graphics 1995 15:1437-55. [Google Scholar]
[3]. Koeller KK, Alamo L, Adair CF, Smirniotopoulos JG, Congenital Cystic Masses of the Neck: Radiologic-Pathologic CorrelationRadiographics 1999 19:121-46. [Google Scholar]
[4]. Coit W, Harnsberger H, Osborn A, Smoker W, Stevens M, Lufkin R, Ranulas and their mimics: CT evaluationRadiology 1987 163:211-16. [Google Scholar]
[5]. Meuwly J, Lepori D, Theumann N, Schnyder P, Etechami G, Hohlfeld J, Multimodality Imaging Evaluation of the Pediatric Neck: Techniques and Spectrum of FindingsRadio Graphics 2005 25:931-48. [Google Scholar]
[6]. Dimov Zh, Dimov K, Kr’stev N, Kr’stev D, Baeva M, Baeva N, Dermoid, epidermoid and teratoma cysts of the tongue and oral cavity floorKhirurgiia (Sofiia) 2000 56(2):30-32. [Google Scholar]