Serratia Marcescens- A Rare Opportunistic Nosocomial Pathogen and Measures to Limit its Spread in Hospitalized Patients
Ashish Khanna1, Menka Khanna2, Aruna Aggarwal3
1 Assistant Professor, Department of Microbiology, SGRDIMSR, India.
2 Associate Professor, Department of Pathology, SGRDIMSR, India.
3 Professor and Head, Department of Microbiology, SGRDIMSR Sri Guru Ram Das Institute of Medical Sciences and Research, Amritsar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ashish Khanna, Assistant Professor, Department of Microbiology, SGRDIMSR, 538, Basant Avenue Amritsar-143001, India.
Phone: 9465128936, 0183- 2562919
E-mail: ashish_538@yahoo.co.in
Background: In November 2011, 6 patients who were in the ICU of the Sri Guru Ram Dass Institute of Medical Sciences and Research acquired an infection which was caused by Serratia marcescens. We investigated the cause of the increase in frequency of the isolation of Serratia marcesens from hospitalized patients.
Methods: Various samples from patients and environmental sources, which were collected from the ICU of Sri Guru Ram Das Institute of Medical Sciences and Research during the 6 month period from November 2011 to April 2011, were included in the study. The isolates from the patients and the surrounding environmental sources were examined by using standard techniques. Further, the isolates of Serratia marcescens were identified, depending upon their biochemical and morphological characteristics.
Results: Seven isolates of Serratia marcescens were identified (six from the patients in the ICU and one from the soap dispenser in the ICU) among a total of 327 isolates from the clinical samples and 84 isolates were identified from the environmental sources in the ICU.
Discussion and Conclusion: An outbreak of the Serratia marcescens infection in the ICU was traced to the extrinsic contamination of the soap dispenser in the ICU, as after the removal of the dispenser, no further case occurred.
Serratiamarcescens, Nosocomial infection, Imipenem
INTRODUCTION
Serratia marcescens is an opportunistic, gram negative, nosocomial pathogen which belongs to family, Enterobacteriaceae. It was discovered by Bizio, an Italian pharmacist, in 1819, when he identified it as a cause of the bloody discolouration on cornmeal mush. He named the organism in honour of the Italian physicist, Serratia who invented the steam boat and marcescens, which is the latin word for ‘decaying’, as the bloody discolouration on cornmeal disappeared quickly. Serratia marcescens was originally considered to be an innocuous, non pathogenic, saprophytic water organism and it was often used as a biological marker because of its easily recognizable red colonies [1].
Intensive care units are often involved in the epidemics of the colonization and the infection with Serratia marcescens. The important reservoirs in epidemics are the digestive tract, the respiratory tract, the urinary tracts and the perineum of neonates and the artificial nails of adults and health care workers. Medical equipment, lotions, antiseptics, medications, blood products and sinks have also been described as the sources of epidemics. Serratia marcescens accounts for only 1-2% of the nosocomial infections which are mostly confined to the respiratory tract, the urinary tract, surgical wounds and soft tissues. Meningitis, which is caused by Serratia marcescens, has been reported from the paediatrics wards. In persons who are addicted to heroin, it causes endocarditis and osteomyelitis. In urinary tract infections, 30-35% of the patients are asymptomatic and most of the patients have a history of instrumentation. The mortality rate is very high in the nosocomial blood stream infections and in meningitis and endocarditis which are caused by the infection with Serratia. Some strains of Serratia are capable of producing a pigment which is known as prodigiosin, which ranges in colour from dark red to pink, depending on the age of the colonies. An important characteristic of Serratia marcescens is its ability to produce a beta lactamase which confers resistance to the broad spectrum, beta lactum antibiotics, which often complicates the therapy. The main risk factors for bacteraemia/sepsis which is caused by Serratia is hospitalization, placement of intravenous catheters, intraperitoneal catheters and urinary catheters and prior instrumentation of the respiratory tract [2–5]. Serratia marcescens causes both opportunistic and nosocomial infections. The objective of our study was to define the extent of the problem, identify the source and the risk factors and to implement control measures.
MATERIALS AND METHODS
Various samples from patients and environmental sources, which were collected from the ICU of Sri Guru Ram Das Institute of Medical Sciences and Research during the six month period from November 2011 to April 2011, were included in the study. The isolates were obtained from various samples like blood, urine and pus and environmental cultures were obtained from numerous surfaces which included walls, floors, corners, door handles, shelves sinks, soap dispensers, ventilators, stethoscopes and other medical equipments. The isolates were processed by standard laboratory methods and their susceptibility to the antimicrobial agents was performed as per the Clinical Laboratory Standard Institute guidelines [6,7]. After the first case of Serratia marcescens was identi- fied in the ICU, surveillance cultures such as pharyngeal swabs, rectal swabs, sputum and stool cultures were obtained from all the patients, to trace the source/ reservoir of the infection. Keeping the human carriage possibility in mind, the hands of the health care workers and the other auxillary staff were also checked. The bottles of saline which were used for the dilution of soap /disinfectants were also either swabbed or cultured.
Further, the isolates of Serratia marcescens were identified, depending upon their biochemical and morphological characters. The isolate producing, late lactose fermenting colonies with red pigment were subjected to further biochemical tests. Gram staining showed that they were gram negative bacilli which were catalase positive and oxidase negative. The organisms were motile and they showed DNAse and gelatinase production. The other biochemical tests were urease, hydrogen sulphide, arabinose and lactose fermentation which were negative and the citrate, lysine and the ornithine decarboxylase tests were positive. (arabinose fermentation is shown by the Serratia liquefaciens group.) [6].
RESULTS
During the 6 months period from November 2011 to April 2012, 327 isolates were identified from the clinical samples and 84 isolates were identified from the environmental/surveillance samples. [Table/Fig-1] Seven isolates of Serratia marcescens were identified among the above isolates. All the 7 isolates were obtained from the ICU( 6 from the patients and 1 from the environmental source) in the month of November only ,within 15 days duration. The first isolate was obtained from a patient who was admitted with chest pain which was caused by pneumonia. The sputum culture at the time of admission contained normal oral flora, but the bronchial wash on the third day revealed Serratia marcescens in the pure cultures.
Showing the frequency of isolation of common isolates from clinical samples and environmental sources
| Common Isolates | From Clinical samples | From Environmental sources |
| Escherchia Coli | 128(39.1) | 17(20.2) |
| Pseudomonas | 55(16.8) | 14(16.7) |
| Klebsiella pneumonia | 40(12.2) | 15(17.9) |
| Acinetobacter species | 31(9.5) | 6(7.4) |
| Citrobacter species | 17(5.2) | - |
| Staphylococcus aureus | 10(3.1) | 5(6.0 |
| CONS | 16(4.9) | 15(17.8) |
| Proteus | 9(2.8) | 9(10.7) |
| Serratia | 6(1.8) | 1(1.2) |
| Candida | 15(4.6) | - |
| Enterrococci | - | 2(2.4) |
| Total | 327 | 84 |
During the next 7 days, 5 more patients from the same ICU showed signs of infection with Serratia marcescens. All the five cases were immunocompromised (one patient was a case of diabetes with hypertension with hemiparesis, the second case was of meningitis, two cases were of Chronic Myeloid Leukaemia (CML) which were on chemotherapy and the fifth patient was a case of burns. In 5 cases, Serratia marcescens was obtained from urine and in one case, it was obtained from the pus samples from the wounds. All the 4 cases of UTI were catheterized. One isolate of Serratia marcescens was isolated from a soap dispenser. The usual large number of medical and paramedical staff were in attendance in the ICU and so the exact source of the infection among the health care workers was not identified. Antibiotic sensitivity tests revealed the pattern of susceptibility to the commonly used antibiotics like piperacillin/tazobactum, imipenem and ertapenem and the pattern of resistance to the aminoglycosides [Table/Fig-1 & 2], [Table/Fig-3 & 4]. All the seven isolates showed pigment production [Table/Fig-3]. Concomitant factors /other diseases were also present in all the six patients. All the patients responded well to imipenem and they recovered fully.
Antibiotic Senstivity pattern of isolates of SerratiaMarcescens
| Antibiotic | No of sensitive isolates | No of resistant isolates | % age Resistance |
| Ampicillin | 4 | 3 | 42.9 |
| Gentamycin | 1 | 6 | 85.7 |
| Amikacin | 2 | 5 | 71.4 |
| Cefotaxime | 2 | 5 | 71.4 |
| Ciprofloxacin | 6 | 1 | 14.3 |
| Colistin | 7 | - | - |
| Imipenem | 7 | - | - |
| Ertapenem | 6 | 1 | 14.3 |
| Piperacillin/Tazobactum | 6 | 1 | 14.34 |
| Ceftazidime | 4 | 3 | 42.9 |
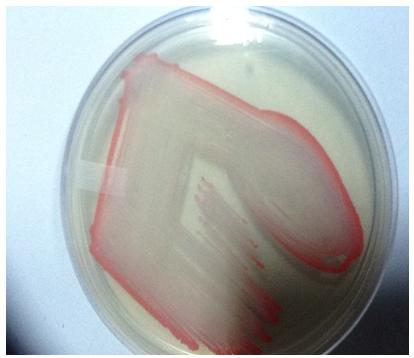
Showing the growth of Serratia marcescens on Nutrient Agar having red discolouration(due to production of pigment–Prodigiosin)
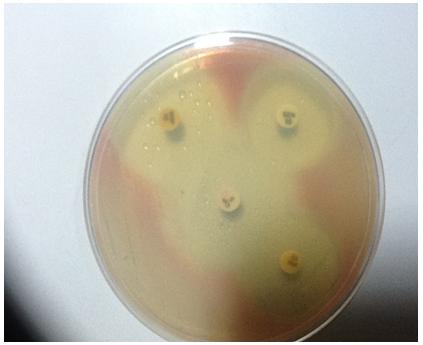
Showing the succeptibility of Serratia marcescens to various antibiotics on muller hinton agar
DISCUSSION AND CONCLUSIONS
Serratia marcescens, a motile, gram negative bacillus, which has been classified as a member of the family, Enterobacteriaceae, is widespread in the environment, but it is a rare cause of human disease. The Serratia species are occasionally recognized as a cause of hospital acquired infections such as urinary tract infections, respiratory tract infections and wound infections. The major factors that are involved in the development of the Serratia infection include contamination of the respiratory equipment and poor catheterization techniques. Most of the outbreaks have been reported from the paediatrics ward. The crude mortality in the nosocomial blood stream infections which are caused by Serratia is 26%, but in case of the urinary tract infections, the mortality is very low. Moreover, more than 90% of the cases of urinary tract infections are caused by the instrumentation [8,9]. In our study also, the patients developed the infection upon hospitalization and instrumentation (as all the patients had a history of instrumentation, either urinary catheterization or placement of the endotrachael tube for ventilation).
This study emphasized the opportunistic nature of Serratia marcescens, as this organism does not cause primary invasive diseases. But it produces an infection when it gains access to a suitable compromised host. The contributory factors for the spread of the hospital acquired infections include inadequate infection control practices which are coupled with the growing range of the modern medical procedures. The present outbreak involved 6 patients; 5 cases were due to cross contamination from the cases of respiratory infections which involved Serratia marcescens. The soap dispenser which was infected with Serratia was removed from the ICU and this probably helped in limiting the spread of the infection. A similar spread of the infection through soap dispensers, which was caused by Serratia marcescens in hospitalized patients as a result of inadequate hand hygiene, has been reported by others also [10,11]. Moreover, the adherence of strict hand hygiene compliance with the use of alcohol based rubs by the health care workers also helped in the containment of the infection. Another study which was done by Mcneal et al., also demonstrated the effectiveness of the alcohol based hand antiseptic, as they were able to remove pathogens from 80% of the health care workers [12]. The usual large number of medical and paramedical staff were in attendance in the ICU and so the exact source of the infection among the health care workers was not identified.
Troillet et al., reported imipenem resistance in 11% of the clinical isolates of Serratia species [13]. Another study showed that the Serratia marcescens isolates were sensitive to imipenem, but the resistance to meropenem was high. Thus, their susceptibilities to the antimicrobials may differ in a manner that is dependent on whether these antibiotics were previously used in the units [14]. But in our study, as the organism was highly sensitive to most of the antibiotics, all the cases were successfully treated with imipenem. The isolates were not sent for genotyping, as the spread was controlled/ limited to a small (six) number of cases, with no recurrence upto 6 months. (no evidence of a further transmission or environmental persistence of Serratia marcescens was seen over a six months period).
On the day of the isolation of Serratia marcescens from the ICU , an extensive, environmental, microbiological sampling was done. Swabs were taken from numerous surfaces which included walls, floors, corners, door handles, shelves, sinks, soap dispensers, ventilators, sthethoscopes and other medical devices. Keeping the human carriage possibility in mind, the hands of the health care workers and the auxillary staff were also checked. The bottles of saline which were used for dilution and the soap and disinfectants were either swabbed or cultured. Extensive sanitation procedures were started and glove usage was encouraged among the staff. The water and air filters were routinely serviced and renewed. Sometimes, to limit the spread of the infection, strict measures like nurse cohorting and closure of the ward to new admissions were taken. The practice of the same health care worker assisting in different wards like various ICUs and neonatal wards, also helps in the dissemination of the infection between different wards. Surveillance cultures should be carried out for a minimum of 6 months, as repeat outbreaks of the Serratia infection has been reported [15]. For the future outbreak control measures, every hospital should focus not only on the patients, but also on the mothers of the paediatric patients and the health care workers. The waterless alcohol based antiseptics are more effective than the antimicrobial soaps in eliminating the pathogen from the hands. The introduction of alcohol based handrubs have increased the hand hygiene compliance, as only less time is required for their use. Although genotyping has no role in the therapy, the isolates should be sent for genotyping for epidemiological purposes, if such facilities are available. Molecular assays allow an early aetiological diagnosis which is supported by epidemiological links and this helps in the containment of the spread of Serratia marcescens [16]. But these assays are not available in the small laboratories in a resource constrained country like India and so, other affordable methods like biotyping, bacteriocin typing, resistotyping and serotyping should be explored. This study showed the importance of the hygiene precautions, especially at high risk places like the ICU in a hospital setting.
[1]. Merlino CP, Bartholomeo Bizios letter to the most eminent priest, Anggelo Bellani, concerning the phenomenon of the red coloured polentaJ Bact 1924 9:527 [Google Scholar]
[2]. Yoon HJ, Choi JY, Park YS, Kim CO, Kim JM, Yong DE, Outbreaks of Serratia marcescens bacteriuria in a neurosurgical intensive care unit of a tertiary care teaching hospital: A clinical, epidemiological and laboratory perspectiveAm J Infect Control 2005 33:595-601. [Google Scholar]
[3]. Casolari C, Pecorari M, Fabio G, Cattani S, Veturelli C, Piccinini L, A simultaneous outbreak of Serratia marcescens and Klebsiella pneumonia in a neonatal intensive care unitJ Hosp Infect 2005 61:312-20. [Google Scholar]
[4]. Stewart Greco VS, Brown EE, Parr C, Kalab M, Jacobs MR, Yomohovian RA, Serratia marcescens strains implicated in adverse transfusion reaction form biofilms in platelet concentrates and demonstrate reduced detection by automated culturesVox Sang 2012 April 102(3):212-20. [Google Scholar]
[5]. Crivaro V, Bagattini M, Salza MF, Raimondi F, Rossano F, Triassi M, Risk factors for extended spectrum beta lactamase producing Serratia marcescens and Klebsiella pneumoniae acquisition in a neonatal intensive care unitJ Hosp Infect 2007 67(2):135-41. [Google Scholar]
[6]. Collee JG, Miles RS, Watt B, Tests for the identification of bacteria. In :Collee JG , Fraser AG, Marmion BP, Simmons A, editorsMackie and Mac Cartney practical medical microbiology 1996 14thEdinburghChurchill Livingstone:151-79. [Google Scholar]
[7]. National Committee for Clinical Laboratory Standards (2000)Performance standards for antimicrobial susceptibility testing-Ninth information supplement:M100-S10. NCLLS. Wayne A, USA [Google Scholar]
[8]. Mlynarczyk A, Mlynarczyk G, Pupek J, Bilewska A, Kawecki D, Luczak M, Serratia marcescens isolated in 2005 from clinical specimens from patients with diminished immunityTransplant Proc 2007 Nov 39(9):2879-82. [Google Scholar]
[9]. David MD, Weller TMA, Lambert P, Fraise AP, An outbreak of Serratia marcescens in the neonatal unit: a tale of two clonesJ Hosp Infect 2006 May 63(1):27-33. [Google Scholar]
[10]. Buffet-Bataillon S, Rabier V, Betremieux P, Beuchee A, Bauer M, Pladys P, Outbreak of Serratia marcescens in a neonatal intensive care unit: contaminated unmedicated liquid soap and risks factorsJ Hosp Infect 2009 72(1):7-22. [Google Scholar]
[11]. Rabier V, Bataillon S, Jolivet-Gougeon A, Chapplain JM, Beuchee A, Betremieux P, Hand washing as a source of neonatal Serratia marcescens outbreakActaPaediatr 2008 97(10):1381-85. [Google Scholar]
[12]. McNeil SA, Foster CL, Hedderwick SA, Kauffman CA, Effect of hand cleansing with antimicrobial soap or alcohol- based gel on microbial colonization of artificial fingernail worn by health care workersClin Infect Dis 2001 32:367-72. [Google Scholar]
[13]. Troillet N, Carmeli Y, Venkataraman L, De Girolami P, Samore MH, Epidemiological analysis of imipenem resistant Serratia marcescens in hospitalized patientsJ Hosp Infect 1999 42:37-43. [Google Scholar]
[14]. Lefort A, Righi S, Jaureguy F, Begue T, Robineau M, Bouchaud O, Serratia marcescens prosthesis infection successfully treated with meropenem after imipenem failureJ Infect 2005 51:45-47. [Google Scholar]
[15]. Fleisch F, Zimmermann-Baer U, Zbinden R, Bischoff G, Arlettaz R, Waldvogel K, Three consecutive outbreaks of Serratia marcescens in a neonatal intensive care unitClin Infect Dis 2002 34(6):767-73. [Google Scholar]
[16]. Adamson V, Mitt P, Pisarev H, Metsvaht T, Telling K, Naaber P, Prolonged outbreak of Serratia marcescens in Tartu University Hospital : a case control studyB M J Infect Dis 2012 Oct 12(1):281 [Google Scholar]