Intrapericardial Hemangioma: A Case Report
Nalini Gupta1
1 Department of Histopathology SRL (Religare) Reference Laboratory, Gurgaon, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nalini Gupta, C6/18 Arr Dee City IInd Floor, Sector 52, Gurgaon - 122001, Haryana, India.
E-mail: drnalinibansal@yahoo.com
Hemangiomas of the pericardium are very rare primary pericardial tumours. Very few cases of pericardial hemangioma have been reported in the literature till date. We are reporting a case of a 40 years old male who presented with the complaints of chest discomfort and palpitation on exertion, of 3 months duration. ECHO and Colour Doppler ECHO which were done, revealed a large heterogeneous mass which measured 7.6 × 7.1cms, which was possibly attached to the roof and the anterior surface of the left atria, which was possibly a myxoma. Based on the radiological findings, a diagnosis of left atrial myxoma was considered. However, intra operatively, an encapsulated mass was seen within the pericardium, which was successfully excised and sent for histopathology. The histopathological examination revealed an intrapericardial hemangioma. This case has been reported on account of its extreme rarity.
Hemangioma, Intrapericardial hemangioma, Myxoma
INTRODUCTION
The tumours of the pericardium can be primary or secondary. The secondary (metastatic) tumours are much more common than the primary tumours and they carry a poor prognosis. The most common primary pericardial neoplasm is a mesothelioma. The other tumours include teratomas, lipomas, lymphangiomas, etc. Hemangiomas of the pericardium have been rarely described in the literature.
Most of the cases are asymptomatic. The symptomatic patients present with dyspnoae, chest pain, pericardial effusion, etc. Surgical excision is the treatment of choice and a complete recovery is the rule. We have herein reviewed the clinical presentation and the differential diagnosis of this rare entity.
CASE REPORT
A 40 years old male presented with the complaints of chest discomfort and palpitation on exertion, of 3 months duration. He was normotensive, non diabetic and dyslipidaemic, with no family history of ischaemic heart disease. The 12 lead ECG showed showed a normal sinus rhythm. A 2 Dimension Colour Doppler ECHO which was done, revealed a large heterogenous mass which was seen in the left atria, which measured 7.6 X 7.1cms, which was attached to the roof and the anterior surface of the left atria. There was also trace mitral regurgitation, mild aortic regurgitation and trace tricuspid regurgitation. A Doppler study of the carotid which was done, revealed a normal picture. On physical examination, his pulse was found to be 86/ min and his BP was 130/80 mmHg. He had a normal trans venous pressure and he had no pallor, cyanosis, oedema, clubbing or jaundice. His respiratory system revealed bilateral, normal, vesicular breath sounds with no wheeze / rhonchi / crypts. A sternotomy which was done, revealed an encapsulated mass which was located within the pericardium, which extended from the anterior surface of the right atrium to the septum and crossed the aorta to the left side. The mass was removed in toto and it was sent for a histopathological examination.
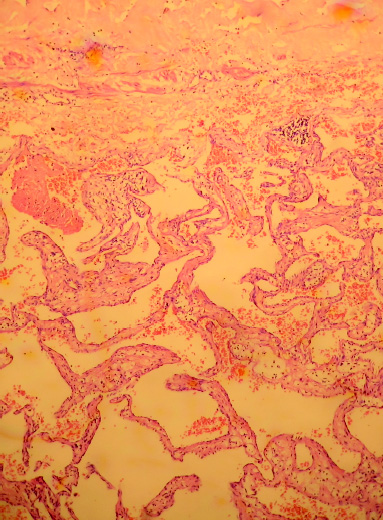
Grossly, the mass was single gray brown and it measured 10 × 8 × 3cms. Its outer surface was congested. Its cut surface was solid brownish and congested [Table/Fig-1]. The microscopic examination revealed a neoplasm which was composed of dilated vascular channels of varying sizes, which were filled with blood [Table/Fig-2]. Its periphery showed scanty firbomuscular tissue. Based on the above histomorphological features, a final diagnosis of an intrapericardial hemangioma was made. The patient was well during 6 months of the follow up.
Gross showing large encapsulated vascular tumor

Microscopic examination revealed large vascular spaces filled with blood lined by endothelial cells (H& E 10X)
DISCUSSION
The tumours of the pericardium can be primary or secondary. The primary pericardial tumours are much less common than the metastatic malignancies [1]. A majority of the metastatic tumours indicate a poor prognosis [2]. The primary pericardial neoplasms are rare lesions and they include the benign and the malignant histologic types. The primary pericardial massess include mesothelial cysts, mesotheliomas, teratomas, bronchogenic cysts, lipomas, lymphangiomas, angiosarcomas, etc. The hemangiomas which occur within the pericardium are very rare, with only few of such case reports being described in the literature. A case of a voluminous angioma which was adherent to the pulmonary artery [3] and another of an epicardial hemangioma [4] had been previously reported. A patient with a cavernous hemangioma which was located over the right ventricle free wall and which extended into the right ventricle out flow tract [5,6] was reported from Japan.
Most of the patients are asymptomatic and the tumour is discovered incidently. The symptomatic patients most commonly present with dyspnoae on exertion, but they may also present with chest pain, right sided heart failure, arrhythmias, pericarditis or pericardial effusion, syncope and sudden death [7,8]
In our case, the patient presented with complaints of chest discomfort and palpitation on exertion, of 3 months duration. ECHO revealed a large (7.6 X 7.1) sized, left atrial myxoma which was attached to the roof and the anterior septum surface of the left atria.
The patient was admitted for the removal of the mass. However, intraoperatively, the mass was large and encapsulated and it was seen within the pericardium to compress the RA, LA, and the SVC and to extend behind the aorta, to the left and to compress the LA appendages.
Histologically, most of the hemangiomas are classified as cavernous, capillary or arteriovenous [1].
Most of the case reports of cardiac hemangiomas describe surgical excision as the treatment of choice and a complete recovery has been the rule. In our case, the patient was well after 6 months of follow up [9].
The prognosis of the patients with surgically treated symptomatic lesions is excellent. The spontaneous regression of cardiac hemangiomas has been reported. The complications of the untreated cases can rarely cause bloody pericardial effusions, heart failure, syncope or sudden death [10].
Hemangiomas of the pericardium are very rare tumours, with only very few cases being reported in the literature. This report herein reviewed the clinical and the histopathological features of this rare neoplasm.
[1]. Grebenc ML, Christenson R, Burke A, Green C, Galvin J, Primary cardiac and pericardial neoplasms. A radiologic-pathologic correlationRadiographics 2000 20:1073-103. [Google Scholar]
[2]. Luk A, Ahn E, Vaideeswar P, Butany JW, Preicardial tumorsSemin Diagn Pathol. 2008 25(1):47-53. [Google Scholar]
[3]. Minutiello L, An intrapericardial angioma which adhered to the trunk of the pulmonary artery. The diagnostic value of computerised axial tomographyMinerva Cardioangiol 1996 44:319-23. [Google Scholar]
[4]. Caires G, Canada M, Couveia R, Aguiar C, Lino JS, Martins AP, Hemangiomas of the right ventricleRev Port Cardiol. 1997 16:561-67. [Google Scholar]
[5]. Ashino Y, Koike K, Okada S, Tanita T, Fujimura S, Nakada T, A case of a hemangioma of the heartKyobu Geka 1989 42:1119-21. [Google Scholar]
[6]. Harada H, Hirata T, Utoh J, Kunitomo R, Hara M, Kitamura N, A cardiac hemangioma of the right ventricle: the report of a caseJpn Thoracic Cardiovasc Surg. 1998 46:629-33. [Google Scholar]
[7]. Burke A, Johns JP, Virmani R, Hemangiomas of the heart; a cliniopathology study of ten casesAm J Cardiovasc Pathol. 1993 3:283-90. [Google Scholar]
[8]. Chao JC, Reihjes CN, Hwang MH, Cardiac hemangiomasSouth Med J. 1990 83:44-47. [Google Scholar]
[9]. Bizard C, Latremouille C, Jebara V A, Acar C, Fabiani J N, Deloche A, Cardiac hemangiomasAnn Thoracic Surg. 1993 56:390-94. [Google Scholar]
[10]. Omura K, Onishi T, Yamawaki K, Marbrouk A, Omar S, Kanzawa M et [Google Scholar]