The Peak Expiratory Flow Rate (PEFR): the Effect of Stress in a Geriatric Population of Chennai- A Pilot Study
Sitalakshmi R1, Poornima K N2, Karthick N3
1 Assistant Professor, Department of Physiology, Sree Balaji Medical College and Hospital, Chromepet, Chennai, India.
2 Tutor, Department of Physiology, SRM Medical College Hospital and Research Center, Potheri, Kattankulathur, India.
3 Tutor, Department of Physiology, SRM Medical College Hospital and Research Center, Potheri, Kattankulathur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sitalakshmi R, Assistant Professor, Department of Physiology, Sree Balaji Medical College and Hospital, Chromepet, Chennai-600044, India.
Phone: 9952053207
E-mail: sitalakshmi.r@gmail.com
India is in a phase of demographic transition and it has acquired the label of “aging nation”, with 7.7% of its population being more than 60 yrs old. Among them, 81 % complain of increasing stress and psychosocial problems [1]. The elderly people are subjected to varying levels of insecurity and depression. A stressful lifestyle, along with environmental pollution and respiratory infections, is known to have adverse effects on the lung functions. PEFR, as a measurement of the ventilatory function, was introduced by Hadorn in 1942, and it was accepted in 1949 as an index of spirometry [2]. The peak expiratory flow emerges from the large airways within 100-102ms from the start of a forced expiration and it remains peaked for 10ms [3]. The normal peak flow is 450-550 L /min in adult males and it is 320-470 L/min in adult females. PEFR is the reflection of the functioning of the larger airways and any amount of stress/ infection/ inflammation in these airways causes adverse reactions. This study hypothesized that stress has a negative effect on the PEFR in elderly subjects.
This cross- sectional study included 68 subjects (males-29, females -35) who were randomly selected from the Sathyalok Charitable Home for the elderly in Chennai. Written informed consents were taken from them. A detailed respiratory history was taken and a clinical examination was done. The anthropometric indices (Ht, Wt, and BMI) were measured. A Perceived Stress Scale - questionnaire which contained both positive and negative statements, was administered [4]. The PEFR was measured by using the Clement Clarke mini peak flow meter after doing calibrations and the best of three readings were selected.
The subjects who were between 61- 91 yrs (who were divided into 3 groups), of both sexes and who were physically active (ambulant), were included in the study. Those with a H/O smoking / alcohol/primary complex/asthma/contact with open Pulmonary TB and those with a H/O recent surgery and a recent respiratory infection were excluded. The statistical analysis was performed by using the SPSS software. The data was expressed as mean±S.D. The independent ‘t’ test was used to compare the variables. A P value of < 0.05 was taken as statistically significant.
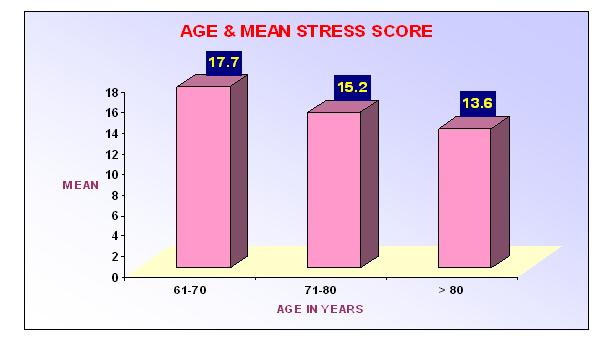
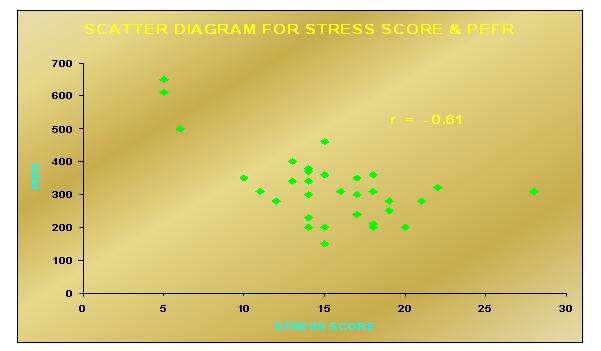
Among the 68 study subjects, 4 were excluded (in 2, we were unable to perform PEFR and 2 had a H/O recent respiratory infection). The study population was divided into 3 groups – Group I= 61-70yrs, Group II= 71-80 yrs and Group III= > 80 yrs. In our study, we found that with the advancement of age, the stress levels came down significantly. The mean stress level in Group I was 17.7, in Group II, it was 15.2 and in Group III, it was 13.6 The mean stress score (μ) of all the subjects was 15.78.The results have been shown in [Table/Fig-1]. There was a strong negative correlation between stress and the PEFR in our study (r = - 0.613), as has been shown in [Table/Fig-2]. We also found that as the age increased, there was a significant fall in the PEFR. The mean PEFR was μ=324.37 L/min. In the otherwise healthy lungs, the following factors determine the PEFR [5].
Stess Scores in the Three Age Groups
As age increases, mean stress score decreases significantly
F= 3.724, p=0.03(one –way ANOVA).
Correlation Between Stress And Pefr Strong negative correlation (r = -0.613) between stress and PEFR, p=0.000
The expiratory muscle strength, especially the abdominals
The dimensions of the intra and the extrathoracic airways
The maximum alveolar pressure reaching speed
The ability of the lung to undergo an elastic recoil
As the age advances, there is a specific reduction in all these parameters, leading to decreased lung functions, which has been demonstrated in various studies worldwide.
The stress questionnaire contained positive and negative statements where 0= no stress and 4 = maximum stress. (Scores of 0-10 = no stress, scores of 11-20 = mild stress, scores of 21- 30 = moderate stress and scores of >30 = severe stress).
In our study, as the stress increased, there is a significant fall in the PEFR, as was already shown by Smyth JM et al., [6]. The psychosocial variables (physical activities, social contacts, mood, and stressors) were strongly related to the PEFR, thus suggesting that they may play more important roles in the bronchial constriction than was previously thought. Stress reduces the PEFR through the cognitive-behaviour pathways or through its direct effect on the parasympathetic system or a combination of both [7]. A chronic stress-induced release of norephinephrine or related alterations in the alpha-adrenergic receptor sensitization may facilitate an adaptation to chronic stress [8].
The mean stress score in the elderly males was 13.2, whereas in the elderly females, it was much higher i.e 17.9.This showed that the elderly females were more stressful than the males, which was statistically significant. (p=0.000).The mean height of our study group was 157.6cms and the PEFR best correlated with height, as was already shown in the previous studies of Vijayan et al. With an increase in height, the PEFR also increased, which was statistically significant (p=0.001). In our study, the PEFR was greater in males than in the females, as shown by Puranik et al., 1995 [9].This can be attributed to the greater height, respiratory muscle strength and the maximal expiratory pressure in males than in females. After calculating the BMI, it was observed that those with Grade –I over weight was the most stressful group. This can be explained, based on the large amount of abdominal fat which hampered the descent of the diaphragm [10].
Our study concluded that elderly people, in today’s scenario, are subjected to increasing amounts of stress. The PEFR decreases with an increase in the age. The stress levels are more in females than in the male geriatric population. Our study concluded that stress was correlated negatively with the PEFR.
[1]. Ingle Gopal K, Nath Anita, Geriatric Health in India: Concerns and SolutionsIndian J Community Med 2008 October 33(4):214-18. [Google Scholar]
[2]. Jain SK, Kumar R, Sharma DA, Peak Expiratory flow rates (PEFR) in healthy Indian adults: A statistical evaluation-ILung India 1983 88-91. [Google Scholar]
[3]. Dikshit MB, Raje S, Agarwal MJ, Lung functions with spirometry: An Indian perspective- Peak expiratory flow ratesIndian J Physiol Pharmacol 2005 49(1):8-18. [Google Scholar]
[4]. Cole Stephen R, Assessment of differential item functioning in the Perceived Stress Scale-10J Epidemiol Community Health 1999 53:319-20. [Google Scholar]
[5]. Quanjer PH, Lebowitz MD, Gregg T, Miller MR, Pederson OF, Peak expiratory flow- Conclusions and recommendations of a working party of the European Respiratory SocietyEur Respir J 1997 10(24):2s-8s. [Google Scholar]
[6]. Smyth JM, Soefer MH, Hurewitz A, Kliment A, Stone AA, Daily psychosocial factots predict levels and diurnal cycles of asthma symptamatology and peak flowJ Behav Med 1999 Apr 22(2):179-93. [Google Scholar]
[7]. Campbell Tavis, Lavoie Kim L, Bacon Simon L, Scharf Deborah, Aboussafy David, Ditto Blaine, Asthma self –efficacy, high frequency heart rate variability, and airflow obstruction during negative affect in daily lifeInternational Journal of Psychophysiology Oct. 2006 62(1):109-14. [Google Scholar]
[8]. Ma S, Morilak DA, Chronic intermittent cold stress sensitizes the hypothalamic- pituitary-adrenal response to a novel acute stress by enhancing noradrenergic influence in the rat paraventricular nucleusJ Neuroendocrinol 2005 17:761-69. [Google Scholar]
[9]. Purranik BM, Kurhade GA, Kaore SB, Patwardhan SA, Kher JR, PEFR in pregnancy: A longitudinal studyIndian J of Physiol Pharmacol 1995 39:135-39. [Google Scholar]
[10]. Muralidhara DV, Bhat Ramesh, Some aspects of pulmonary functions in the underweight and overweight human subjectsThai Journal of Physiological Sciences 2007 Mar-Sep 20(1) [Google Scholar]