Peripheral insensate neuropathy is defined as the presence of one or more insensate areas [1]. It is a common problem which is encountered in middle and old aged people. It is one of the disabling complications of diabetes because of its high incidence and its potential to lead to lower extremity ulceration, deformation and amputation [2]. Many factors have been associated with neuropathy, like age, sex, race, glycaemic control, nutrition, toxin exposure, drugs, alcohol, etc [1,3,4].
Peripheral neuropathy affects 2- 8% of the adults and it increases with age. With an early detection and history taking and focused laboratory tests, the underlying cause can be identified in ~75% of the cases. The prevalence of neuropathy is 66% for type 1 diabetes and it is 59% for type 2 diabetes. In a population cohort of diabetic patients, two third of the diabetics had an objective evidence of neuropathy, mainly a loss of the foot sensation, but only 15% of the IDDM cases and 13% of the NIDDM cases were symptomatic. Peripheral neuropathy can occur before the onset of clinically detectable Diabetes mellitus (DM) [5].
Height is an important and a practical predictor of peripheral insensate neuropathy. As the height increases, the lengths of the nerve fibers also increase and so the surface area of the axons is available for the toxin exposure and the physical damage is more. So, the risk of peripheral insensate neuropathy increases with an increase in height. Many studies have shown the corelation of height with peripheral neuropathy and amputation among diabetics [3,6]. It is still unknown whether there is any threshold in association between height and the risk for peripheral insensate neuropathy in the general population.
An early screening of peripheral insensate neuropathy by the health care personal, a tight glycaemic control among diabetics, a cessation of alcohol intake and smoking, correction of nutritional deficiencies, avoiding toxins and drugs and other preventive care are considered as the key public health strategies which can be used against costly foot complications [7,8].
A simple instrument, a Semmes-Weinstein monofilament of 5.07/10 gm has been recommended by the International Diabetes Federation, the American Diabetes Association and the World Health Organization as a device that can be used by health care professionals at every level of care [8]. Previous studies have shown that the presence of one or more insensate areas is highly predictive of ulcers and that it has moderately high sensitivity (~85%) and specificity (~80%) based on the vibration testing and the ulcer history [9–11].
The Semmes Weinstein monofilament is portable, cost effective, easily available and it has good sensitivity.
A cross sectional study was conducted in Kasturba Medical College (Manipal University) in the years 2009-2012, which included an examination of 818 people of the ages of >30 years by random sampling, who attended the outpatients clinic, after taking informed consents from the subjects and an institutional clearance from the KMC Hospital, Manipal University.
METHODOLOGY
A detailed history was taken, with a particular emphasis on the sensory symptoms of neuropathy, drug ingestion, toxin exposure, diabetes, alcohol consumption, and education. A detailed examination was done, with emphasis on height, weight and blood pressure.
Peripheral insensate neuropathy assessment:
The Semmes Weinstein monofilament of 5.07/10 gm force was used on the patients with their eyes closed. The sensation at 3 sites on each foot was checked [Table/Fig-1] (6 sites) [1,12].
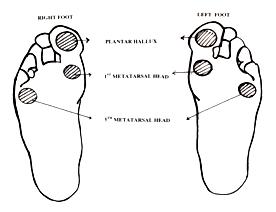
The plantar hallux.
The plantar 1st meta tarsal head.
The plantar 5th meta tarsal head.
The filament was applied at the site till it buckled and it was held for another second. The people with calluses were excluded and a clinical examination was done [Table/Fig-2]. The site was considered to be insensate if:
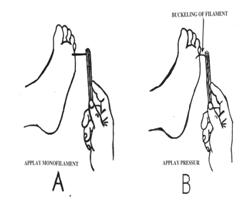
There were two incorrect responses.
Two responses could not be determined.
One response was incorrect and one response couldn’t be determined.
The sites were tested in a non sequential order. An impaired sensation was quantified on the basis of the total number of insensate areas on both the feet [Table/Fig-1 and 2].
• The parameters which were analyzed were
Hypertension [Yes (<7 years ( ), >7 years ( ) /No ( )], Diabetes [Yes <7 years ( ), >7 years ( )/ No], Alcohol consumption. [Yes ( )/ No ( )] , Smoking [Yes ( )/ No ( )], Height in cm [<150 ( ), 150-159( ), 160-169 ( ), >170( )], BMI <18.5 ( ), 18.6-24.9 ( ), 25-29.9( ),>30( )}, Hb A1C [<6 ( ), 6 -6.9 ( ), 7- 7.9 ( ), >8)
The data analysis was carried out by using the Chi square test, logistic regression analysis and the SPSS software, version 17.0 . A p value of <0.05 was considered as significant.
RESULTS
This study included the examination of 818 patients who attended the OPD, among whom the mean height was 161.3 cm and the mean weight was 62.7Kg. [Table/Fig-3] shows the characteristics of the study sample. The prevalence of peripheral insensate neuropathy was 9.1% (9.7% in males and 7.6% in females). The height which was adjusted for the gender analysis was found to be significant [Table/Fig-4].
| Variables | Numbers (%) |
|---|
| Gender | Male | 583 (71.3%) |
| Female | 235 (28.7%) |
| Age | < 40 | 184 (22.5%) |
| 41-50 | 349 (42.7%) |
| 51-60 | 182 (22.2%) |
| 61-70 | 73 (8.9%) |
| >70 | 30(3.7%) |
| DM | Present | 148 (18.1%) |
| Absent | 670 (81.9%) |
| HTN | Present | 150 (18.3%) |
| Absent | 668 (81.7%) |
| BMI | Lean | 16 (2%) |
| Normal | 469 (57.3%) |
| Overweight | 290 (35.5%) |
| Obese | 43 (5.2%) |
| Alcohol | Present | 167 (20.4) |
| Absent | 651 (79.6%) |
| Smoking | Present | 152 (18.6%) |
| Absent | 666 (81.4%) |
| Height | Median | Short | 370 (45.2%) |
| Tall | 448 (54.8%) |
| 1 SD | Short | 114 (13.9%) |
| Normal | 568 (69.4%) |
| Tall | 136 (16.6%) |
| Quartiles | 0-25% | 227 (27.8%) |
| 25-50% | 185 (22.6%) |
| 50-75% | 227 (27.8%) |
| 75-100% | 179 (21.9%) |
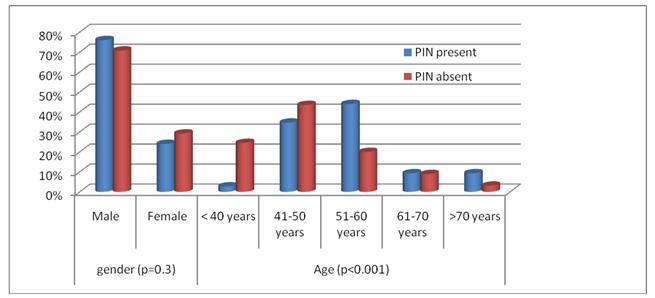
prevalence of PIN with respect to age and gender
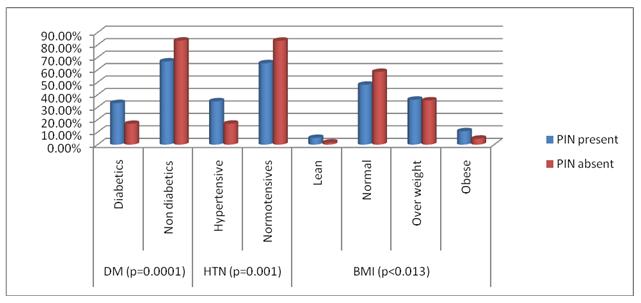
The people with hypertension were found be at a higher risk, the same as in diabetics, for peripheral insensate neuropathy. The prevalence of peripheral insensate neuropathy among the hypertensive group was 17.3% as compared to 16.9% among the diabetics, which explained the significance of hypertension.
The durations of hypertension and diabetes were also statistically significant. The prevalence of peripheral insensate neuropathy was three times more in the hypertensive group with a duration of >7years-42.1% as compared to that in the group with a duration <7years -13.5% and it was two times more among diabetics with a duration of >7years -31.8% as compared to that in diabetics with a duration of < 7years-14.3% [Table/Fig-5].
prevalence of PIN among DM, HTN and BMI
Peripheral insensate neuropathy prevalence increases as the age advances, irrespective of the gender (<40years-1.1%,>70years- 23.3%). Among the people, peripheral insensate neuropathy was found to be at a higher level between the ages of 40-60 years (78.7%). The mean height was 163.4cm among men and it was 155.6cm among women. For our analysis, to know the effect of height, irrespective of the gender and the diabetic and the hypertensive statuses and the BMI, we segregated the people into quartiles, 1SD and median height [Table/Fig-6]. The threshold of the prevalence of peripheral insensate neuropathy increases as the height increases, in the taller group and in the 4th quartile (p<0.001) [Table/Fig-7].
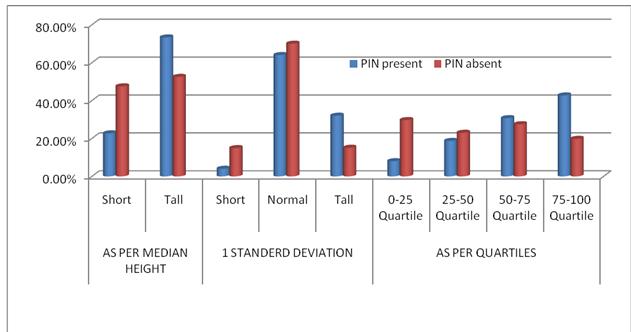
prevalence of PIN with respect to height (P<0.001)
Distribution of variables with respect to height (taking Quartile).
| Variables | 0-25% | X2 (P) | 25-50% | X2 (P) | 50-75% | X2 (P) | 75-100% | X2 (P) | Total |
|---|
| PIN | PIN | PIN | PIN |
|---|
| Yes | No | Yes | No | Yes | No | Yes | No |
|---|
| Gender | M | 4 (0.6%) | 87 (14.9%) | 1.813 (0.17) | 9 (1.54%) | 113 (19.38) | 0.019 (0.891) | 18 (3.08%) | 184 (31.5%) | 3.004 (0.08) | 26 (4.45% | 142 (24.3%) | 10.734 (0.0011) | 583 (100% |
| F | 2 (0.8%) | 134 (57.02%) | 5 (2.12%) | 58 (24.6%) | 5 (2.12%) | 20 (8.5%) | 6 (2.5%) | 5 (2.12%) | 235 (100%) |
| DM | Present | 2 (1.35%) | 44 (29.7%) | 0.651 (0.4196) | 5 (3.37%) | 24 (16.21) | 4.60 (0.032) | 4 (2.70%) | 39 (26.3%) | 0.040 (0.841) | 14 (9.45%) | 16 (10.81) | 24.206 (0.0001) | 148 (100%) |
| Absent | 4 (0.59%) | 177 (26.4%) | 9 (1.34%) | 147 (21.9%) | 19 (2.83%) | 165 (24.6%) | 18 (2.68%) | 131 (19.55) | 670 (100%) |
| HTN | Present | 3 (2%) | 43 (28.6%) | 3.373 (0.063) | 6 (4%) | 37 (24.6%) | 3.266 (0.0702) | 5 (3.3) | 32 (21.3%) | 0.55 (0.456) | 12 (8%) | 12 (8%) | 19.481 (0.0001) | 150 (100%) |
| Absent | 3 (0.4%) | 178 (26.6%) | 8 (1.19) | 134 (20.0) | 18 (2.69) | 172 (25.7) | 20 (2.99) | 135(20.2) | 668 (100%) |
| BMI | Lean | 1 (6.30%) | 4 (25%) | 7.38 (0.06) | 1 (6.3%) | 5 (31.35) | 2.11 (0.54) | 1 (6.3%) | 2 (12.5%) | 16.67 (0.0008) | 1 (6.3%) | 1 (6.3%) | 1.97 (0.57) | 16 (100%) |
| Normal | 2 (0.4%) | 106 (22.6%) | 7 (1.5%) | 84 (17.9) | 8 (1.7%) | 144 (30.7) | 19 (4.1%) | 99 (21.1) | 469 (100% |
| OW | 2 (0.7%) | 98 (33.8%) | 4 (1.4%) | 70 (24.1) | 10 (3.4%) | 51 (17.7) | 11 (3.8%) | 44 (15.8) | 290 (100%) |
| Obese | 1 (2.3%) | 13 (30.23%) | 2 (4.7%) | 12 (27.9%) | 4 (9.3%) | 7 (16.3%) | 1 (2.32% | 3 (6.97) | 43 (100%) |
As shown in [Table/Fig-7], we found a similar association between the height and the peripheral insensate neuropathy across the strata of diabetes, the hypertensive status, gender and BMI, with respect to the height, by dividing the population with respect to the quartiles. We also found similar results when we divided the population into tall and short with respect to the 1SD and the median height, irrespective of the co morbidities. Among the study population, the BMI was also one of the important risk factors, even though the prevalence was much higher among the lean and obese groups.
In the study population, the risk of peripheral insensate neuropathy was significantly higher among males >167cm and among females, it was >159cm. The adjusted peripheral insensate neuropathy prevalence rate was higher among hypertensives than in those without hypertension from the logistic regression analysis.
We found no statistically significant interaction between peripheral insensate neuropathy and smoking and the alcohol consumption status. The logistic regression analysis shows the effect of the individual variables on nullifying the effect of the variables on each other. It shows that age, diabetes, hypertension, BMI and height (quartiles) are independent variables which have significant correlations with peripheral insensate neuropathy.
DISCUSSION
In our cross-sectional study, we confirmed that peripheral insensate neuropathy was common and that it was associated with increasing age, diabetes, hypertension and BMI. We also found that being tall was a similarly important risk factor, as was found in a similar previous study [1]. As per the definition of PIN which has been described in the methods section, 9.1% of the subjects had PIN. It was less in comparison to that in other studies (16.2%) (Cheng YJ et al.,)[1], which was probably due to the differences in the race and ethnicity (Abbott CA et al.,) [13].The reason for the difference in the rates between the ethnic groups is unknown, but height may be a factor (Tseng et al., [14], Abbott CA et al.,[13], as is also BMI (Tseng et al.,) [14].
In our study, the prevalence of PIN among the diabetics was 16.8%, as compared to that in non-diabetics (7.4%) ( p<0.001). Diabetics have a 2-3 times higher prevalence than the non-diabetics. The prevalence of PIN was 21.8% in the individuals with a duration of diabetes of >7 years as compared to the prevalence of 14.28% in diabetic individuals with <7years of disease duration (p=0.042). The glycated haemoglobin levels do not have a statistically significant association with peripheral insensate neuropathy. However, the group with glyco Hb >8 % had a higher prevalence (21%) as compared to18% in the <8% group (Herman WH et al.,) [6].
The prevalence of PIN in males was 9.7% as compared to that in females was 7.6%.The height adjusted gender analysis showed a statistical significant (p=0.001) association of PIN with the male gender. There was a significant gender difference in our study as compared to that in previous studies,{( Cheng YJ et al.,) [1] ,(Tasfaye S et al.,) [15] ,(Gregg EW et al.,)[16], which showed that PIN was more in males. This was attributed to the height factor [1,17,18]. The difference between the genders can also be explained on the basis of the biomechanics of the foot (Dinh T et al.,) [19].
The prevalence of PIN increases as the age advances (p <0.001). The prevalence roughly increased by 10% from the age group of 41-50 to the age group of 51-60 yrs ( Gregg EW et al., [16] which was comparable to the findings of other studies) and it also doubled in the age group of more than 70 years. However, there was a drop in the 61- 70 years age group and the reason was not known. As compared to the findings of previous studies, in our study, the prevalence of PIN increased as the age advanced, irrespective of the diabetic status [1–9,16,20,21]. The attribution of the increase in age for PIN may be because of the decreased nerve fibres, a reduction in the nerve diameter and changes in the fibre membrane and the conduction velocity {(Huang CR et al.,) [22],(Chu NS et al.,) [23].
Hypertension was found to be significantly associated with PIN in our study (p < 0.001). The prevalence of PIN in the hypertensive group was 17.3% as compared to 7.33% in the non hypertensive group. The patients of the PIN group with hypertension of >7 years duration had a prevalence of 42%, which was almost 3 times as compared to that in the group with a duration of less than 7 years (13.5%), with a p value of 0.0019. In one of the studies (Cohen JA et al.,) [24], the duration of hypertension was positively associated with PIN. Hypertension is related to both micro and macro vascular complications. So, the control of hypertension reduces both and thus it reduces PIN [25,26].
In our study, it was seen that the prevalence of PIN was more in the lean (25%) and obese groups (18.6%) as compared to that in the normal (7.67%) and the overweight (9.3%) groups. In the extremes of BMI, like in lean persons, more height is a risk factor (Cheng YJ et al.,)1, or the malnutrition (underweight), this plays a role in the development of PIN. The extremes of BMI are prone for DM and they may also contribute to the development of PIN {(Solomon OU et al., [27], (Tomic M et al.,) [28]. The weight loss in lean and obese persons is an index of a poor glycaemic control, which may predispose to PIN [27–28]. The increase in the prevalence of PIN correlated significantly and independently with the body weight (Tomic M et al.,) [28], which may be a contributing factor in obese and lean persons.
Height is an important, independent and a practical predictor of PIN [1,3,4,29,30].
With respect to the height, the study population was divided into tall and short on the basis of the median height, 1SD and in terms of quartiles. In the median group, the prevalence of PIN was 12.94% in the taller group [>159cm] as compared to 4.59% in the shorter group, with a p value of 0.0001. With respect to 1SD, the prevalences of PIN were 17.64% in the taller group [>168cm], 8.45% in the normal group [153.6-168.5cm] and 2.63% in the shorter group [<159cm], with a doubling of the prevalences from the shorter to the taller groups. With respect to the quartiles, the prevalence of PIN was 2.64% in the first quartile, it was 7.56% in the second quartile, it was 10.13% in the third quartile and it was 17.88% in the fourth quartile. The above finding shows that the increase in height from the first to the fourth quartile was associated with an increase in PIN, which was statistically significant (p < 0.001).
By taking account of the median height as a cut off value, even 0.1cm above or below the median height would categorize the patients as tall and short respectively, which were two extremes of the height which would give false (false positives) interpretations. In our study, we had not considered 2 SD to categorize the patients as short and tall, as there were only few patients who belonged to the short and tall groups, which could give false negative results. (<10% Tall > 176 and Short <145cm), as the Indian average height in males is 164.5cm and in females, it is 152cm [population from the census of India 2001]. We considered 1 SD to divide the population into tall, normal and short. We also found that the males who were above 167cm, [Table/Fig-7] and the females who are above 159 cm [Table/Fig-7] were at a high risk for PIN. Even though the prevalence of PIN was very high among the females whose height was above 167cm (as in [Table/Fig-7], the number of females in that category was very less, which was extreme tallness for a female whose average height was 152cm.
Considering all the above findings, we would like to propose a screening for PIN in males who are > 167cm and for a females who are > 159cm.
As compared to the findings of a previous study (Cheng YJ et al.,) [1], in our study, a greater height was associated with an increase the PIN prevalence among the persons with and without diabetes (p<0.001). The prevalence of PIN in previous study was more among the persons who were taller than 175.5cm. However, in our study, there was a sharp increase in PIN in males after a height of 167cm and after a height of 159cm in females. This could probably be attributed to the demographic difference.
It seems unlikely that an increased stature has a generalized adverse effect on the peripheral nerve function, since sensorineural hearing loss, another form of peripheral deficit, by contrast, is associated with a reduced stature (Barrenas et al.,) [31]. A short stature is associated with CVS disease, hypertension, early arterial stiffening, IGT, type 2 DM, GDM and pre-eclampsia. A short stature is associated with micro vascular complications like nephropathy and retinopathy. But PIN is more common in the taller patients (Waden J et al.,) [32]. Many studies have shown that an increased height is associated with PN, PIN [1,3,29,33], LEA, foot ulcers and also diabeties [33].
The exact pathogenesis of height and PIN is not known. The proposed hypotheses are, an increase in height associated with an increased nerve length and a greater axon surface area. So, there is a greater risk of injury [1,3,4,14]. The greater the length of the nerve, more prolonged is the time for a complete recovery of the injured nerve{(Cheng YJ et al.,) [1] ,(Polydefkis M et al.,) [34]. As the height increases, the hydrostatic pressure in the lower limbs increases. Loss of the compensatory responses to the large pressure changes in the small blood vessels in elderly patients with diabetes tend to have more PIN. A greater skin thickness or other protective characteristics on the roles of tall people are linked to PIN.
Height was not associated with a painful neuropathy (symptomatic neuropathy) [1,3]. Smoking and alcohol consumption were not significantly associated with peripheral insensate neuropathy.
LIMITATIONS OF THE STUDY
This was a cross-sectional study and the sample was not representative of the entire population. The durations of diabetes and hypertension do not reflect the true duration of the disease. Since this was a cross-sectional study, we were unable to determine the association between the modifiable risk factors and the risk of PIN as a cause-effect association. This may explain why we did not find significant association between smoking and PIN. We used the monofilament testing to determine the PIN status, where electrophysiological studies would have provided a more accurate data.
CONCLUSION
Height is one of the independent risk factors for PIN. The duration of hypertension carries a higher significance as compared to the DM duration. The BMI was found to be a significant risk factor at the extreme ends (lean and obese). The height will help the health care providers in identifying the persons who require a more intensive neuropathic screening because of their higher risk for PIN.
We recommend that the persons with a height > 167cm among the males and with a height of 159cm among females be screened annually for PIN after the age of 40 years, irrespective of the risk factors.