Sarcoptic Mange: A Zoonotic Ectoparasitic Skin Disease
Kiran Madhusudhan Bandi1, Chitralekha Saikumar2
1 Associate Professor, Bharath University, Sree Balaji Medical College & Hospital, Chennai, India.
2 Professor, Bharath University, Sree Balaji Medical College & Hospital. Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kiran Madhusudhan Bandi 20, (Old No.12) Lynwood Avenue Mahalingapuram, Chennai-34 (India).
Phone: 9841434966
E-mail: brskiran@yahoo.in
A 56-year old man attended the Dermatology Outpatients Department with the complaint of a localized, extremely itchy, erythematous papular lesion of acute onset on the ventral aspect of the right thigh. The patient was referred to the Microbiology Lab for the microscopic detection of the fungal elements. The KOH mount from the skin scrapings showed no fungal elements, but it showed the mites of Sarcopetes scabiei mange. The Sarcoptic Mange is noteworthy because of the fact that it is a zoonotic disease which can easily be passed on to humans. A close contact with infested pet dogs was considered as the main predisposing factor in this case. The response to the antiscabietic treatment was dramatic.
Sarcoptic mange, Zoonotic ectoparasite, Sarcopetes scabiei mange, Sarcopetes scabiei var canis
INTRODUCTION
Sarcoptic mange (animal scabies, pseudo scabies, canine scabies) is a highly contagious skin disease which can affect a variety of wild, domestic and farmed animals. The Sarcopetes scabiei mange mite gets transmitted to humans on close contact with infected domestic animals, leading to intense pruritis and irritation due to the hypersensitivity reactions for the mites and their products [1]. The disease runs a prolonged course in humans who are known to have poor immune functions or in patients who are being treated with immuno-suppressants and in young children. The infestations, although they are typically self-limiting, can be intensely itching and bothersome. There are reported cases of Sarcoptic mange in humans that are not self-clearing and they require months of treatment to control them [2,3].
CASE REPORT
A 56-year old man attended the Dermatology Outpatients Department with a severely itching, localized skin lesion of 5 days duration, on the antero-lateral aspect of his right thigh. He was not an alcoholic or a smoker. The patient had no other medical complaints and he was not on any medication. He gave a H/o close physical contact with pet dogs.
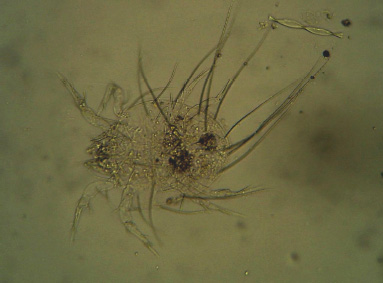
The patient was referred to the Microbiology Lab for the detection of the fungal elements. His cutaneous examination showed a well defined, 3 x 2.5cm sized, erythematous plaque with a papulo – vesicular eruption and minimal scaling. Skin scrapings were taken from the site of the lesion, they were treated with 10% KOH and examined for presence of fungal elements. The microscopic examination under low power revealed the absence of fungal elements. A 300–400mm sized, adult mite was seen and it was identified as the Sarcopetes scabiei mange mite on the basis of its morphology. This, along with the absence of the typical scabietic lesions, positive history of a contact with infected pet animals and the presenting site of the lesion, helped in the diagnosis of Sarcoptic mange in this patient [Table/Fig-1 & 2].
Papulo erythrematous rash on patient’s right thigh

Adult Sarcopetes scabiei mange mite under low power
The patient was treated with antiscabietic drugs. He was prescribed the topical 5% Permethrin cream, (overnight application from neck to toe), antihistamine tablets (-1HS/ SOS for 3 days) and tablet Ivermectin (2 doses at two weeks interval). He was advised to avoid close contact with his pet dogs and to get them treated by a veterinarian without delay to prevent a re-infection. The review of the patient after 1 month showed a complete disappearance of the lesion.
DISCUSSION
Sarcoptic mange is a serious ectoparasitic disease in many animals. Sarcoptes scabiei var cannis affects parts of the bodies of dogs which are devoid of hair, such as the head, chest, abdomen, neck, face, ears, elbow and the hocks. The papular lesions are intensely pruritic and they are associated with scaling, oozing, crusting and scab formation. There is a marked alopecia and weight loss. A secondary bacterial infection can occur, leading to severe morbidity in these animals.
The mite is transmissible to humans on close contact with infested animals. The animal scabies in humans presents with a totally different picture from that which is produced by the Sarcoptes scabiei var hominis (human itch mite) infection. Each species of the mite prefers one specific type of host and it does not live long or reproduce away from the preferred host [4–6]. So, humans are unlikely to develop full blown scabies from this source. The incubation period is shorter, the symptoms are transient and the infestation is self limiting. The lesions are seen more on the forearm, the lower chest, the abdomen, the thighs and the areas which are exposed to mites, when the affected animals are carried. The interdigital webs and the genitalia are usually spared. The characteristic deep, long burrows are not formed. These mites burrow into the skin to lay eggs for a short time, causing itching and intense irritation, which may get secondarily infected with pyogenic bacteria(eg) Streptococcus pyogenes or Staphylococus aureus, leading to post infective complications such as acute post streptococcal glomerulonephritis [7,8].
The adult female is approximately 0.3 x 0.4mm in size, while the male is smaller, around 0.25 x 0.2mm [6]. Sarcopetes scabei var canis belongs to the phylum-Arthropoda Class-Arachnida; Sub class-Acari; Order-Acarina; Family-Sarcoptidae Genus-Sarcoptes. Its developmental stages include the egg, larva, protonymph, tritonymph and the mite. Its body is roughly circular, convex dorsally and flattened ventrally. It has 4 pairs of legs and the 1st and the 2nd pairs bear suckers, while the 2 rear pairs have long trailing bristles. They have spur like claws and spine like projections on their dorsal surfaces. The surface of the female mite is covered with fine transverse striations and scales, which are of taxonomic value [9]. Over 15 different varieties or strains have been described in various hosts, although morphologically, they appear similar. Molecular studies have indicated clear physiological and genetic differences between the host strains.
The transmission from animal to animal is through direct contact or via fomites. The young and the poorly nourished animals are the most susceptible to the infection. The treatment in animals varies from medicated baths and Amirtaz dips, antibiotic injections or oral medications (Ivermectin) or a combination of these. To prevent a re-infection, it is generally advised to discard the brushes, combs, collars and the bedding of the affected animals or to wash these in a diluted bleach solution.
CONCLUSION
The human scabies infection is not rare in our setup, the predisposing factors being low socioeconomic conditions, overcrowding and poor hygiene [10]. The animal scabies in humans should be considered as a differential diagnosis for the itchy dermal lesions in those who give a H/o a direct contact with animals. The lesions of the animal scabies in humans can mimic various dermatological skin diseases such as dermatitis, herpitiformis, eczema, contact dermatitis, fungal infections and insect bites. The traditional tests which are used to diagnose scabies are less than 50% accurate. The current studies include, identifying the antibodies in individuals with active scabies by using recombinant antigens [11]. Epiluminescense microscopy and high resolution video dermatoscopy can help in diagnosing on observation of the “jet with contrail” pattern in the skin, which represents the mite and its burrow.
The prevention includes an early identification and a prompt treatment of the source animals .Care must be taken while they are being handled. Protective clothing such as gloves should be worn. The lesions in humans should be diagnosed and treated, keeping this ectoparasitic skin disease in mind.
[1]. ADVL Text Book and Atlas of Derm, Vol I-II edition by RG Valia and Ameet R. Valia [Google Scholar]
[2]. Medical Review: Michael J Sextan MD paediatrics; Alexander H Murrey, MD-FRCPC Dermatalogy [Google Scholar]
[3]. Taplin D, Porcelain SL, Meinking TL, The community control of scabies: a model which is based on use of the permethrin creamLancet 1991 337:1016-18. [Google Scholar]
[4]. Arlian LG, Biology, Host Relations and Epidemiology of S.ScabieiAnnu RW entomol 1989 34:139-61. [Google Scholar]
[5]. Charles Worth EN, Johnson JL, An epidemic of canine scabies in manArch Derm. 1974 110:572 [Google Scholar]
[6]. Davis DP, Moon RD, The dynamics of the swine mange: a critical review of the literatureJ Med Entomol. 1990 27:727-37. [Google Scholar]
[7]. Smith EB, Claypoole TF, Canine scabies in dogs and humansJAMA 1967 199:59-64. [Google Scholar]
[8]. Tropical Dermatopathology by Manoj Singh Nov 16,2004 1edMcGraw-Hill Professional [Google Scholar]
[9]. Manson’s Tropical Diseases (21st ed) by Gordon C. Cook and Alimuddin Zimla [Google Scholar]
[10]. Wong LC, Amega B, Connors C, The outcome of an interventional program for scabies in an indigenous communityMed J. Aust 2001 175:367-70. [Google Scholar]
[11]. Walton SF, Currie BJ, The Problems in Diagnosing Scabies, a Global Disease inHuman and Animal Populations:268-79. [Google Scholar]