Diabetes mellitus is a universal health problem which has a global prevalence of 1.3% [1]. More than 220 million people worldwide have diabetes [2] Globally, 3.2 million deaths are attributed to diabetes every year. At least one in 10 deaths among the adults who are between 35 and 64 years of age is attributed to diabetes [3]. The WHO has projected that the diabetes deaths would double between 2005 and 2030 [2].
Diabetes is not only a disease of the affluent countries, it is prevalent in the developing countries too [1]. The increasing prevalence of diabetes in the developing countries is closely associated with the industrialization and the socioeconomic development [4] India ,is known as the “Diabetes capital of the world”.
In India, the prevalence of diabetes in the urban areas increased tenfold from 1.2-12.1% during the years 1971- 2000 [5], while in the rural areas, it increased three times from 2.2% to 6.4% during the years, 1989–2003 [6] [Source: Noncommunicable Diseases in the South-East Asia Region- Situation and Response; WHO 2011].
One of the barriers in the way of seeking health care advice is the misconceptions about the disease, which revolve around all the aspects of diabetes, which include its prevention, control and treatment. Misconceptions are false beliefs which result from a lack of awareness. Studies have indicated that misconceptions and inadequate knowledge are the significant barriers in the way of a proper management of diabetes [9–11].
The present study was an attempt to know as to what misconceptions were prevalent among the urban population of Pondicherry and their associations with the socio-demographic factors.
MATERIALS AND METHODS
The study design: A cross sectional study.
The study area: Urban Health Centre (UHC) Ariankuppam, a field practice area of the Department of Community Medicine, Mahatma Gandhi Medical College and Research Institute, Pondicherry, which caters to a population of 4974.
The sample size and the selection criteria: The study was conducted during July to August 2011. A sample size of 384 was calculated, considering a 50% prevalence of the awareness with a 10% relative precision and a 95% confidence level. A total of 406 adult patients (irrespective of the presenting complaints) who visited UHC were interviewed. The purpose of the study was informed to the participants and their consent was obtained prior to the start of the study.
The data collection procedure: A pretested, semi-structured interview schedule was developed in the local language (Tamil), and it was utilized to collect the data. Trained interviewers visited the UHC to collect the data. The interview schedule contained the questions which were related to the socio-demographic profile and to the misconceptions about the management of Diabetes mellitus.
STATISTICAL ANALYSIS
The collected interview schedules were scrutinized for the accuracy of the information which was provided and for any lacunae. For study purposes, we stratified the study subjects, based on their education, occupation, etc. The compilation and analysis of the data was carried out with the help of the Epi-Info software.
The T test and the Chi-square test were used according to the distribution of the data to check the association of the different factors. A P value less than 0.05 was considered to be statistically significant.
RESULTS
In present study, a total of 406 adult patients were interviewed. The study group comprised of 243 (59.8%) females and 163(40.2%) males. Their mean age was 44.2 years (SD±17.2). A majority (24.4%) of participants were of the older age groups.
There were two most common misconceptions: “Diabetes can be cured by herbal treatment” and “Bitter foods reduce the elevated blood sugar levels” [Table/Fig-1].
Details of groups at trial entry
| Misconception | No. of participants (n 406) |
|---|
| Diabetes can be cured by herbal treatment | 189 (46.6) |
| Bitter foods reduce elevated blood sugar level | 189 (46.6) |
| Prolonged use of oral hypoglycaemic drugs and insulin can lead to serious side effects | 148 (36.5) |
| Lifestyle measures have no role in diabetes management | 144 (35.5) |
| Insulin can cure diabetes | 136 (33.5) |
| If you are taking medications you can eat anything you want | 126 (31.0) |
| Treatment should be stopped if Diabetes is controlled for few months | 111 (27.3) |
| Soaking feet in water reduces elevated blood sugar level | 110 (27.1) |
| All carbohydrates should be removed from the diet of a diabetic patient | 106 (26.1) |
| Artificial sweeteners are carcinogenic in humans | 87 (21.4) |
| Diet has no role in diabetes treatment | 86 (21.2) |
When the misconceptions were distributed according to the ages of the patients, the misconception, “The treatment should be stopped if the diabetes is controlled for a few months” significantly decreased with advancing age [Table/Fig-2].
Parameters assessed in episiotomy suturing
| Misconception | 18-27 (n-82) | 28-37 (n-77) | 38-47 (n-83) | 48-57 (n-65) | >57 (n-99) | p value |
|---|
| Diabetes can be cured by herbal treatment (n 189) | 43 (52.4) | 41(53.2) | 35(42.2) | 29(44.6) | 41(41.4) | 0.37 |
| Lifestyle measures have no role in diabetes management (n 144) | 24(29.3) | 26(33.8) | 33(39.8) | 23(35.4) | 38(38.4) | 0.65 |
| Soaking feet in water reduces elevated blood sugar level (n 110) | 30(36.6) | 25(32.5) | 20(24.1) | 15(23.1) | 20(20.2) | 0.09 |
| Bitter foods reduce elevated blood sugar level (n 189) | 32(39.0) | 37(48.1) | 44(53.0) | 35(53.8) | 41(41.4) | 0.22 |
| If you are taking medications you can eat anything you want (n 126) | 26(31.7) | 25(32.5) | 23(27.7) | 20(30.8) | 32(32.3) | 0.97 |
| All carbohydrates should be removed from the diet of a diabetic patient (n 106) | 17(20.7) | 19(24.7) | 26(31.3) | 20(30.8) | 24(24.2) | 0.49 |
| Diet has no role in diabetes treatment (n 86) | 21(25.6) | 17(22.1) | 16(19.3) | 11(16.9) | 21(21.2) | 0.76 |
| Artificial sweeteners are carcinogenic in humans (n 87) | 11(13.4) | 19(24.7) | 24(28.9) | 11(16.9) | 22(22.2) | 0.13 |
| Insulin can cure diabetes (n 136) | 30(36.6) | 19(24.7) | 36(43.4) | 18(27.7) | 33(33.3) | 0.10 |
| Prolonged use of oral hypoglycaemic drugs and insulin can lead to serious side effects (n 148) | 30(36.6) | 32(41.6) | 36(43.4) | 20(30.8) | 30(30.3) | 0.25 |
| Treatment should be stopped if Diabetes is controlled for few months (n 111) | 32(39.0) | 28(36.4) | 22(26.5) | 14(21.5) | 15(15.2) | 0.01** |
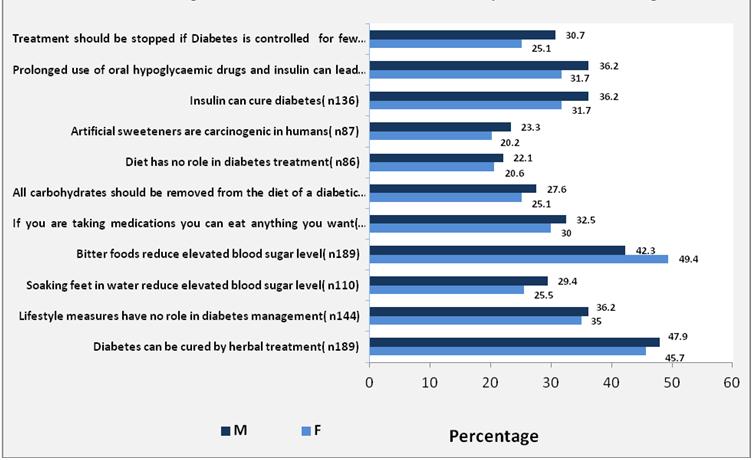
Though more males had misconceptions than females, there were no significant differences between two. The commonest misconception among females was “Bitter foods reduce the elevated blood sugar levels” (49.4%) and among males, it was, “Diabetes can be cured by herbal treatment” (47.9%) [Table/Fig-3].
Gender wise distribution of misconceptions Diabetes Management
In our study, 27.3% of the participants were illiterate, followed by 26.6 % who had education up to the middle school. The different levels of education among the participants showed a significant difference with regards to the misconception, “Artificial sweeteners are carcinogenic in humans” [Table/Fig-4].
Educational status wise distribution of misconceptions regarding Diabetes management
| Misconception | Illiterate (n-111) | Primary (n-81) | Middle (n-108) | High school & high sec. (n-89) | College & above (n-17) | P-value |
|---|
| Diabetes can be cured by herbal treatment (n 189) | 59(53.2) | 38(46.9) | 46(42.6) | 38(42.7) | 8(47.1) | 0.53 |
| Lifestyle measures have no role in diabetes management (n 144) | 42(37.8) | 29(35.8) | 35(32.4) | 32(36.0) | 6(35.3) | 0.53 |
| Soaking feet in water reduce elevated blood sugar level (n 110) | 30(27.0) | 22(27.2) | 27(25.0) | 28(31.5) | 3(17.6) | 0.76 |
| Bitter foods reduce elevated blood sugar level (n 189) | 58(52.3) | 37(45.7) | 47(43.5) | 39(43.8) | 8(47.1) | 0.71 |
| If you are taking medications you can eat anything you want (n 126) | 34(30.6) | 27(33.3) | 28(25.9) | 30(33.7) | 7(41.2) | 0.62 |
| All carbohydrates should be removed from the diet of a diabetic patient (n 106) | 22(19.8) | 26(32.1) | 32(29.6) | 24(27.0) | 2(11.8) | 0.18 |
| Diet has no role in diabetes treatment (n 86) | 26(23.4) | 17(21.0) | 21(19.4) | 17(19.1) | 5(29.4) | 0.84 |
| Artificial sweeteners are carcinogenic in humans (n 87) | 16(14.4) | 13(16.0) | 24(22.2) | 31(34.8) | 3(17.6) | 0.01** |
| Insulin can cure diabetes (n 136) | 30(27.0) | 28(34.6) | 36(33.3) | 36(40.4) | 6(35.3) | 0.39 |
| Prolonged use of oral hypoglycaemic drugs and insulin can lead to serious side effects (n 148) | 39(35.1) | 32(39.5) | 41(38.0) | 31(34.8) | 5(29.4) | 0.91 |
| Treatment should be stopped if Diabetes is controlled for few months (n 111) | 24(21.6) | 19(23.5) | 35(32.4) | 32(36.0) | 1(5.9) | 0.02** |
Regarding the occupation, most of the participants (56.2%) were unemployed, followed by unskilled workers. There was no significant difference with regards to the various misconceptions between the occupational categories.
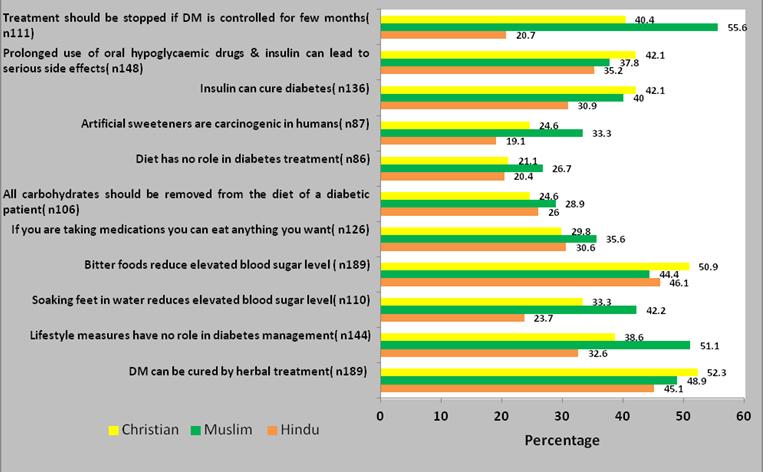
Out of the 406 participants, 304 (74.9%) were Hindus, followed by 57 (14.04%) Christians and 45 (11.08%) muslims. When the misconceptions were compared,there were significant differences between the subjects who belonged to different religions (“The treatment should be stopped if the diabetes is controlled for a few months”, “The lifestyle measures have no role in the diabetes management” and “Bitter foods reduce the elevated blood sugar levels) [Table/Fig-5].
Religion wise comparison of misconceptions of Diabetes management
DISCUSSION
Diabetes was first identified as a public health problem in the 1970s. It is an important public health problem due to the long course of the illness, its increasing prevalence in all the social strata and as it is an economic burden on the family as well as the community. Diabetes has been declared as a modern epidemic. It’s preventable and manageable nature again adds to the importance of the disease from a public health view.
It is also known as a “silent killer”, as most often, the symptoms of diabetes are absent, till the patients present with complications. Asians develop diabetes at comparatively younger ages, thus providing sufficient time for the development of the complications like neuropathy, nephropathy, retinopathy and peripheral vascular atherosclerosis, ultimately resulting in higher morbidities and mortalities [12,13].
Knowledge is the greatest weapon to fight against diabetes. The information which is related to the management can help people in assessing their risk of developing the complications and it can motivate them to seek proper treatment and care [14].
The awareness regarding self care like foot care, taking the right dose of medication at the right time, taking meals at regular intervals, regular monitoring of the blood glucose, diet control and exercise are important. Due to a lack of awareness,complications may develop and they can make the condition worse.
Health beliefs are often shaped in the minds of people on the basis of folklore and hearsay [15]. The results of our study suggested that people were having various misconceptions because of their lack of knowledge.
It is necessary for the health service providers to know what people think about a disease and its prevention and management, as misconceptions act as a barrier for the management and prevention of a disease. Diabetes, being asymptomatic most of the times, does not interfere with the daily routine and the patients ignore the condition until they develop some complications [16].
The use of traditional indigenous remedies is very much prevalent in many cultures [17]. In the Indian subcontinent, traditional medicines play an important role in the diabetes care, and a number of plants, herbs and vegetables are used therapeutically [18]. Opting for different treatment therapies at the same time or just discontinuing the allopathic treatment after a short time period of the treatment is common. In our study, we found that the prevailing conception, ‘a herbal treatment can cure diabetes’, was prevalent among 45% of the total participants, while in a study which was done by Rai M and Kishore J [19], it was seen in 17.6% of the participants. This difference may be due to the different settings of these 2 studies.
Overall, there was a strong false dietary belief that ‘Bitter foods reduce the elevated blood sugar levels’. Similar results were found in a study which was done by Rafique et al., [20] too. As “sweet” and “bitter” are opposite to each other, people have a conception that the effect of increased sugar can be reduced by bitter food items.
The participants also believed that ‘diabetes can be managed by soaking the feet in water, which reduces the elevated blood sugar levels’ and this could be because of the total ignorance of the population to the nature and the cause of the disease.
Gender was not a significant factor which was associated with most of the myths. In a study which was done by Nisar et al., [21] in Pakistan, no significant difference was seen when the genders were compared for the diabetes myths.
In our study, we found that religion was an important factor. Muslims had more myths as compared to the Hindus, which indicated a lack of knowledge among the Muslim population. This fact should be taken in to consideration when plans are made for information, education and communication (IEC) activities. In another study which was done by Rai M and Kishore J [19], a similar prevalence of the myths were seen in both the religions.
For most of the misconceptions, there was no significant difference among the different age groups. The misconception about the duration of the treatment i.e. “The treatment should be stopped if the diabetes is controlled for a few months”significantly decreased with advancing age. This reflected that the young population was more aware about the long management of diabetes. The younger age groups comprised the learning age groups and so it was possible that they were more aware as compared to the higher age groups.
Surprisingly, for most of the myths, there was no significant difference in our study among the respondents with different standards of education. Probably, these beliefs were deep rooted in their minds where mere education was also not effective. In another study which was done by Sharaf et al., [22], education was a significant factor which affected the diabetes awareness. This may probably be due to the less number of participants from among the graduates and the above category.
In our study, for the most of the variables, we couldn’t find any association with the Diabetes mellitus misconceptions. Both males and females had similar beliefs, except for a few and so it signified that the awareness campaigns should include both males and females.
CONCLUSION
The misconceptions regarding the diabetes management in the general population, irrespective of the education and particularly among the Muslim community, were widespread. A majority of these misconceptions were diet and drug related. Printed health education materials which depict the dietary guidelines for diabetics and other diabetes management related information should be considered, where a medical team has to respond to a large number of patients in a limited time duration. The mass media like the newspapers and television can also serve the purpose well. Newspapers can have a column separately for the misconceptions and the truth which are related to diseases. The television can advertise the facts which are related to diabetes, which can reach even the small huts.
The misconceptions regarding the diabetes management in the general population, irrespective of the education and particularly among the Muslim community, were widespread. A majority of these misconceptions were diet and drug related. Printed health education materials which depict the dietary guidelines for diabetics and other diabetes management related information should be considered, where a medical team has to respond to a large number of patients in a limited time duration. The mass media like the newspapers and television can also serve the purpose well. Newspapers can have a column separately for the misconceptions and the truth which are related to diseases. The television can advertise the facts which are related to diabetes, which can reach even the small huts.