An Interesting Case of a Subcutaneous Nodule
Basavaprabhu Achappa1, Deepak Madi2, Soundarya Mahalingam3
1 Associate Professor, Department of General Medicine, Kasturba Medical College, Mangalore (affiliated to Manipal University), India.
2 Assistant Professor, Department of General Medicine, Kasturba Medical College, Mangalore (affiliated to Manipal University), India.
3 Associate Professor, Department of Paediatrics, Kasturba Medical College, Mangalore (affiliated to Manipal University), India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepak Madi, Assistant Professor, Department of General Medicine, Kasturba Medical College,(affiliated to Manipal University) Attavar, Mangalore-575001, India.
Phone: 9845609148
E-mail: deepakmadi1234@gmail.com
Human dirofilariasis is a zoonotic disease which is caused by the filarial nematodes, Dirofilaria repens and Dirofilaria immitis. Dirofilariae are transmitted to humans via mosquito bites. Human Dirofilariasis presents commonly as subcutaneous nodules, pulmonary nodules or nodules in the eyes. They are considered as emerging pathogens. We are presenting a case of human Dirofilariasis from Karnataka, which was caused by Dirofilaria repens.
Dirofilariasis, Dirofilaria repens
INTRODUCTION
Dirofilariasis is caused by filarial nematodes. It is a zoonotic infection which is caused by D.immitis, D.repens, D tenuis and D.ursi. It is transmitted to humans by the Culex, Aedes or the Anopheles mosquitoes, which ingest the blood-containing microfilaria from affected dogs. Human Dirofilariasis is rare. It usually presents with nodular lesions in the lung, the subcutaneous tissues or the eyes. The reported cases of the Dirofilaria infection in humans are mainly caused by 2 species, Dirofilaria immitis (D.immitis) and Dirofilaria repens. We are presenting a case of human Dirofilariasis from Karnataka, which was caused by Dirofilaria repens.
CASE REPORT
A 48 year old female presented to our institution with a subcutaneous nodule above her left eye of 4 month’s duration. The nodule enlarged gradually. Her physical examination showed a well-defined, nontender and oval shaped nodule which was about 2 × 2 centimetre in size.
Her lab investigations showed Hb -12.9g/dl, Total White Blood Cell count - 5900 cells/cu.mm, Differential count– N-65, L-28, E-6, M-1 and ESR- 13mm/1st hour. Her chest X-ray was normal.
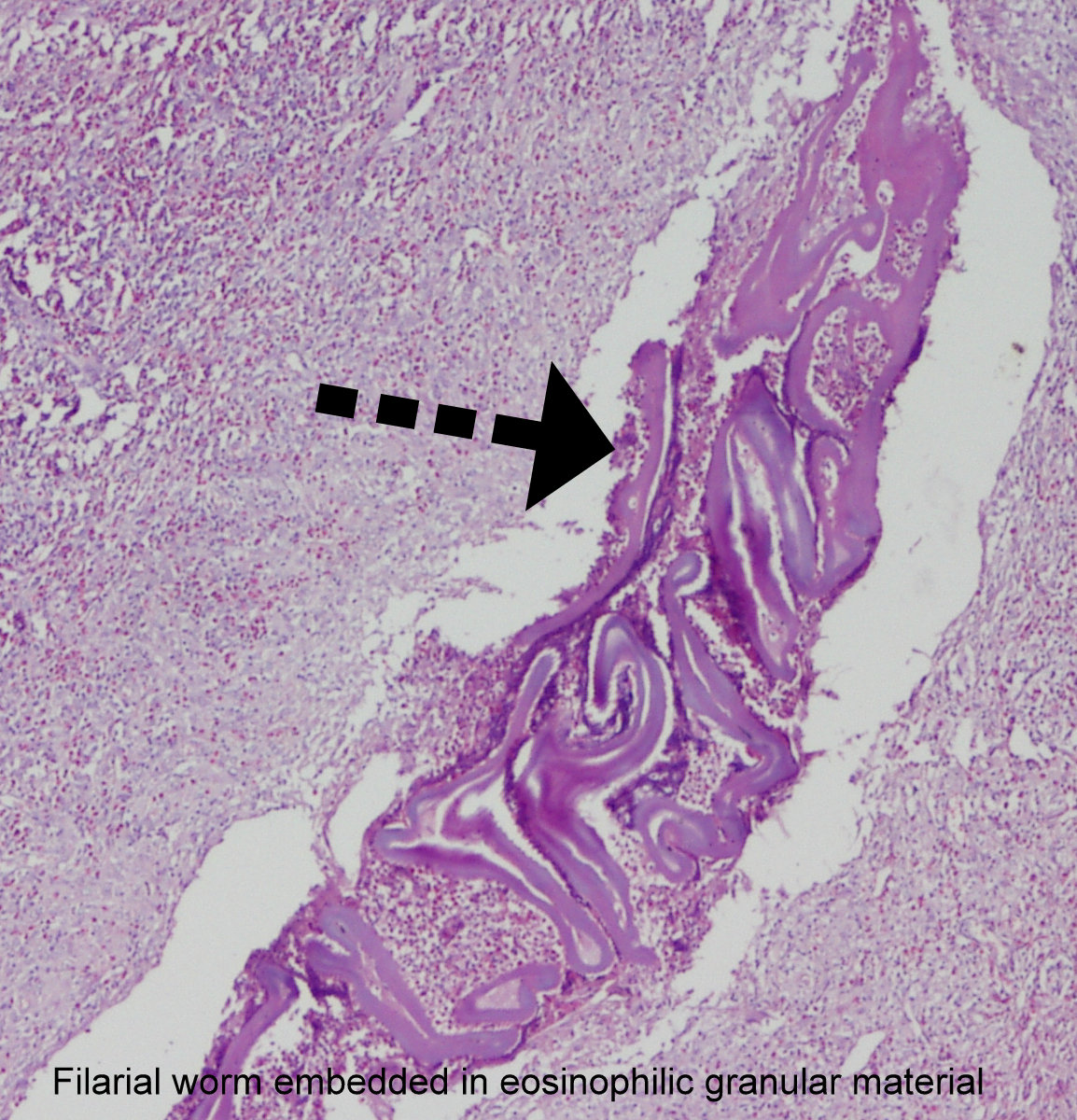
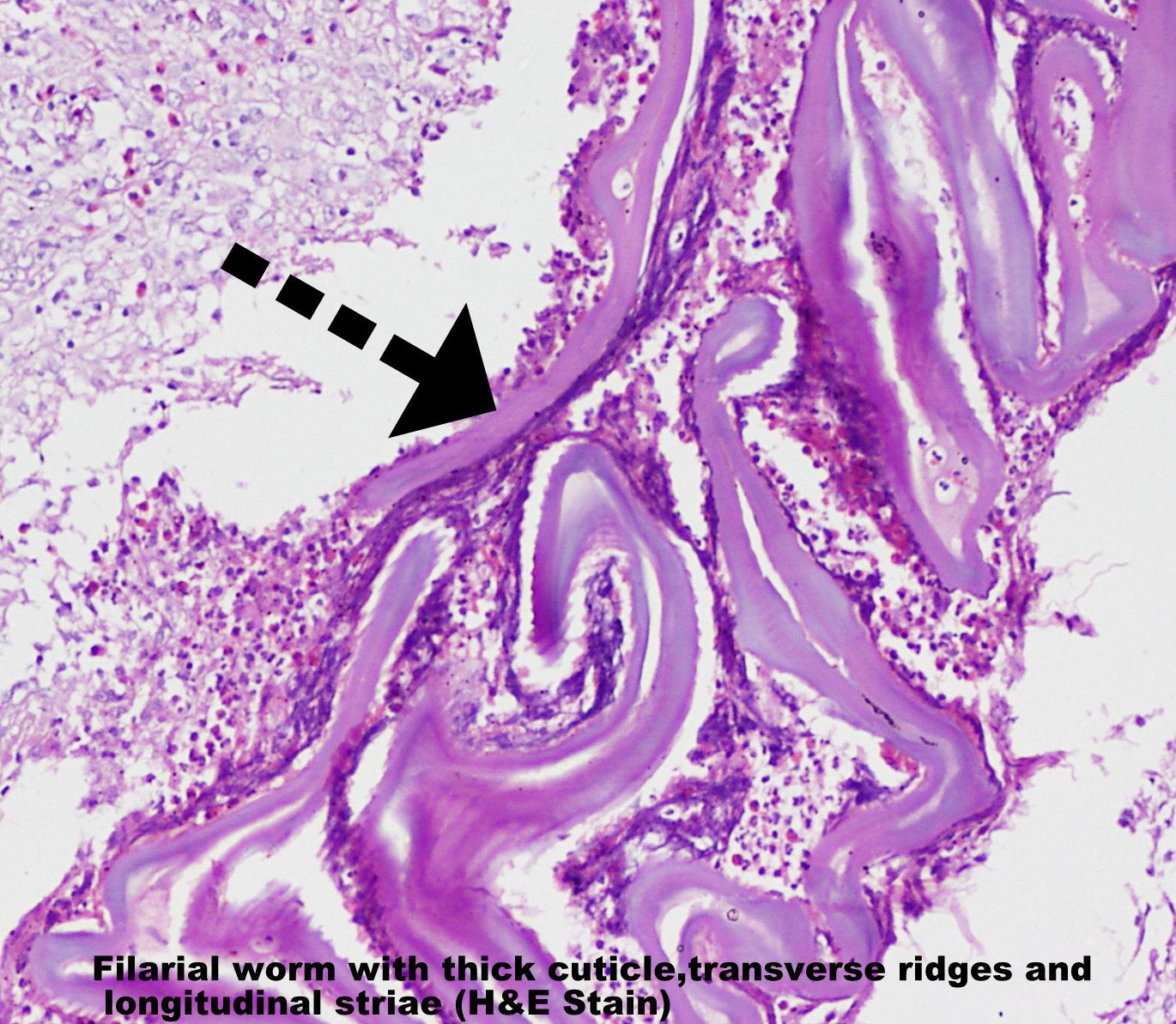
An excision biopsy of the nodule was performed. The gross examination revealed 2 irregular pale brown tissues that measured 0.6 cm and 1.8 cm in diameter. There was no evidence of calcification within the nodule. The pathological examination revealed a nematode which was embedded in the eosinophil rich granular material [Table/Fig-1 and 2]. Under the microscope, the nematode was found to have a thick laminated cuticle which had prominent longitudinal ridges and transverse striations. The worm was identified as Dirofilaria repens, based on its morphology.
Filarial worm embedded in eosinophilic granular material
Filarial worm with thick cuticle, transverse ridges and longitudinal striae
DISCUSSION
Though human Dirofilariasis is rare, the number of cases of Dirofilariasis which are caused by Dirofilaria repens has been increasing worldwide over the last decade. In India, cases of human Dirofilariasis are being reported from Karnataka [1], Kerala [2], Tamil Nadu [3] and Assam [4]. The definitive hosts of Dirofilaria repens and Dirofilaria immitis are dogs, but other animals have also been reported as the reservoirs of this disease (cats and bears).
The vectors for this parasite are mosquitoes (Culex and Anopheles) [5]. The adult female worms of D. repens release microfilariae into the circulation of the infected animals, which are ingested by the vectors during a blood meal [6]. An accidental human infection results in a subcutaneous mass anywhere in the body, preferentially around the eye. In response to the infection, an inflammatory granulomatous reaction develops. The adult worms do not reach maturity in humans and they do not produce microfilaria.
Human Dirofilariasis can be classified as pulmonary and extrapulmonary Dirofilariasis. Extra-pulmonary Dirofilariasis is classified further into: subcutaneous, visceral, and ophthalmic Dirofilariasis [7]. D. repens usually resides subcutaneously, while D. immitis frequently ends up in the lung. Khurana et al have reported three cases of human subcutaneous Dirofilariasis from India [8].
The diagnosis is confirmed by studying their morphologies after their removal. The worms which belong to the genus, Dirofilaria are identified by their thick laminated cuticle, broad lateral ends and large muscle cells. D.immitis can be differentiated from D. repens by the absence of ridges [3]. An accurate diagnosis can also be made by a PCR-based DNA analysis [9]. A PCR based DNA analysis was not done in our case.
A complete surgical excision of the lesion is the treatment of choice for the patients with human Dirofilariasis. Chemotherapy is not necessary as microfilaraemia is extremely rare [10]. Dirofilariasis is considered an emerging zoonotic disease [11]. An increased awareness on this emerging zoonotic infection in India among doctors will help in the early detection of this disease.
CONCLUSION
This case report suggests that Dirofilariasis should be considered as a differential diagnosis in the patients who present with subcutaneous nodular lesions.
[1]. Nadgir S, Tallur SS, Mangoli V, Halesh LH, Krishna BV, Subconjunctival dirofilariasis in IndiaSoutheast Asian J Trop Med Public Health 2001 32:244-46. [Google Scholar]
[2]. Ittyerah TP, Mallik D, A case of subcutaneous dirofilariasis of the eyelid in the South Indian state of KeralaIndian J Ophthalmol 2004 52:235 [Google Scholar]
[3]. Sathyan P, Manikandan P, Bhaskar M, Padma S, Singh G, Appalaraju B, Subtenons infection by DirofilariarepensIndian J Med. Microbiol 2006 24:61-62. [Google Scholar]
[4]. Nath R, Gogoi R, Bordoloi N, Gogoi T, Ocular dirofilariasisIndian J Pathol Microbiol 2010 53:157-59. [Google Scholar]
[5]. Athari A, Zoonotic subcutaneous dirofilariases in IranArchives of Iranian Medicine 2003 6:63-65. [Google Scholar]
[6]. Joseph K, Vinayakumar AR, Criton S, Vishnu MS, Pariyaram SE, Periorbital mass with cellulitis caused by dirofilariaIndian J Med Microbiol 2011 29:431-33. [Google Scholar]
[7]. Akao N, Human dirofilariasis in JapanTrop Med Health 2011 39:65-71. [Google Scholar]
[8]. Khurana S, Singh G, Bhatti HS, Malla N, Human subcutaneous dirofilariasis in India: A report of three cases with brief review of literatureIndian J Med Microbiol 2010 28:394-96. [Google Scholar]
[9]. Cancrini G, Prieto G, Favia G, Giannetto S, Tringali R, Pietrobelli M, Serological assays on eight cases of human dirofilariasis identified by morphology and DNA diagnosticsAnn Trop Med Parasitol. 1999 93:147-52. [Google Scholar]
[10]. Padmaja P, Kanagalakshmi Samuel R, Kuruvilla PJ, Mathai E, Subcutaneous dirofilariasis in southern India: A case reportAnn Trop Med Parasitol 2005 99:437-40. [Google Scholar]
[11]. Azari-Hamidian S, Yaghoobi-Ershadi MR, Javadian E, Mobedi I, Abai MR, Review of dirofilariasis in IranJ Med Facul Guilan Univ Med. Sci 2006 15:102-13. [Google Scholar]