Stromal Endometriosis of the Intestine: An Elusive Presentation with A Review of the Literature: A Case Report
Shashi Upreti1, Rani Bansal2, Sanjay Upreti3, Shiva Mathur4
1 Assistant Professor, Department of Pathology,
2 Professor and Head, Department of Pathology,
3 Assistant Professor, Department of Pathology,
4 Junior Resident, Department of Pathology, Subharti Medical College, Meerut U.P., India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shashi Upreti, Assistant Professor, Department of Pathology, Subharti Medical College, Meerut Haridwar Bypass Road, Meerut, U.P., India.
Phone: 09917352266
E-mail: drsanjayupreti@gmail.com
Although endometriosis involves the small intestine only rarely, when present, this condition may simulate a variety of inflammatory and sometimes neoplastic conditions because of its nonspecific symptoms. We are reporting here, a case of ileal, caecal and appendiceal endometriosis which presented in the emergency as a case of an acute intestinal obstruction with a long history of symptoms which were referable to the GI tract. The patient had the diffuse involvement of a segment of the ileum with mural thickening and luminal narrowing, which led to obstruction. The literature on small bowel endometriosis has been reviewed and the clinical and pathological features have been discussed.
Stromal endometriosis, CD 10, Endometrial stromal sarcoma
INTRODUCTION
Endometriosis is the presence of heterotopic endometrium outside the uterus. Though this condition is frequent in the western world, it is much less frequent in India [1]. Small bowel endometriosis occurs in 1-10 % of the patients, as has been reported in the western literature [2]. The prevalence of appendiceal endometriosis is 2-8% [3], followed by the ileum and the caecum. In a majority of the cases, it is unassociated with the clinical manifestations which are referable to the intestinal tract. The endometriosis which lacks glandular components and in which only stroma is present, is known as stromal endometriosis. Stromal endometriosis poses a problem in the diagnosis, especially when it is present outside the pelvis. Misdiagnoses are also common because of the decreased index of suspicion. We are presenting here, a case of intestinal stromal endometriosis.
CASE HISTORY AND OBSERVATIONS
A 40 years old lady presented to the emergency department with subacute intestinal obstruction. She complained of, on and off vomiting, abdominal discomfort and constipation of 3-4 months duration, loss of weight and appetite for one year, and polymenorrhoea of 1 ½ years duration. An ultrasonography which was done six months ago, was suggestive of pelvic inflammatory disease (? tubercular aetiology) An emergency laparotomy and an ileostomy were performed. The specimen was sent for a histopathological examination. The post operative period was uneventful. She was discharged and was re-admitted for ileostomy closure 10 weeks later. She is asymptomatic and on regular follow up, seven months after the surgery.
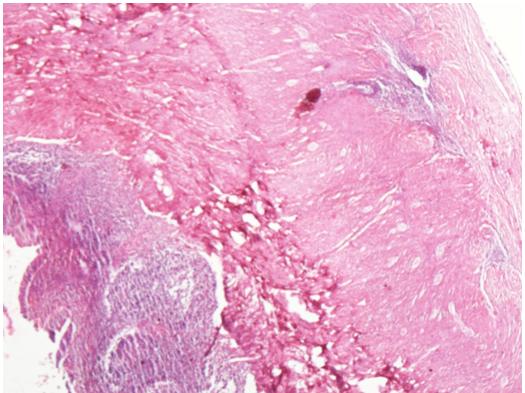
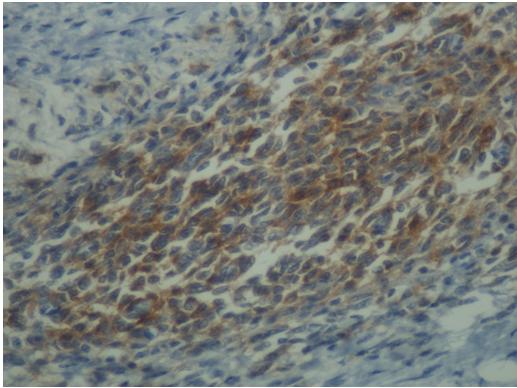
The resected specimen of the intestine, which included a part of the ileum, caecum and the appendix, measured 55 cms in length. The outer surface showed multiple grey white to grey brown tiny pin head sized nodular areas on the serosal surface. At the caecal end, the lumen was narrowed. No perforations were identified. The mucosa was unremarkable. The appendix also showed tinypale white nodules on the serosal aspect. No lymph nodes were present. The microscopic examination revealed chronic serositis and fibrosis with a mixed inflammatory cell infiltrate. Small collections of endometriotic stroma which were surrounded by dilated and congested capillaries and areas of haemorrhage were present in the subserosa, periserosa, mesentry and in the muscularis propria [Table/Fig-1] of the ileum, caecum and the appendix. The mucosa and the submucosa were unremarkable.. CD 10 staining showed a diffuse positivity in the endometriotic stromal cells [Table/ Fig-2].
Focus of stromal endometriosis in outer muscle layer of ileum
Positive CD10 immunostaining in endometriotic stromal cells
DISCUSSION
Endometriosis is uncommon in our country or may be, under reported. A symptomatic involvement of the small bowel occurs infrequently, causing a partial or complete obstruction by kinking the lumen or by forming a mass. Involvement of the appendix may lead to symptoms of acute appendicitis [4].
Small bowel endometriosis tends to affect the serosa and the deposits are not usually larger than 2 cm in size. It is usually characterized by a patchy involvement [5]. However, in our case, microscopically, both continuous and patchy involvement were seen, which involved the serosa and the muscular layer. In this case, a history of a mild to moderate diffuse abdominal pain with distension, was present. The intestinal symptoms were associated with menorrhagia, which is commonly seen in perimenopausal women. The patient had an elevated ESR and a mildly elevated total leukocyte count. As ours is a tuberculosis endemic country, and due to the nonspecific chronic symptoms, a clinical diagnosis of tubercular pelvic inflammatory disease and a tubercular intestinal obstruction was suggested.
Associated acute bowel obstruction is a rare event which is reported in less than 1% of the intestinal endometriosis cases and it usually affects the rectosigmoid colon [6]. Small bowel obstructions have been observed in only 0.7% of all the surgical interventions which are carried out for endometriosis [6], Our case presented with acute small bowel obstruction and it required an emergency surgical intervention. A clinical diagnosis of small bowel endometriosis is difficult because of the different acute and chronic nonspecific symptoms, as it was in our case.
The clinical symptoms and signs of endometriosis may mimic different pathological conditions such as inflammatory bowel disease, acute appendicitis, intestinal tuberculosis, ischaemic enteritis and tumours. The most common symptom of enteric endometriosis is colicky abdominal pain with other common symptoms such as nausea, vomiting, pyrexia, constipation, weight loss and anorexia, which often have a low diagnostic validity [7, 8].
The true incidence of endometriosis which causes bowel obstruction is unknown [9] although a complete obstruction occurs in < 1% of all the cases [10]. In stromal endometriosis, the ectopic foci of the endometrium are usually seen without the glandular elements, with extravasation of the red blood cells and a prominent vascularity, which is an under-recognized form of endometriosis [11]. This is difficult to diagnose, if it is present focally and is not associated with a high degree of pathological suspicion.
Because of the pure or almost pure stromal composition of the lesion, it can be confused histologically with benign and malignant neoplasms, particularly low grade endometrial sarcoma (ESS) and Kaposi's sarcoma [12]. The differentiation of stromal endometriosis from low grade ESS is important. On light microscopy, low grade ESS has been found to have infiltrating margins and it typically shows a worm like vessel invasion [13] as compared to stromal endometriosis, which has well circumscribed boundaries. A mitotic activity is typically seen in ESS, which is < 3/ 10 hpf in the low grade type of disease.. The intestinal forms are usually seen in the subserosal and the muscular layers, which are associated with muscle hypertrophy. CD10 is a sensitive and a diagnostically useful marker of the normal as well as neoplastic endometrial stromal cells. It shows a diffuse cytoplasmic positivity in the stromal cells but not in the glands. Wherever there is a diagnostic doubt, immunohistochemical (IHC) staining with CD 10 may be useful for identifying the endometrial stroma (which otherwise lacks the characteristic IHC marker) and for confirming the diagnosis of endometriosis [14,15].
To conclude, endometriosis should be considered in the differential diagnosis in women with gynaecological and unexplained gastrointestinal symptoms.
[1]. Haubrich WS, Enteric endometriosis. In: JE Berk, WS Haubrich, MH Kalser, JLA Roth, F Schaffner, editorsBokus Gastroenterology 1985 PhiladelphiaWB Saunders Co:2484-89. [Google Scholar]
[2]. Martimbeau PW, Pratt JH, Gaffey TA, Small-bowel obstruction secondary to endometriosisMayo Clinic Proc 1975 50:239-43. [Google Scholar]
[3]. Offodile A, Hodgin JB, Arnell T, Asymptomatic intussusception of the appendix secondary to endometriosisAm Surg. 2007 73:299-301. [Google Scholar]
[4]. LiVolsi VA, Perzin KH, Endometriosis of the small intestine producing intestinal obstruction or simulating neoplasmDigestive diseases and sciences 1974 19(2):100-8.DOI: 10.1007/BF01072618 [Google Scholar]
[5]. Anaf V, El Nakadi I, Simon P, Van de Stadt J, Fayt I, Simonart T, Preferential infiltration of large bowel endometriosis along the nerves of the colonHum Reprod. 2004 19:996-1002. [Google Scholar]
[6]. Beltran MA, Tapia QTF, Araos HF, Martinez GH, Cruces KS, Ileal endometriosis as a cause of intestinal obstructionReport of two cases: Rev Med Chil 2006 134:485-90. [Google Scholar]
[7]. Slesser AS, Kubba F, Selluet D, Acute small bowel obstruction secondary to intestinal endometriosis an elusive condition: a case reportWorld J Emerg Surg. 2010 5:27 [Google Scholar]
[8]. Teke Z, Aytekin FO, Atalay AO, Demirkan NC, Crohn's disease complicated by multiple stenoses and internal fistulas clinically mimicking small bowel endometriosisWorld JGastroenterol 2008 14:146-51. [Google Scholar]
[9]. Paksoy M, Karabicak I, Ayan F, Aydogan F, Intestinal obstruction due to rectal endometriosisMt Sinai J Med. 2005 72(6):405-08. [Google Scholar]
[10]. de Bree E, Schoretsanitis G, Melissas J, Christodoulakis M, Tsiftsis D, Acute intestinal obstruction caused by endometriosis mimicking sigmoid carcinomaActa Gastroenterol Belg 1998 61:376-08. [Google Scholar]
[11]. Boyle DP, McCluggage WG, Peritoneal stromal endometriosis: a detailed morphological analysis of a large series of cases of a common and under-recognised form of endometriosisJ Clin Pathol 2009 62:530-03. [Google Scholar]
[12]. Sumathi VP, McCluggage WG, CD10 is useful in demonstrating endometrial stroma at ectopic sites and in confirming a diagnosis of endometriosisJ Clin Pathol 2002 55:391-92. [Google Scholar]
[13]. McCluggage WG, Sumathi VP, Maxwell P, CD10 is a sensitive and diagnostically useful immunohistochemical marker of normal endometrial stroma and of endometrial stromal neoplasmsHistopathology 2001 39:273-78. [Google Scholar]
[14]. Clement Philip B, Young Robert H, Stromal endometriosis of the uterine cervix : A variant of endometriosis that may simulate sarcomaAm J of Surg Pathol May 1990 14(5):449-55. [Google Scholar]
[15]. Tavassoli FA, Devilee P, WHO classification of Pathology and genetics of tumours of the breast and female genital organs. In : Tavassoli FA, Devilee. P, editors 2003 Lyon,FranceIARC. Press:233-36. [Google Scholar]