Cigarette smoking has become a common tendency worldwide. In general, tobacco is consumed by approximately 1.3 billion of the world’s population [1].
While tobacco use is rising globally, the epidemic of tobacco related diseases has just begun. Most of tobacco’s damage to the human health does not become evident until years or even decades after the onset of its use. While tobacco use is the leading cause of preventable dealth in the world [2] but this epidemic can be stopped by proper measures.
Tobacco, especially its content of nicotine, is a drug that has various deleterious effects besides having seductive effects and a dangerous risk of dependence. Many of the health effects of smoking depend on the exposure history, which includes the age at which the smoking began, the number of cigarettes which were smoked per day, the degree of inhalation, and the cigarette characteristics such as the tar and the nicotine content [3–5].
Besides the various tobacco related diseases, smoking has been associated with its effect on the senses, which includes the sense of hearing. The current smokers were 1.69 times as likely to have a hearing loss as the non-smokers. This relationship remained for those without a history of occupational noise exposure and in analyses which excluded those with non-age-related hearing loss [6]. Meta analysis studies which were done in Japan and Korea also came with similar evidences of a positive association between smoking and hearing loss [7,8]. The Framingham 33 and Baltimore studies 34 didn’t find any connection between hearing loss and smoking. Smoking may accelerate the age related hearing loss (presbycusis), as was demonstrated in various studies [7,9].
An interaction between smoking and occupational noise was reported, whereby the deleterious effect of the noise exposure was exacerbated by smoking [10], while the recent publications reported no interaction, thus indicating that smoking affected the hearing loss independently [11,12].
MATERIALS AND METHODS
The present hospital based, cross-sectional study was conducted in the Out Patients Department of Otorhinolaryngology, Jawaharlal Nehru Medical College, AMU, Aligarh (Uttar Pradesh). The participants were classified as either smokers (i.e. who had smoked or were current smokers) and non-smokers (i.e. who have/had never smoked). The test group consisted of male smokers (n=108) of ages between 20-60 years (mean age=37.45 years). The age matched control group (n=40) comprised of subjects who had never smoked (mean age=41.35 years).
Both the smokers and the non-smokers were interviewed by using a preformed questionnaire. The smoking was ascertained, based on the following questions: ‘Have you ever smoked?’ and ‘Do you smoke? and also on the duration of smoking and the number of bidis/cigarette s which were consumed per day. All the smokers with a history of ototoxic drug use, diabetes mellitus, hypertension, any kind of hearing loss, severe or frequent ear infections, ear surgery, a head injury which was associated with unconsciousness, familial deafness, an exposure to noise (occupational noise or non-occupational noise such as amplified music and participation in war, hunting, etc.) were excluded from the study. Both the test cases and the controls were chosen randomly on the basis of inclusion and exclusion criteria. All the subjects participated voluntarily in the study and an informed consent was obtained from each one.
The hearing tests were carried out in a sound proof room in the OPD of the Otorhinolaryngology Dept. The hearing examination included an otoscopic evaluation, a screening tuning fork test, and pure tone air-conduction and bone conduction audiometry.
AUDIOMETRY
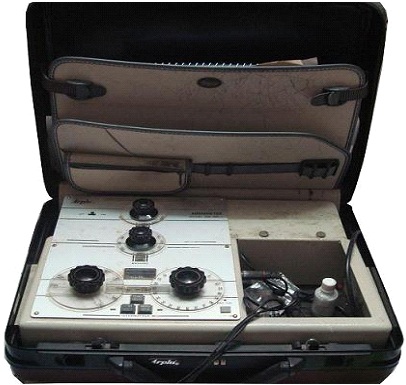
Audiometry was done by using an ARPHI’S series 500 Portable Audiometer by an experienced audiologist, who was unaware of the subject’s smoking status. The basic hearing test included pure tone audiometry. The range of the frequencies which were tested was 500-6000 Hz. The audiometric analysis was done to assess the degree and the type of the hearing loss. The instrument was regularly calibrated before use. Presently, the audiometer was calibrated according to the ISO 389 (1985).
By using the audiometric data, the hearing loss was defined as a pure tone average (PTA) of the thresholds at 500, 1000, 2000 and 4000 Hz which were greater than the 25-dB hearing level in the worser ear. The worser ear was chosen in order to include the subjects with at least 1 affected ear. The severity of the hearing loss was classified as mild (> 25 dB HL, AND ≤ 40 dB), moderate (>40 dB HL and ≤ 60dB), and severe (> 60dB), based on the pure tone average. The classification into conductive and sensorineural hearing impairment was also done on the basis of audiometry.
STATISTICAL ANALYSIS
The statistical analysis was carried out by using SPSS, version 16.0 and a p value of less than 0.05 was taken as significant.
RESULTS
On analyzing the audiometric data for the severity of the hearing impairment, it was observed that the mild form (26-40 db loss) was the most common (56.5%), while the severe type was the least common (2.8%) in the smokers [Table/Fig-1].
ARPHI’S series 500 Portable Audiometer.
Smoking was found to be statistically associated with the hearing impairment, with 65.7% of the smokers and 15% of the non smokers having hearing impairment. Also, as the age increased, the percentage of the affected individuals also increased, with greater percentages of the smokers being affected in comparison to the non smokers.
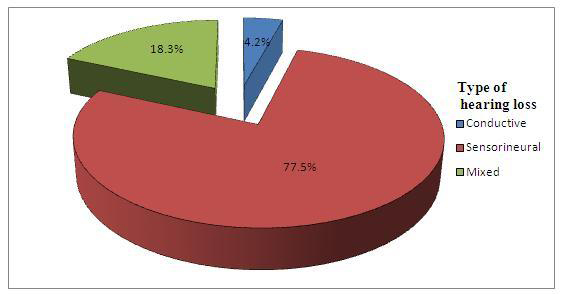
The most common type of hearing loss in the smokers was the sensorineural type (77.5%), followed by the mixed hearing loss (18.3%), while the mixed type was found in the non smokers.
The severity of the hearing loss in the smokers increased with an increase in the number of bidis/cigarettes which were smoked and the duration of smoking and this association was found to be significant statistically.
DISCUSSION
The age wise distribution of the subjects into smokers and non smokers has been depicted in [Table/Fig-2],[Table/Fig-3]. This corresponded to the working class in general, that was more likely to be exposed to tobacco smoking. [Table/Fig-4] shows that as the age increased, the percentage of the subjects with hearing loss also increased, both among the smokers and the non smokers. Also, with increasing age, the percentage of the smokers who had hearing loss was more than the percentage of the non smokers who had hearing impairment. Thus, it was seen that smoking was a contributing factor in the accelerating age related hearing loss.
Age composition of study groups
| Age Group (years) | Smoking status | Total |
|---|
| Smoker | Non-Smoker |
|---|
| No | % | No | % | No | % |
|---|
| 20-30 | 23 | 21.3 | 8 | 20.0 | 31 | 20.9 |
| 31-40 | 43 | 39.8 | 10 | 25.0 | 53 | 35.8 |
| 41-50 | 27 | 25.0 | 12 | 30.0 | 39 | 26.4 |
| 51-60 | 15 | 13.9 | 10 | 25.0 | 25 | 16.9 |
| Total | 108 | 100 | 40 | 100 | 148 | 100 |
Degree of hearing loss and smoking status X2 test, p value <0.05
| Smoking status | Affected subjects | Degree of Hearing Loss | No Hearing Loss | Total |
|---|
| 26-40 db | 41-60 db | >60 db |
|---|
| No | % | No | % | No | % | No | % | No | % |
|---|
| Smokers | 71 | 65.7 | 61 | 56.5 | 7 | 6.5 | 3 | 2.8 | 37 | 34.3 | 108 |
| Non Smokers | 6 | 15.0 | 6 | 15.0 | 0 | 0.0 | 0 | 0.0 | 34 | 85.0 | 40 |
Hearing loss in relationship with age
X2 test, p value<0.05
| Smoking Status | Age (in years) | Affected subjects | Hearing loss (in dB) | No Hearing loss | Total |
|---|
| No | % | 26-40 | 41-60 | >60 |
|---|
| Smoker | 20-30 | 6 | 26.1 | 6 | 0 | 0 | 17 | 23 |
| 31-40 | 29 | 67.4 | 27 | 1 | 1 | 14 | 43 |
| 41-50 | 21 | 77.8 | 19 | 1 | 1 | 6 | 27 |
| 51-60 | 15 | 100.0 | 9 | 5 | 1 | 0 | 15 |
| Total | 71 | 65.7 | 61 | 7 | 3 | 37 | 108 |
| Non smoker | 20-30 | 0 | .0 | 0 | 0 | 0 | 8 | 8 |
| 31-40 | 0 | .0 | 0 | 0 | 0 | 10 | 10 |
| 41-50 | 1 | 8.3 | 1 | 0 | 0 | 11 | 12 |
| 51-60 | 5 | 50.0 | 5 | 0 | 0 | 5 | 10 |
| Total | 6 | 15.0 | 6 | 0 | 0 | 34 | 40 |
Age and smoking had a multiplicative effect on the hearing impairment, which was in concordance with the findings of Noorhassim et al., [13]. For each age-decade, as the frequency increased, the percentage of the ears which were able to respond, decreased [14]. Smoking increased the risk of hearing loss and it was a contributory factor in age related hearing loss, which was also shown by other studies [6,15–17]. A multicentre study also reported that smoking was a risk factor for age related hearing loss [18].
The association between the smoking status and hearing loss has been depicted in [Table/Fig-2]. 65.7% of the smokers were affected and most of the subjects had hearing loss in the range of 26-40 db (56.5%). This association was found to be statistically significant, which pointed out that smoking was one of the contributing factors in accelerating age induced hearing loss.
The statistical interactions between smoking and hearing loss and the fact that smoking was associated with an increased risk of hearing loss were reported in the studies which were done by Cruickshanks [6], Itoh [15], Uchida [19], Nakanishi [20], Drettner [21] and Siegelaub [22] et al.,. A meta analysis study which was conducted in Japan also came with similar conclusions. This study had 15 observational studies, out of which the quality scores of 9 studies showed positive associations between smoking and hearing loss [23]. In contrast to the findings of this study, no correlation was found between hearing loss and smoking in the Framingham [24] and Baltimore studies [25].
The debate on the effect of tobacco smoking on the sensorineural loss has been controversial. It has been shown that the hearing loss which was associated with smoking was SNHL, with the damage mainly affecting the higher frequencies [26]. In the present study, a close association was found between smoking and the sensorineural hearing loss [Table/Fig-5], [Table/Fig-6], [Table/Fig-7]. Similar findings were also reported by Chung et al., [27]. A retrospective analysis of the data which were collected during the 1963 follow up of the NAMRL Thousand Aviator Study also showed a positive correlation between smoking and the chances of the development of the sensorineural hearing loss [28].
Type of hearing loss and smoking status
X2 test, p value < 0.05
| Smoking Status | Type of Hearing Loss | Total |
|---|
| Conductive | Sensorineural | Mixed |
|---|
| No | % | No | % | No | % | No | % |
|---|
| Smokers | 3 | 4.2 | 55 | 77.5 | 13 | 18.3 | 71 | 100 |
| Non Smokers | 0 | 0.0 | 2 | 33.3 | 4 | 66.7 | 6 | 100 |
| Total | 3 | 3.9 | 57 | 74.0 | 17 | 22.1 | 77 | 100 |
Chart showing degree of hearing loss in cases
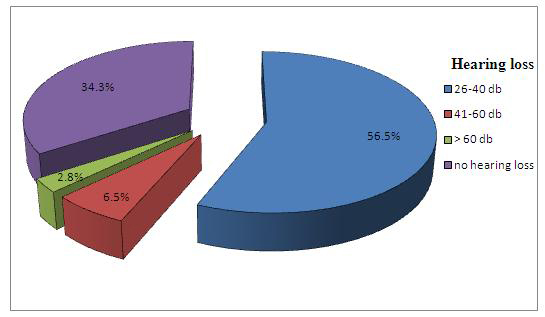
Chart showing type of hearing loss in cases
Sharabi et al., [18] also described that any type of hearing loss i.e. conductive, sensorineural, or the mixed type had a significantly higher incidence (p<0.0001) in the current and the past smokers as compared to that in the non smokers. But they also found that it was the conductive hearing loss which was more common than the sensorineural hearing loss in the current and the past smokers.
In the current study, the effect of the quantity of bidis/cigarettes which were smoked [Table/Fig-8] and the duration of smoking [Table/Fig-9] were found to be statistically associated with the hearing loss. A similar finding was illustrated by Sharabi et al., [29]. They observed that the prevalence of the hearing loss was significantly higher in the smokers who smoked more than 20 cigarettes per day than in those who smoked less than 20 cigarettes per day, but when the age was taken into consideration, this was not found to be statistically significant. Similar reports were also made by Uchida et al., [19], Mizoue et al., [11]. and Nomura et al., [7].
Hearing loss in relation to number of bidi/cigarette consumed
X2 test, p<0.05
| Number of Cigarette/bidi Per day | Hearing Impairment | No Hearing Impairment | Total |
|---|
| 26-40 db | 41-60 db | >60 db |
|---|
| No | % | No | % | No | % | No | % | No | % |
|---|
| 1-12 | 2 | 14.3 | 0 | 0.0 | 0 | 0.0 | 12 | 85.7 | 14 | 100 |
| 13-24 | 15 | 51.7 | 0 | 0.0 | 0 | 0.0 | 14 | 48.3 | 29 | 100 |
| 25-36 | 25 | 65.8 | 2 | 5.3 | 1 | 2.6 | 10 | 26.3 | 38 | 100 |
| >36 | 19 | 70.4 | 5 | 18.5 | 2 | 7.4 | 1 | 3.7 | 27 | 25.0 |
| Total | 61 | 56.5 | 7 | 6.5 | 3 | 2.8 | 37 | 34.3 | 108 | 100 |
Hearing loss in relation to duration of smoking
X2 test, p<0.05
| Duration of smoking (years) | Hearing loss | No Hearing loss | Total |
|---|
| 26-40 db | 41-60 db | > 60 db |
|---|
| No | % | No | % | No | % | No | % | No | % |
|---|
| <5 years | 1 | 14.3 | 0 | 0.0 | 0 | 0.0 | 6 | 85.7 | 7 | 100 |
| 5-10 years | 8 | 34.8 | 0 | 0.0 | 0 | 0.0 | 15 | 65.2 | 23 | 100 |
| 11-20 years | 19 | 52.8 | 1 | 2.8 | 0 | 0.0 | 16 | 44.4 | 36 | 100 |
| 21-30 years | 24 | 92.3 | 1 | 3.8 | 1 | 3.8 | 0 | 0.0 | 26 | 100 |
| >30 years | 9 | 56.2 | 5 | 31.2 | 2 | 12.5 | 0 | 0.0 | 16 | 100 |
So, as the dose of the smoking increased i.e. as the number of cigarettes or bidis which were smoked increased, the exposure of the body and the inner ear, in particular to nicotine, also increased, resulting in side effects, which included hearing impairment. Smoking, as a hearing hazard, becomes more prominent as the duration of the smoking increases [28,16,30]. Similar findings were also seen in various studies, which showed that as the number of cigarettes and the years of exposure increased, the risk of the hearing impairment also increased [6, 13, 20].
Various mechanism has been proposed by which tobacco smoke may affect the hearing. Cigarette smoking may affect the hearing through the direct ototoxic effect of nicotine on the cochlea [31–33]. As smokers are constantly exposed to the levels of carbon monoxide in the range of 500 to 1,500 parts per million [34], it has been suggested the carbon monoxide in tobacco smoke causes a rise in the carboxyhaemoglobin levels in smokers, which may in turn reduce the oxygen which is available for the organ of Corti [35, 36], resulting in a damage to the hair cells which are sensitive to oxygen [36].
One of the mechanisms through which the toxic chemicals in cigarettes may have an effect on hearing, is by causing damage to the anti oxidative mechanisms or to the vasculature which supplies the auditory system [37].
Smoking reduces the blood supply due to the vasospasms which are induced by nicotine, the atherosclerotic narrowing of the blood vessels and by thrombotic occlusions. Therefore, at all the measured frequencies, the percentage of the loss was greater for the smokers and it was the greatest at the higher frequencies [38].
The atherosclerotic effects may be accounted for as an intermediator between smoking and the hearing loss, because the literature has suggested that smoking is an independent risk factor for atherosclerosis, which in turn may affect the vasculature which supplies the auditory system [6, 39, 26].
CONCLUSION
There have been different views on the effects of smoking on the hearing abilities. Also, most of the studies had been done in the western population, with some studies favouring it, while some hadn’t found any association. The current study found the positive correlation of smoking and its various aspects with respect to the hearing status. This study was unique in the sense that it is conducted in Indian poulation (Utter Pradesh, India.) about which very little data was available regarding the smoking effects on the hearing status. We hope that, this study may pave the way for large scale studies which could be carried out further. Our findings may result in a future provision for an early screening in smokers for identifying any hearing impairment and for carrying out a timely intervention to correct it.