Multiple Musculovascular Anomalies in the Superior Extremities of a Cadaver: A Case Report
Rajan Kumar Singla1, Rimpi Gupta2, Kanika Sachdeva3
1 Additional Professor, Department of Anatomy, Government Medical College, Amritsar-143001, Punjab, India.
2 Assistant professor, Dept of Anatomy, BPS Govt Medical College for Women, Khanpur Kalan, Sonipat, Haryana, India.
3 Assistant Professor, Department of Anatomy, Chintpurni Medical College, Pathankot, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajan Kumar Singla, 79, S.G. Enclave, Majitha Road, Amritsar-143001, India.
Phone: 9872477073, 08146669505. E mail: rajananat@gmail.com
During the evolution from the lower animals to man, the upper limbs have acquired a great mobility, but at the cost of their stability. The reverse is true for the lower limbs. The muscular anomalies which are common in the upper limbs are largely explainable on a phylogenetic basis. The same is true for the vascular anomalies. However, such anomalies are usually seen singly and they are never together in the same limb or in two limbs of the same body. The upper limbs which are being reported here had multiple musculovascular anomalies and some of these were bilateral. These include the superficial brachial artery, the accessory head of the biceps brachii, the accessory muscular slips which arose from the common flexor origin and went to the tendons of the flexor digitorum profundus and the flexor pollicis longus separately, bifurcation of the tendon of insertion of the brachioradialis and bifurcated (split) insertion of the third lumbrical on the adjacent fingers. Though all these variations have been described in the standard text books of Anatomy, their occurrence, together in one limb and the bilateral presentations of some of these, have never been encountered. Almost all these variations have been explained phylogenically, thus supporting the dictum, “The ontogeny repeats the phylogeny.” Furthermore, their clinical significance has also been discussed.
Upper limbs, Biceps brachii, Flexor digitorum profundus, Flexor pollicis longus, Brachioradialis, Lumbricals, Superficial brachial artery
INTRODUCTION
The human upper limbs, with a mobile basal shoulder girdle, an extensible folding arm and a forearm and a terminal working tool, the hand, have an extraordinary range and versatility of movement. Being pre-eminently adapted for reaching, grasping and manipulating, it has also much potentiality for other activities: pushing and adjusting objects without grasping, striking blows and supporting the body in endless positions. During the evolution, it has undergone various modifications, one of which is the lateral rotation of the forelimbs at the joints, with the pectoral girdle [1]. As it has been freed from weight bearing functions, its stability was sacrificed to achieve a mobility. This mobility is especially marked in the hands and fingers, but to a lesser extent, it is present throughout the upper limb [2].
The muscular anomalies are common in the upper limbs and there is much speculation, which is largely based on phylogenetic studies, concerning their significance. A concept which seems to be popular is that the major anomalies may result from small disturbances of the normal development, which occur at the critical stages. Such disturbances affect the muscle development more in the upper limb than in the lower limb, as the latter lags behind the former in development [3].
Sarikcioglu and Yildrim [4] described the coexistence of muscular, neural and vascular anomalies in the upper limb and emphasized that the variations within one system of the limb frequently occur in conjunction with those of the other systems. They further asserted that the co-existence of such anomalies should be kept in mind by angiologists, radiologists, traumatologists and vascular surgeons.
Numerous muscular and vascular anomalies have been reported earlier in the form of additional heads of the biceps brachii [4,5,6], additional heads of the triceps brachii [7,8], accessory heads of origin of the FDS, FDP and the FPL [2,9], bifurcations of the lumbricals [2] and the superficial brachial artery [10,11], bifurcation of the axillary artery in its third part [12], trifurcation of the brachial artery [13], duplications of the superficial palmar arch [14] and the axillary arch muscle [15], etc. However, all of these have been encountered individually and separately. None of the studies found multiple musculovascular anomalies in the same limb. A bilateral representation of most of these is even rarer. A superficial brachial artery which was found bilaterally was however reported earlier by Sharma et al., [16] and Kaur et al. [17] But its association with the numerous muscular anomalies has never been observed.
We, in the Department of Anatomy, Govt Medical College, Amritsar, India, came across such a case where multiple musculovascular anomalies were found, some of them being bilateral. Since this was the rarest of the rare cases which had an ontogenic, phylogenic and a clinical significance, it is being reported here.
CASE REPORTRT
During the routine undergraduate dissections of the upper limbs of a 50 years old female cadaver in the Department of Anatomy, Govt Medical College, Amritsar, India, the following variations were seen on the left side:
An accessory head of origin of the biceps brachii was arising from the upper half of the anteromedial surface of the humerus and the adjoining anterior surface of the medial intermuscular septum. It mingled with the other two heads of the biceps in its distal part, for a common insertion. The nerve supply to this accessory head came from the musculocutaneous nerve, as a separate branch.
A superficial brachial artery crossed the median nerve from the medial to the lateral side superficially and divided into its terminal branches, as is usual [Table/Fig-1].
Showing the Third Head Of Biceps Brachii and Superficial Brachial Artery In Right Left Upper Limb
(CB: Coracobrachialis; LH: Long head of Biceps Brachii; SH: Short head of Biceps Brachii; TH: Third head of Biceps Brachii; MCN: Musculocutaneous nerve; MN: Median nerve; SBA: Superficial brachial artery)

An accessory muscular slip was arising from the common flexor origin of the forearm and the Flexor Digitorum Superficialis (FDS) and it was going distally. Its tendon was joining on the radial side of the Flexor Digitorum Profundus (FDP) tendon.
Another accessory muscular slip with the same origin, but of a somewhat smaller size, was ending in a tendon, which joined the ulnar side of the tendon of the Flexor Pollicis Longus (FPL) [Table/Fig-2].
Showing accessory muscular slips of origin for FDP and FPL and bifurcation of tendons of Brachioradialis.
(FDS- Flexor digitorum superficialis; FDP- Flexor digitorum profundus; FPL- Flexor pollicis longus; AMI: accessory muscular slip for FDP; AMII: accessory muscular slip for FPL; BR: Brachioradialis; T1,T2: Two tendons of insertion of BR; MN: Median nerve; RA: Radial artery; UA: Ulnar artery)
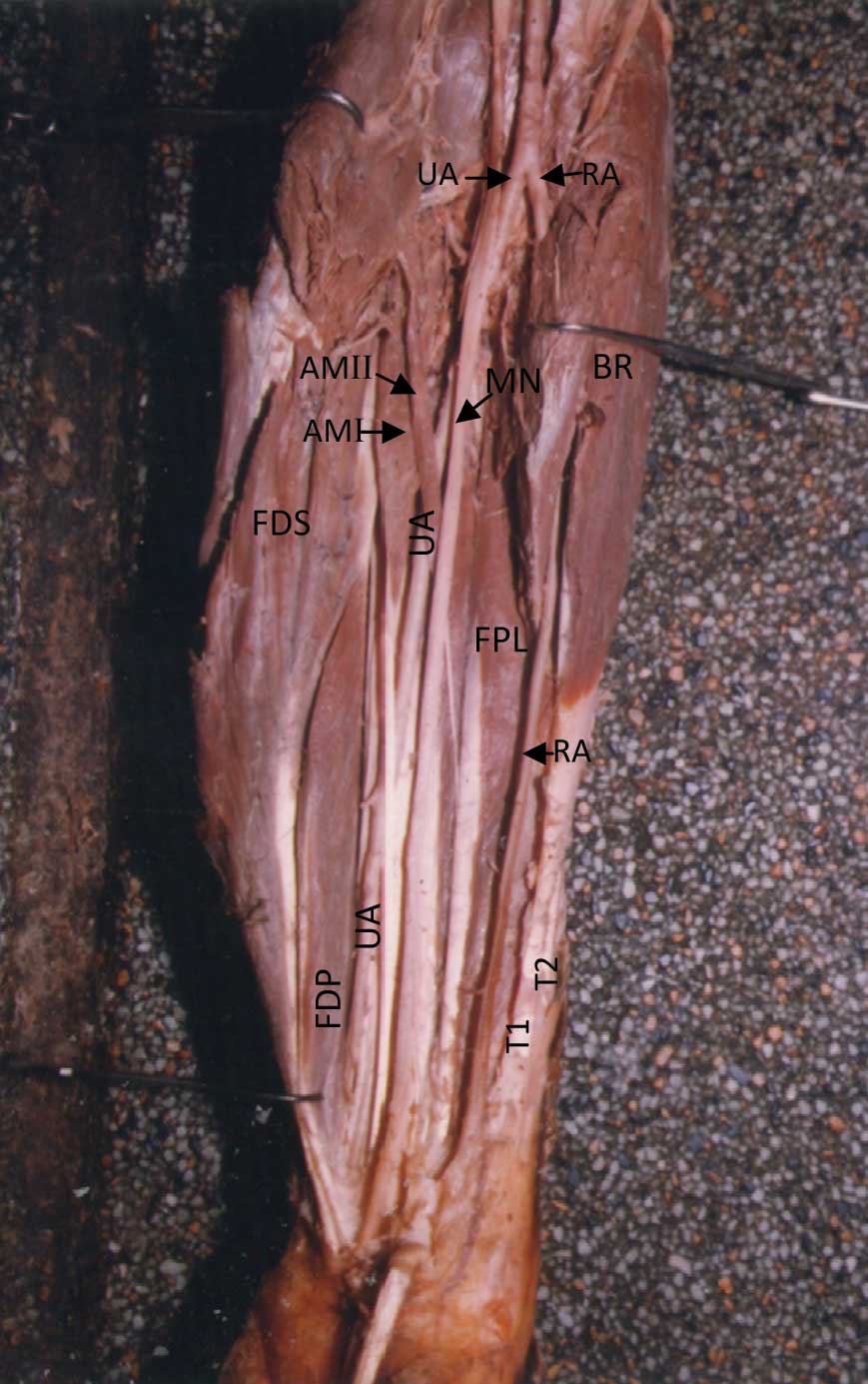
Bifurcation of the tendon of the brachioradialis, with one tendon getting inserted into the distal one third of the lateral border of the radius and the other getting inserted into its styloid process.
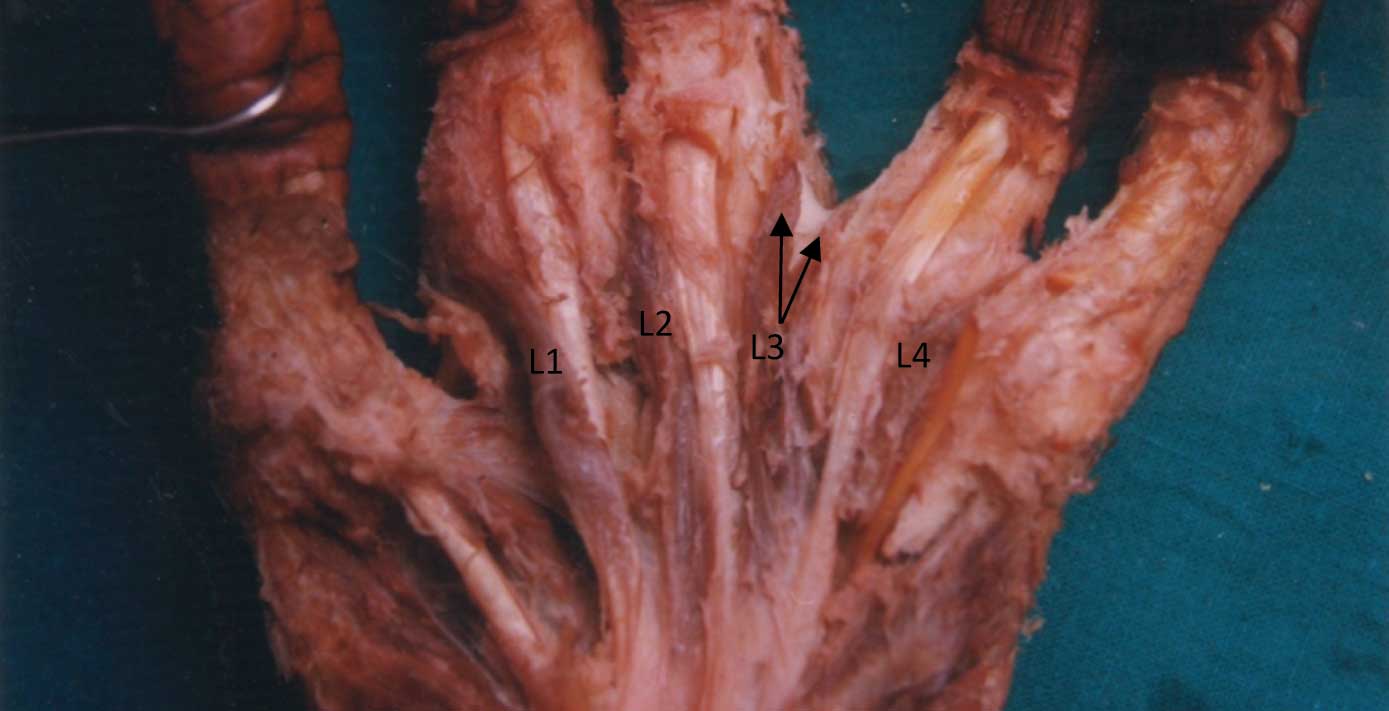
The third lumbrical was bifurcating almost in the middle, with two bellies going to the adjacent sides of the third and fourth fingers for getting inserted into the ulnar side of the third and the radial side of the fourth dorsal digital expansion [Table/Fig-3].
Showing Bifurcation of Third Lumbrical
(L1- L4: Lumbricals)
The right limb of the same body showed:
The accessory head of the biceps brachii as on the left side.
An accessory muscular slip from the common flexor origin to the flexor digitorum profundus.
A bifid insertion of the third lumbrical as well as the fourth lumbrical.
DISCUSSION
The three headed biceps brachii: This muscle usually arises by two heads i.e. the short and long heads. Cheema and Singla [6] threw a flood of light on the incidence of its supernumerary third head, which occurs in a frequency which ranges from 0.18% [18] to 21.5% [19] in different populations. They found it in 2.3% of their 126 dissections in north Indians, but none of them was bilateral.
Phylogeny: According to Hooton [20], two or three extra heads are found normally in gibbons. This is because of the brachiating nature of the former, where these extra heads are used for lifting whole body weight, by flexing the arm. During the phylogeny from the brachiating gibbons to the terrestrial and the bipedal man, the need for the the third head decreased and ultimately it disappeared. Its occasional persistence unilaterally or bilaterally supports the view of gibbons being one of the ancestors of man. It is also explained as a remnant of a “tuberculoseptate” head which is seen in hyalobates, but is a product of regression in humans and anthropoids [21]. Thus, this anomaly is an atavistic condition.
Functional and clinical implications: From a functional view point, the humeral origin of the third head of the biceps brachii would enhance the strength of flexion of the elbow joint, irrespective of the position of the shoulder joint, because it crosses only the elbow joint. A dual origin of the third head in which the medial fibres originate from the short head of the biceps and the lateral fibres originate from the insertional area of the deltoid muscle, may contribute to the supination of the forearm, as the muscle origin is in a lateral position which is relative to the rotational axis of the arm [22]. However, a medial brachial origin, as was found in the present case, may contribute to the pronation of the forearm, irrespective of the shoulder joint position.
Clinically, the third head may lead to an unusual bone displacement which is subsequent to a fracture [22]. Furthermore, if it is unilateral, it may be the cause of an asymmetry between the 2 arms and hence, the cause of a confusion with pathological conditions like tumours [6].
Accessory slips for FDP and FPL: The FDP usually arises from the upper three quarters of the anterior and the medial surfaces of the ulna from a depression on the medial side of the coronoid process, from the upper three quarters of the posterior ulnar border by an aponeurosis and the anterior surface of the ulnar half of the introsseus membrane. The FPL arises from the grooved anterior surface of the radius, extending from below its tuberosity to the upper attachment of the pronator quadrates and from the adjacent introsseus membrane [1]. It was Gantzer (1813) who first described the two accessory muscles in the human forearm, which insert either into the FPL or the FDP. Later on, these were reported by many authors and were named after the pioneer, as Gantzer’s muscle [23–25]. The incidence of the accessory head of the FPL has been reported to range from 39.2% [26] to 73.7% [23] and that of the accessory head of the FDP has been reported to range from 2.9% [23] to 35.2% [24]. These accessory muscles have been observed to arise from the coronoid process or from the medial epicondyle via the fibres of the flexor digitorum superficialis, or from a combination of these two [23,24,26]. As far as a bilateral presentation is concerned, it is usually said that there are more chances for an accessory head to be bilateral than to be unilateral [23,27]. In the present case, an accessory slip was seen to bilaterally arise from the common flexor origin and the FDS and it joined the radial side of the FDP tendon. Another accessory muscular slip was seen only on the left side to arise from same origin and to insert into the ulnar side of the FPL tendon. Thus, the accessory slip for FDP was bilateral and that for FPL was unilateral.
Ontogeny: Dylevsky [28] considered the deep and the superficial flexor tendons to be derived from separate strata and not from a single blastema. However, Chaplin and Greenlee [29], after studying the development of the digital tendons in human embryos and foetuses, confirmed the initial single blastemal arrangement of all the digital flexor tendons. According to William et al., [1] the skeletal muscles originate from a pool of premyoblastic cells which arise in the dermamyotomes of the maturing somite. These myotomic precursor cells ultimately differentiate to form the axial (or the epaxial) musculature (the erector spinae). A distinct cohort of the precursor cells migrate away from the somite to invade the lateral region of the embryo to form the muscles of the limbs and the body wall (hypaxial musculature). Virtually, all the cells in the lateral half of the newly formed somite are destined to migrate in this way. They further emphasized that the myoblastic cells from which the limb muscles develop, do not arise in situ from the local limb bud mesenchyme, as was once thought, but that they migrate from the lateral half of the somite.
During myogenesis in the limb buds, the mononucleate myoblasts aggregate and fuse to form multinucleate cylindrical syncytia or myotubes. These primary myotubes attach at each end to the tendons and the developing skeleton in the early stages of their development. Similarly, secondary and tertiary myotubes are formed and this leads to an increase in the bulk of the muscle. In the present case, it was assumed that some of these myotubes, instead of joining the tendon of the FDS, joined the tendons of the FPL and the FDP, while their proximal attachment was still on the common flexor origin. These myotubes formed accessory slips while they were going to the FPL and the FDP. Their bilateral presentation indicates that the factors which were responsible for this variation could have been operating during their ontogenesis.
Phylogeny: In the lower vertebrates, the forearm musculature consists of a common mass and it is inserted into the palmar aponeurosis from which the short flexors arise. In mammals, these digital muscles degenerate into tendinous bands with which the tendons of the antebrachial part become continuous. In monotremes, the flexor digitorum sublimus et profundus and the flexor pollicis longus form a common mass from which the digital tendons arise. In marsupials, the antebrachial muscle mass gets differentiated into 5 parts, namely the condylo-ulnaris, the condylo-radialis, the radialis, the centralis and the ulnaris [9].
As the evolutionary scale ascends, part of and later, the whole of the condylo-ulnaris separates from the common mass and it joins the digital tendons. At a later stage, the condylo-radialis and the centralis follow suit and all the three join together, resulting in the formation of the flexor digitorum sublimus. The ulnaris and the radialis remain united and after their complete separation from the superficial mass, they form a flexor digitorum profundus like muscle [9].
In man and primates, the radialis part separates and it forms the flexor pollicis longus and the ulnaris persists as the flexor digitorum profundus.
Thus, the accessory slips of origin of the FDP and the FPL may be considered as a connection between the superficial and the deep flexors of the forearm and they may be regarded as a phylogenetic relic of the evolution of the incomplete separation of the flexor muscle mass.
Functional and clinical implications: From a functional point of view, the FPL stabilizes the flexed phalanx of the thumb in precision handling (finger thumb prehension) and a powerful grip (full thumb prehension) [30]. Furthermore, it is the architecture of the whole muscle which is important in determining its function. The structural variations affect not only the overall shape and size of the muscle, but also the function of the skeletal muscle, especially the range of motion. The additional head of the FPL is made up of fusiform muscle fibres which are in opposition to the unipennate muscle fibres of the FPL. Since the functions of the fusiform and the unipennate are different, these could lead to an extra strain on the normal functional movements of the FPL, which could in turn lead to a loss of the precise and skilful movements [30,31].
From the clinical point of view, the accessory head of the FPL has been implicated in the anterior interosseus syndrome [27], while that of the FDP may be associated with its restricted movements, which can result in burning pain in the lower third of the forearm via a muscle tendon shearing action [32]. Hammady et al., [33] advices to keep the possibility of the Gantzer’s muscle in mind during the anterior approaches to the proximal radius and the elbow joint and during a decompression fasciotomy for the compartment syndrome of the forearm. It is also important to rule out such accessory muscles while neuropathies of different types like the carpel tunnel, the Guyon’s tunnel, the cubital tunnel, etc are being diagnosed [31].
Bifurcation of the tendon of the brachioradialis: Usually, the brachioradialis inserts as a single tendon on the lateral side of the distal end of the radius, just proximal to its styloid process [1]. According to Tountas and Bergman [34], in about 7% of the individuals, the tendon of the brachioradialis splits into two or three slips that are inserted into styloid process of the radius or into the lateral aspect of the lower end of the radius. In the present case, in the left upper limb, the two slips of the brachioradialis got inserted into the lower one-third of the lateral aspect of the radius and its styloid process.
Clinical implication: Occasionally, the superficial branch of the radial nerve may pass through these slips and thus, is in danger of getting compressed in between the same.
Bifid or split insertion of the third and fourth lumbricals: Normally, each lumbrical passes to the radial side of the corresponding finger and is attached to the lateral margin of the dorsal digital expansion of the extensor digitorum [1]. In the present case, the third lumbrical on the left side and the third and the fourth lumbricals on the right side, split to get inserted on the extensor expansion of the adjacent fingers. The third lumbrical has been called as the ‘most variable lumbrical’ by Mehta and Gardner [35], which showed a split or a misplaced insertion. [Table/Fig-4] compares the incidence of the split insertion of the third and fourth lumbricals, as has been reported by earlier authors.
Showing the incidence of split insertion of third and fourth lumbricals
| Sr. No. | Authors (Year) | Incidence of split insertion of |
|---|
| Third Lumbrical (%) | Fourth Lumbrical (%) |
|---|
| 1. | Eyler & Markee (1954) [36] | 15.6 | 6.06 |
| 2. | Mehta and Gardner (1961) [35] | 38.7 | 8 |
| 3. | Singh et al. (1975) [37] | 27.1 | 25.2 |
As is evident from [Table/Fig-4], the third lumbrical showed a split insertion in the frequency range of 15.6% [36] to 38.7% [35], while in case of the fourth lumbrical, its incidence was 6.06% [36] to 25.2% [37]. Singh et al [37] attributed such a high incidence of the split insertion in the third and fourth lumbricals to their bipennate origins.
Phylogeny: Mc Murrich [38] compared the split insertion of the third and fourth lumbricals morphologically to the doubling of the muscles in some lower mammals like Verginian opposum. Thus, this condition may also be an atavistic condition.
The superficial brachial artery: Usually, the brachial artery passes deep to the median nerve from the medial to the lateral side in front of the arm. But when it crosses the median nerve superficially, it is termed as the superficial brachial artery [16].Patnaik et al., [10] threw a flood of light on the earlier literature which was related to this entity. It was found in the frequency range of 0.2% to 25% [16,17].
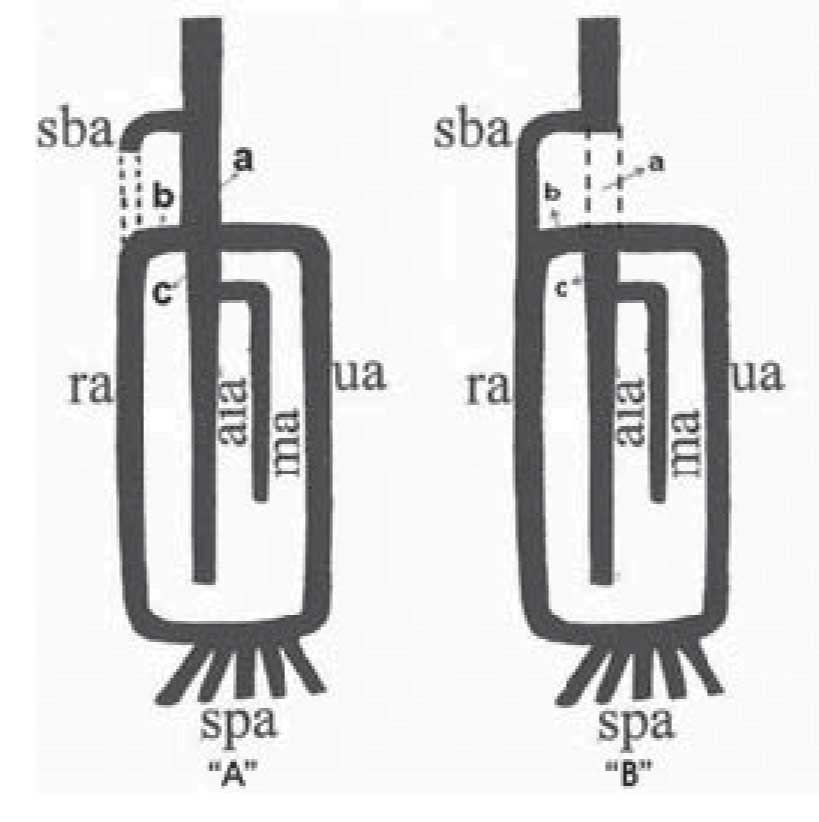
Ontogeny: It can be easily interpreted if one goes through the Singer [39] staging of the development of the brachial artery. In the present case, it seemed that in Singer [39] stage 3, the brachial artery which was between the origin of the ulnar artery and the superficial brachial artery (a in [Table/Fig-5]) had retrogressed and had severed its communication with the common interosseus artery. The superficial brachial artery had failed to retrogress and it had continued to supply the radial artery. The anastomosis between the superficial brachial artery and the brachial artery (b in [Table/Fig-5]) which usually forms the proximal part of the radial artery, now formed the proximal part of the ulnar artery, thus giving an appearance that the radial and the ulnar arteries were terminal branches of the superficial brachial artery and that the common interosseus artery was coming as a branch of the ulnar artery.
(A) Normal Development of Human Brachial artery. (Singer, 1933); (B) Development as in the present case.
(sba: Superficial brachial artery, ra: Radial artery, ua: Ulnar artery, ma: Median Artery, aia: Anterior Interosseous Artery, spa: Superficial Palmer Arch)
Phylogeny: The superficial brachial artery is found normally in primates [40] and so it was also reasoned out to be an atavistic condition.
Clinical implication: Kaur et al., [17] emphasized that the superficial brachial artery, because of its position, not only is more vulnerable to trauma, but is also made accessible to cannulation, if it is needed. Intravenous drugs, if they are accidently injected into a superficial brachial artery, may lead to gangrene or loss of the hand.
[1]. Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Muscle, Salmon S edr. In:Gray’s Anatomy 1995 38thNew YorkChurchill Livingstone:842-44. [Google Scholar]
[2]. Hollinshead WH, General survey of the upper limb and the arm. In:Functional Anatomy of the Limbs and the Back 1951 65PhiladelphiaW.B. Saunders and Co.:105-16. [Google Scholar]
[3]. Jones EG, Some unusual muscular anomalies explained embryologicallyActa Anat. 1966 64:517-30. [Google Scholar]
[4]. Sarikcioglu L, Yildrim FB, High origin of the radial artery accompanied by muscular and neural anomaliesAnn Anat. 2003 185:179-82. [Google Scholar]
[5]. Higashi N, Sone C, A study on accessory head of biceps brachii in manActa Anat Nippon. 1988 63:78-88. [Google Scholar]
[6]. Cheema P, Singla RK, Low incidence of third head of biceps brachii in the North Indian populationJ Clin Diag Res. 2011 5(7):1323-26.(Supp 2) [Google Scholar]
[7]. Fabrizio PA, Clemente FR, Variation in the triceps brachii muscle: a fourth muscular headClin Anat. 1997 10:259-63. [Google Scholar]
[8]. Cheema P, Singla RK, Four headed triceps brachii muscle- A case reportInt J Anat Variation 2011 4:43-44. [Google Scholar]
[9]. Bhargva I, An extra muscle in forearmJ Anat Soc Ind. 1956 5(2):81-82. [Google Scholar]
[10]. Patnaik VVG, Kalsey G, Singla RK, Branching pattern of brachial artery- A morphological studyJ Anat Soc Ind. 2002 51(2):176-86. [Google Scholar]
[11]. Singla RK, Lalit M, Superficial brachial artery with high origin of profunda brachii and common introsseus artery- A case reportJ Clin Diag Res. 2011 5(3):628-30. [Google Scholar]
[12]. Patnaik VVG, Kalsey G, Singla RK, Bifurcation of axillary artery in its third part-A case reportJ Anat Soc Ind. 2001 50(2):166-69. [Google Scholar]
[13]. Patnaik VVG, Kalsey G, Singla RK, Trifurcation of brachial artery- A case reportJ Anat Soc Ind. 2001 50(2):163-65. [Google Scholar]
[14]. Patnaik VVG, Kalsey G, Singla RK, Superficial palmar arch duplication-A case reportJ Anat Soc Ind. 2000 49(1):63-66. [Google Scholar]
[15]. Sharma T, Singla RK, Agnihotri G, Gupta R, Axillary arch muscle- A case reportKathmandu Uni Med J. 2009 7(4):432-34. [Google Scholar]
[16]. Sharma T, Singla RK, Sachdeva K, Bilateral superficial brachial artery-A case reportKathmandu Uni Med J. 2009 7(4):426-28. [Google Scholar]
[17]. Kaur N, Patnaik VVG, Singla RK, Bilateral superficial brachial artery- A case reportInt J Anat Variation 2011 (4):207-10. [Google Scholar]
[18]. Khaledpour VC, Uber Anomalies des M biceps brachiiAnat Anz. 1985 159:79-85. [Google Scholar]
[19]. Greig HW, Anson BJ, Budinger JM, Variations in the form and attachments of the biceps brachii muscleQurt. Bull Northwest Univ Med School 1952 26:241-44. [Google Scholar]
[20]. Hootan EA, Man’s relations and the individual life cycle. In:Up From the Ape 1959 252ndNewYorkMc Millan Co.:226 [Google Scholar]
[21]. de Burlet HM, Correlge J, Uber variation des menschlichen musculus biceps brachiiGeganbaur’s morphol Jahrb 1919 50:403-16. [Google Scholar]
[22]. Sweiter MR, Carnichael SW, Bilateral three headed biceps brachii musclesAnat Anz. 1980 148:346-49. [Google Scholar]
[23]. Mangini U, Flexor pollicis longus muscle- its morphology and clinical significanceJ Bone Joint Surg 1960 42A:467-70. [Google Scholar]
[24]. Kida M, The morphology of Gantzer’s muscle with specific reference to morphogenesis of the flexor digitorum superficialisKaibogaku-Zasshi 1988 63:539-46. [Google Scholar]
[25]. Jones M, Abrahams PH, Sanudo JR, Accessory head of deep forearm flexors- Case ReportJ Anat 1997 191:313-14. [Google Scholar]
[26]. Wood J, Variations in human mycologyProceedings of the Royal Society of London 1868 16:483-525. [Google Scholar]
[27]. Dellon AL, Mackinson SE, Musculoaponeurotic variations along the course of median nerve in the proximal forearmJ Hand Surg. 1987 12 B:359-63. [Google Scholar]
[28]. Dylevsky I, Tendons of the muscle flexor digitorum superficialis et profundus in the ontogenesis of human handFolia Mophol. 1968 16:124-30. [Google Scholar]
[29]. Chaplin DM, Greenlee TK, The development of human digital tendonsJ Anat. 1975 120:253-74. [Google Scholar]
[30]. Levangic PK, Norkin CC, Joint structure and function: A comprehensive analysis 2006 4thPhiladelphiaFA Davis Co.:120-21. [Google Scholar]
[31]. Mani SS, Vishnumaya G, Madhan SJK, Accessory head of Flexor Pollocis Longus and its significance in anterior introsseous nerve neuropathies and precision handlingInt J Anat Variation 2010 3:46-48. [Google Scholar]
[32]. Ryu J, Watson HK, SMB Syndrome (Symptomatic Supernumerary Muscle Belly Syndrome)Clin Orthop and Rel Res 1987 216:195-202. [Google Scholar]
[33]. Hemmady MV, Subramanya AV, Mehta IM, Occasional head of Flexor Pollocis Longus muscle: A study of its morphology and clinical significanceJ Postgrad Med 1993 39:14-18. [Google Scholar]
[34]. Tountas CP, Bergman RA, Anatomic variations of the upper extremity 1993 NewYorkChurchill livingstone:109-35. [Google Scholar]
[35]. Mehta HJ, Gardner WU, A study of lumbrical muscles in the human handAm J Anat. 1961 :227-38. [Google Scholar]
[36]. Eyler DL, Marker JE, The anatomy and function of the intrinsic musculature of the fingersBone Joint Surg 1954 36A(1):1-9. [Google Scholar]
[37]. Singh JD, Raju PB, Singh S, Anomalous insertion of hand lumbricalsJ Anat Soc Ind. 1975 24(3):122-25. [Google Scholar]
[38]. Mc Murrich JP, Phylogeny of palmar musculatureAm J Anat. 1903 2:463-500. [Google Scholar]
[39]. Singer E, Embryological patterns persisting in the arteries of the armAnat Record 1933 55:406-13. [Google Scholar]
[40]. Miller RA, Observations upon the arrangements of axillary artery and brachial plexusAm J Anat. 1939 64:143-63. [Google Scholar]